Chronic kidney disease - causes, symptoms, treatment
Chronic kidney disease is not a disease, but a syndrome, that is, a similar condition that can occur with various diseases. In some cases, it is possible to make a diagnosis of chronic kidney disease, but it is worth understanding that this is not a nosological disease. Chronic kidney disease can be recognized in a patient only when impaired renal function has been observed for three months or more, or during this time there are signs of nephropathy, even with a normal glomerular filtration rate.
Chronic kidney disease causes
There are many reasons for the development of chronic kidney disease. The most common of them, which out of four cases in about three lead to the development of chronic kidney disease, are:
- High blood pressure (arterial hypertension). Poorly controlled or advanced hypertension most often leads to the development of chronic kidney disease. However, chronic kidney disease itself contributes to the development of hypertension. That is, blood pressure and the state of kidney function are interconnected. Moreover, nine out of ten patients at stages 3-5 of chronic kidney disease develop arterial hypertension.
- Diabetes. Quite often, with diabetes mellitus, so-called diabetic kidney damage develops, which ultimately leads to chronic kidney disease.
- Age-related decline in kidney function or aging of the kidneys. Almost all elderly people over 75 years of age have the first or second degree of chronic kidney disease. As a rule, if there are no concomitant diseases that affect kidney function, then chronic kidney disease does not develop beyond the second stage.
There are also other medical conditions that increase the risk of progression to chronic kidney disease. Such diseases include:
- Renal artery stenosis
- Glomerulonephritis
- Blockage of urine flow
- Polycystic kidney disease
- Chronic kidney infections
- Hemolytic uremic syndrome
- Kidney damage due to poisoning or drug poisoning
- Hyperlipidemia
- Urinary tract obstruction or urinary tract infection
- Acute renal failure
- Autoimmune diseases
- Systemic infections
- Hereditary burden
- Obesity
- Smoking and many, many other reasons.
Stages of CKD
- GFR (glomerular filtration rate) shows normal kidney function (>90), signs of nephropathy are observed.
- GFR 60-89 – moderate decrease in function against the background of identified kidney disease.
- GFR 45–59 (3A), 30–44 (3B) – a clear decrease in renal function with or without identified pathology. For example, older patients may experience decreased function without association with a specific disease.
- GFR 15–29 severe decline in kidney function.
- An GFR of less than 15 is called end-stage renal disease.
Chronic kidney disease symptoms
Kidney symptoms vary depending on the stage of chronic kidney disease. So, in the first and second stages of the disease, as a rule, the patient does not present any complaints and the syndrome is determined by laboratory tests. At the third stage, symptoms of general malaise begin to develop, which usually occur with any disease, so they cannot be called specific either. The patient may complain of fatigue, chronic fatigue, drowsiness, headaches, and so on. Subsequently, the patient may complain of:
- loss of appetite and weight loss,
- decreased performance,
- dryness and irritation of the skin, itching,
- pale skin,
- muscle spasms,
- swelling of the legs,
- swelling under the eyes,
- frequent urge to urinate.
In addition, chronic kidney disease is accompanied by one or several clinical syndromes with all the ensuing symptoms:
- anemia,
- azotemia,
- arterial hypertension,
- acidosis,
- electrolyte disturbances.
Diagnostics Diagnosis is made on the basis of clinical studies:
- Determination of glomerular filtration rate. This is one of the main studies. It should be taken into account that the absence of changes in glomerular filtration rate does not exclude the presence of chronic renal disease, since at the first stage it may be normal. That is, if the glomerular filtration rate is normal, but there is renal damage of any etiology for three or more months, then we are dealing with first-degree chronic kidney disease. However, a decrease in glomerular filtration rate for three months or more always indicates the presence of chronic kidney disease.
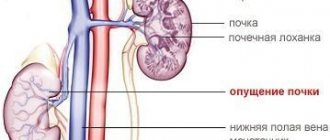
- Renal ultrasound is necessary to determine the condition of the kidneys, their function and the presence or absence of kidney damage.
- A general urine test is necessary to determine kidney function.
- Blood test to determine the presence of creatinine and monitor electrolyte levels.
To determine the root cause, as well as treat the primary disease, other additional tests and research methods may be prescribed.
Renal failure, diagnosis and treatment of renal failure in St. Petersburg
The main functions of the kidneys (removal of metabolic products, maintaining a constant water-electrolyte composition and acid-base state) are carried out by the following processes: renal blood flow, glomerular filtration and tubules (reabsorption, secretion, concentration ability). Not every change in these renal processes leads to severe impairment of renal function and can be called renal failure. Renal failure is a syndrome that develops as a result of severe disturbances of renal processes, leading to a disorder of homeostasis, and is characterized by azotemia, a violation of the water-electrolyte composition and the acid-base state of the body. Acute renal failure can occur suddenly as a result of acute, most often reversible, kidney disease. Chronic renal failure develops gradually as a result of progressive irreversible loss of functioning parenchyma.
Acute renal failure (ARF). Etiology, pathogenesis. The causes of acute renal failure are diverse: 1) impaired renal hemodynamics (shock, collapse, etc.); 2) exogenous intoxications (poisons used in the national economy and everyday life, bites of poisonous snakes and insects, medications); 3) infectious diseases (hemorrhagic fever with renal syndrome and leptospirosis); 4) acute kidney diseases (acute glomerulonephritis and acute pyelonephritis); 5) obstruction of the urinary tract; 6) arenal condition (trauma or removal of a single kidney).
Renal hemodynamic disorders and exogenous intoxications cause 90% of all cases of acute renal failure. The main mechanism of kidney injury in these two forms of acute renal failure is renal tubular anoxia. With these forms of acute renal failure, necrosis of the tubular epithelium, edema and cellular infiltration of interstitial tissue, and damage to the renal capillaries develop, i.e., necrotic nephrosis develops. In most cases, this damage is reversible.
Symptoms, course . In the initial period of acute renal failure, symptoms caused by shock (pain, anaphylactic or bacterial), hemolysis, acute poisoning, infectious disease come to the fore, but already on the first day a drop in diuresis is detected (less than 500 ml/day), i.e. a period develops oliguria-anuria, and homeostasis is already disturbed. In plasma, along with an increase in the levels of creatinine, urea, residual nitrogen, sulfates, phosphates, magnesium, potassium, the levels of sodium, chlorine and calcium decrease. The combination of humoral disorders causes increasing symptoms of acute uremia. Adynamia, loss of appetite, nausea, vomiting are observed already in the first days of oliguria-anuria. As azotemia increases (usually the level of urea increases by 0.5 g/l daily), acidosis, overhydration and electrolyte disturbances, muscle twitching, drowsiness, retardation of consciousness appear, and shortness of breath increases due to acidosis and pulmonary edema, the early stages of which are determined by x-ray. Characterized by tachycardia, expansion of the borders of the heart, dull tones, systolic murmur at the apex, and sometimes pericardial friction murmur. Some patients have arterial hypertension. Rhythm disorders are often associated with hyperkalemia: it is especially dangerous and can cause sudden death. With hyperkalemia of more than 6.5 mmol/l on the ECG, the T wave is high, pointed, the QRS complex widens, and the R wave may decrease. Heart blocks or ventricular fibrillation can result in cardiac arrest. Anemia persists during all periods of acute renal failure, leukocytosis is characteristic of the period of oliguria-anuria. Abdominal pain and liver enlargement are common symptoms of acute uremia. Death in acute renal failure most often occurs from uremic coma, hemodynamic disorders and sepsis. In acute renal failure, hypoisosthenuria is detected from the very beginning.
The protein content in the urine and the nature of the urinary sediment depend on the cause of acute renal failure. An increase in diuresis of more than 500 ml/day means a period of diuresis recovery. Clinical improvement becomes obvious, even after the onset of polyuria, not immediately, but gradually, as the level of azotemia decreases and homeostasis is restored. During the period of polyuria, hypokalemia (less than 3.8 mmol/l) with ECG changes (low T wave voltage, U wave, decreased S7 segment) and extrasystole is possible. By the time the residual nitrogen content in the blood normalizes, homeostasis is largely restored—the convalescent period. During this period, renal processes are restored. It lasts up to a year or more. However, the fate of patients is that a decrease in glomerular filtration and the concentrating ability of the kidneys remains, and in some, renal failure takes a chronic course, with associated pyelonephritis playing an important role.
The diagnosis is made on the basis of a sudden drop in diuresis as a result of one of the above reasons, an increase in azotemia and other typical disturbances of homeostasis. Anamnesis data, a decrease in kidney size in chronic glomerulonephritis and pyelonephritis, and identification of a chronic urological disease help differentiate from exacerbation of chronic renal failure or its terminal stage. In acute glomerulonephritis, high proteinuria is observed.
Treatment . From the first hours of the disease, pathogenetic therapy is indicated, the nature of which is determined by the cause that caused acute renal failure. First of all, it is necessary to carry out plasmapheresis, the volume of which is determined by the severity of the patient’s condition and the degree of intoxication. The removed plasma must be replaced with fresh frozen plasma or albumin solution. In case of hemodynamic disorders, anti-shock measures are indicated (replenishment of blood loss by transfusion of blood components, blood substitutes, intravenous drip administration of 100–200 to 400 mg of prednisolone). With ongoing hypotension (after replenishment of blood loss), intravenous drip administration of 1 ml of 0.2% solution of norepinephrine in 200 ml of isotonic sodium chloride solution is advisable. In case of acute poisoning, along with anti-shock therapy, measures are taken to remove the poison from the body (see Poisoning). In case of massive intravascular hemopysis, if the hematocrit is below 20%, a replacement blood (or plasma) transfusion is performed. If the cause of acute renal failure is bacterial shock, then in addition to anti-shock measures, antibiotics are prescribed. At the very beginning of the acute renal failure disease, a 10% solution of mannitol is administered intravenously at the rate of 1 g per 1 kg of the patient’s body weight. If anuria continues for 2–3 days, treatment with mannitol is not advisable. In the initial period of opyguria-anuria, diuresis is stimulated with furosemide (160 mg IV 4 times a day). If diuresis increases, then the use of furosemide is continued. Further therapy is aimed at regulating homeostasis. A diet that restricts protein and potassium should be high in calories with adequate amounts of carbohydrates and fats. The amount of fluid administered should exceed diuresis, as well as the amount of water lost through vomiting and diarrhea, by no more than 500 ml. This volume includes 400 ml of a 20% glucose solution with 20 units of insulin. In addition, for hyperkalemia, 10–20 ml of a 10% calcium gluconate solution and 200 ml of a 5% sodium bicarbonate solution are administered intravenously. Large quantities of sodium bicarbonate solution can be administered only after establishing the degree of acidosis and under control of blood pH.
Testosterone propionate 50 mg/day or 100 mg retabolil is administered intramuscularly once a week. Prescribing antibiotics is often necessary, but their dose is reduced by 2–3 times due to the limited excretion in batches. Streptomycin, monomycin, neomycin in conditions of anuria have a very pronounced ototoxic property, and they should not be used in acute renal failure. Continued oliguria and increasing symptoms of uremia are indications for transferring the patient to the hemodialysis department, where he can undergo extracorporeal cleansing using an artificial kidney or peritoneal dialysis.
Indications for hemodialysis or peritoneal dialysis are plasma urea levels more than 2 g/l, potassium levels - 6.5 mmol/l; decompensated metabolic acidosis and the clinical picture of acute uremia. Contraindications to hemodialysis: cerebral hemorrhages, gastric and intestinal bleeding, severe hemodynamic disorders with a drop in blood pressure. Contraindications to peritoneal dialysis are recent surgery on the abdominal organs and adhesions in the abdominal cavity.
Forecast. With timely and correct application of adequate treatment methods, most patients with acute renal failure recover and return to normal life.
Chronic renal failure (CRF). Etiology, pathogenesis. The most common causes of chronic renal failure are chronic glomerulonephritis, chronic pyelonephritis, nephritis in systemic diseases, hereditary nephritis, polycystic kidney disease, nephroangiosclerosis, diabetic glomerulosclerosis, renal amyloidosis, as well as urological diseases (bilateral or solitary kidney). The main pathogenetic mechanism of chronic renal failure is a progressive decrease in the number of active nephrons, leading to a decrease in the efficiency of renal processes, and then to impaired renal function. The morphological picture of the kidney in chronic renal failure depends on the underlying disease, but most often there is replacement of the parenchyma with connective tissue and wrinkling of the kidney.
Chronic kidney disease can last from 2 to 10 years or more before chronic kidney disease occurs. They go through a number of stages, the conditional identification of which is necessary for proper planning of treatment for both kidney diseases and chronic renal failure. When glomerular filtration and tubular reabsorption are maintained at normal levels, the underlying disease is still at a stage that is not accompanied by disturbances in renal processes. Over time, glomerular filtration becomes lower than normal, and the ability of the kidneys to concentrate urine also decreases; the disease enters the stage of disruption of renal processes. At this stage, homeostasis is still preserved (there is no renal failure yet). With a further decrease in the number of active nephrons and the glomerular filtration rate below 50 ml/min, the levels of creatinine in the blood plasma increase to more than 0.02 g/l and urea to more than 0.5 g/l. At this stage, conservative treatment of chronic renal failure is required. When filtration is below 10 ml/min, azotemia and other homeostasis disorders are steadily increasing, despite conservative therapy, and the end stage of chronic renal failure occurs, in which the use of dialysis is necessary.
With the gradual development of chronic renal failure, homeostasis slowly changes - the levels in the blood of not only creatinine and urea, but guanidine derivatives, sulfates, phosphates and other metabolites increase. When diuresis is maintained (polyuria is often observed), sufficient water is excreted, and the levels of sodium, chloride, magnesium and potassium in the plasma do not change. Constantly observed hypocalcemia is associated with impaired vitamin D metabolism and calcium absorption in the intestine. Polyuria can lead to hypokalemia. Metabolic acidosis is very often detected. In the terminal stage (especially when oliguria occurs), azotemia rapidly increases, acidosis worsens, hyperhydration increases, hyponatremia, hypochloremia, hypermagnesemia and especially life-threatening hyperkalemia develop. The combination of humoral disorders causes the symptoms of chronic uremia.
Symptoms, course. Patients complain of fatigue, decreased performance, headache, and loss of appetite. Sometimes they notice an unpleasant taste in the mouth, nausea and vomiting. The patient is pale, the skin is dry and flabby. Muscles lose tone, small muscle twitching, tremors of fingers and hands are observed. Sometimes there is pain in the bones and joints. Anemia develops, leukocytosis and bleeding appear. Arterial hypertension is often present, which is usually due to underlying kidney disease. The boundaries of the heart are expanded, its sounds are muffled, ECG changes are detected (sometimes they are associated with diokalemia). This stage can last several years. Conservative therapy makes it possible to regulate homeostasis, and the patient’s general condition often allows him to still work, but increased physical activity, mental stress, dietary errors, drinking restrictions, infection, and surgery can lead to deterioration of kidney function and worsening uremic symptoms.
When glomerular filtration is below 10 ml/min, conservative correction of homeostasis is impossible. This terminal stage of chronic renal failure is characterized by emotional lability (apathy is replaced by agitation), disturbance of night sleep, daytime sleepiness, lethargy and inappropriate behavior. The face is puffy, gray-yellow in color, the skin is itchy, there are scratches on the skin, the hair is dull and brittle. Dystrophy increases, hypothermia is characteristic. No appetite. The voice is hoarse. There is an ammonia smell from the mouth. Aphthous stomatitis occurs. The tongue is coated, the abdomen is swollen, vomiting and regurgitation are often repeated. Often diarrhea, foul-smelling, dark-colored stools. Anemia and hemorrhagic syndrome increase, muscle twitching becomes frequent and painful. With long-term uremia, pain in the arms and legs and bone fragility are observed, which is explained by uremic neuropathy and renal osteodystrophy. Noisy breathing is often due to acidosis, pulmonary edema, or pneumonia. Uremic intoxication is complicated by fibrinous pericarditis, pleurisy, ascites, encephalopathy and uremic coma.
The diagnosis is made on the basis of a history of chronic kidney disease, characteristic symptoms of uremia, laboratory data of azotemia and other typical disorders of homeostasis. Differential diagnosis with acute renal failure is helped by anamnestic data and symptoms distinguishing chronic uremia (anemia, dystrophy, etc.).
Encephalopathy in chronic renal failure differs from an attack of encephalopathy in acute glomerulonephritis in its gradual development, not always deep coma, small convulsive twitching of individual muscle groups, noisy breathing, while renal eclampsia has an acute onset and is accompanied by complete loss of consciousness, dilated pupils, large convulsions and asphyxia.
Treatment of chronic renal failure is inseparable from the treatment of the kidney disease that led to kidney failure. In a stage not accompanied by disturbances in renal processes, etiological and pathogenetic therapy is carried out, which can cure the patient and prevent the development of renal failure or lead to remission and a slower course of the disease. In the stage of impaired renal processes, pathogenetic therapy does not lose its importance, but the role of symptomatic treatment methods increases (hypertensive drugs, antibacterial agents, protein restriction in the daily diet - no more than 1 g per 1 kg of body weight, sanatorium treatment, etc.). The combination of these measures makes it possible to delay the onset of chronic renal failure, and periodic monitoring of the level of glomerular filtration, renal blood flow and the concentration ability of the kidneys, the level of creatinine and urea in plasma makes it possible to predict the course of the disease.
Conservative treatment of chronic renal failure: therapeutic measures are mainly aimed at restoring homeostasis, reducing azotemia and reducing symptoms of uremia.
The protein content in the daily diet depends on the degree of renal dysfunction. When glomerular filtration is below 50 ml/min and the level of creatinine in the blood is above 0.02 g/l, it is advisable to reduce the amount of protein consumed to 30–40 g/day, and when glomerular filtration is below 20 ml/min, a diet with a protein content of no more than 20 is prescribed –24 g/day. The diet should be high in calories (about 3000 kcal) and contain essential amino acids (potato-egg diet without meat and fish). Food is prepared with a limited (up to 2–3 g) amount of table salt, and for patients with high hypertension - without salt. In the absence of edema and the presence of moderate hypertension, the patient is given an additional 2–3 g of table salt to add salt to food. Impaired calcium metabolism and the development of osteodystrophy require long-term use of calcium gluconate and vitamin D up to 100,000 IU per day, but the administration of vitamin D in large doses for hyperphosphatemia can lead to calcification of internal organs. To reduce the level of phosphates in the blood, use almagel 1-2 teaspoons 4 times a day; treatment requires regular monitoring of calcium and phosphorus levels in the blood.
For acidosis, depending on its degree, 100-200 ml of 5% sodium bicarbonate solution is administered intravenously. When diuresis decreases, furosemide (Lasix) is indicated in doses (up to 1 g/day) that provide polyuria. To reduce blood pressure, conventional antihypertensive drugs are used (see Hypertension) in combination with furosemide. Treatment of anemia is complex and includes the administration of testosterone propionate to enhance erythropoiesis, 1 ml of a 5% oil solution intramuscularly daily, and iron supplements. When the hematocrit is 25% and below, red blood cell transfusions in fractional doses are indicated. Antibiotics and chemotherapeutic drugs for chronic renal failure should be used with caution: the doses of penicillin, ampicillin, methicillin, ceporin and sulfonamides are reduced by 2-3 times. Streptomycin, monomycin, neomycin, polymyxin in chronic renal failure, even in reduced doses, can cause auditory neuritis and other complications. Nitrofuran derivatives are contraindicated in chronic renal failure.
In case of heart failure in patients with chronic renal failure, glycosides are used with caution, in reduced doses, especially in case of hypokalemia. When treating pericarditis, small doses of prednisolone are prescribed, but hemodialysis is more effective. Hemodialysis may be indicated for exacerbation of renal failure, and after improvement of the patient's condition, conservative therapy can be carried out again for a more or less long time.
Repeated courses of plasmapheresis provide a good effect in chronic renal failure. In the terminal stage, if conservative therapy does not have an effect and if there are no contraindications, the patient is transferred to treatment with regular (2-3 times a week) hemodialysis. Regular hemodialysis is usually used when creatinine clearance is below 10 ml/min and its plasma level becomes above 0.1 g/l. Experience shows that a long-term state of uremia, deep dystrophy, encephalopathy and other complications of chronic renal failure significantly worsen the results of hemodialysis and do not allow kidney transplantation, therefore decisions on hemodialysis and kidney transplantation should be made in a timely manner.
Forecast. Hemodialysis and kidney transplantation change the fate of patients with chronic renal failure, allowing them to prolong their lives and achieve rehabilitation for years. The selection of patients for these types of treatment is carried out by specialists from hemodialysis and organ transplantation centers.
Chronic kidney disease treatment
In the treatment of chronic kidney disease, two directions are used:
- the first is the treatment of the disease that caused the development of chronic kidney disease
- and second, nephroprotective treatment, which is universal for all renal pathologies.
Treatment of the underlying disease is specific and depends on the underlying disease itself. Nephroprotective treatment is common for all kidney pathologies and is aimed at slowing the progression of chronic kidney disease. Basically, slowing down the process is achieved by blocking the renin-angiotensin-aldosterone system. For this, a number of drugs are used: angiotensin receptor blockers, direct renin inhibitors, angiotensin-converting enzyme blockers, aldosterone antagonists, and so on. Also, in nephroprotective treatment, it is important to reduce the level of proteinuria by normalizing intraglomerular hypertension and protecting the proximal epithelium from endocytosis of proteins. In the treatment of chronic kidney disease, it is very important to carry out antihypertensive therapy for concomitant hypertension. In the case of progressive chronic renal failure at stage 4 of chronic kidney disease, the question of dialysis or kidney transplantation is raised. At the fifth stage of the disease, dialysis or kidney transplantation is mandatory.
Diagnostics
If chronic renal failure is suspected, consultation with a nephrologist and a series of laboratory and instrumental studies are required. The most reliable are laboratory tests according to Zimnitsky, Reberg, general and biochemical blood and urine tests. To make a diagnosis of chronic renal failure, the basis is:
- decreased glomerular filtration level;
- high concentration of urea and creatinine;
- hyposthenuria - decreased urine density.
Ultrasound, CT or MRI of the kidneys reveals a decrease in their size and a pronounced decrease in the thickness of the parenchymal tissue, and echo Dopplerography of the renal vessels demonstrates a decrease in renal blood flow.
The powerful diagnostic base of the Clinic of Modern Medicine allows you to conduct a comprehensive examination for chronic renal failure and promptly obtain the results necessary to establish the correct diagnosis. The scope of necessary research is determined by the clinic’s specialists at the initial consultation.