Currently, about 30% of the world's population have various types of urinary disorders. About 100 million people suffer from urinary incontinence. Neurogenic bladder dysfunction is rightfully considered one of the most severe sufferings in terms of its impact on the patient’s quality of life.
Meanwhile, according to a number of large studies, only 27% of patients who consulted a doctor were able to receive sufficient advice and treatment. This circumstance is largely due to the lack of necessary understanding among general practitioners about the pathophysiology of urinary disorders, the ineffectiveness of outdated approaches and previously proposed standards of treatment. Significant difficulties in making a diagnosis in patients with urinary disorders are associated with the existing confusion in terminology and classification.
Pathophysiology of neurogenic bladder dysfunction
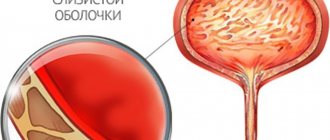
The lower urinary tract - the bladder and urethra - is a complex anatomical and physiological complex united by the unity of the functions of accumulation, retention and excretion of urine, while each of these three functions can normally be adequately controlled.
Urinary tract dysfunctions in patients with verified neurological diseases are classified as neurogenic dysfunctions. In the absence of neurological pathology, disorders are considered idiopathic.
From a neurological point of view, the lower urinary tract has a complex mixed innervation united by multi-level reflexes. According to the most common concept, a simplified diagram of the innervation of the lower urinary tract is as follows.
Scheme of innervation of the bladder
1 - center of voluntary control of urination of the cerebral cortex; 2 - stem urinary control center (bridge); 3 - lumbar and extraspinal sympathetic ganglia; 4 - parasympathetic ganglia and nerve pathways; 5 - bladder; 6 - sphincter apparatus of the bladder.
The adaptive function of the bladder is controlled by the sympathetic nervous system. Extraspinal sympathetic ganglia provide the function of urine storage by maintaining a relaxed state of the detrusor and tonic contraction of the internal sphincter. A constant inhibitory effect on filling signals coming from the bladder receptors is normally provided by the stem (pontine) urinary control center. Reaching the threshold of its adaptation is accompanied by the appearance of an urge. At the same time, further urinary retention is controlled by cortical centers, which provide voluntary contraction of the external urethral sphincter through somatic nerves. Sensory innervation and, ultimately, bladder emptying are provided primarily by parasympathetic ganglia and nerve pathways at the level of the sacral spinal cord. For adequate urination, simultaneous friendly (synergistic) contraction of the detrusor and relaxation of the bladder sphincters are necessary.
From the point of view of pathogenesis and the possibility of assessing the level of denervation, the following classification of neurogenic bladder dysfunctions seems successful:
- Uninhibited cortical bladder
- Reflex spinal bladder
- Unadapted bladder a - spinal
- b - ganglionic
- a - spinal
Uninhibited cortical bladder - characterized by functional weakness of cortical centers, which are unable to provide an inhibitory effect on spinal structures, while voluntary control over urinary continence when urge occurs is absent or weakened. In patients with an uninhibited bladder, a common manifestation is the presence of an uncontrollable (imperative) urge to urinate, which leads to urge urinary incontinence. An uninhibited bladder in children is often associated with intrauterine hypoxia, birth trauma, or delayed development and maturation of regulatory centers. In adults, loss of voluntary control over the lower urinary tract is caused by microcirculatory disorders, trauma and inflammatory damage to the frontal lobes of the cerebral cortex. Reflex spinal bladder - occurs in patients with damage to the spinal cord above the lumbosacral centers. In the absence of the inhibitory influence of the brain, urination occurs involuntarily with a small volume of bladder filling, similar to a spinal reflex. A number of such patients urinate when a feeling of heaviness appears in the lower abdomen by voluntary irritation of the skin of the thighs or by stimulating a reflex contraction of the detrusor by pressing on the bladder area (Creed, Valsalva maneuvers). In some patients, suprasacral denervation may be accompanied by persistent spasm of the external urethral sphincter or the appearance of its reflex contractions simultaneously with contraction of the detrusor (sphincter-detrusor dyssynergia). In these cases, patients develop chronic urinary retention. Unadapted bladder - characterized by a decrease in the adaptive (storage) function of the bladder due to damage to the sympathetic centers of the spinal cord or extraspinal sympathetic ganglia. In patients with an unadapted bladder, the urge is usually absent or sharply weakened, which is associated with the inability to fill the bladder to a threshold level. With ganglion lesions, incontinence in patients can be combined with a small amount of residual urine, which is due to partial preservation of sphincter function, since complete destruction of all ganglia, as a rule, does not occur. Reflex bladder - characterized by the absence or significant weakening of the urge to urinate due to loss of sensitivity due to damage to the spinal or ganglion parasympathetic centers, as well as underdevelopment or death of the peripheral nerve endings of the bladder (intramural forms). In such patients, the equivalent of urge can be achieved only with maximum filling of the bladder. Mixed bladder manifests itself as chronic urinary retention followed by dilatation of the upper urinary tract and increasing renal failure. Common symptoms in patients are the development of overflow urinary incontinence (ischuria paradoxa) and constipation. Patients with a reflex bladder require continuous urinary diversion or intermittent catheterization. Shriveled bladder - develops as a result of the progression of degenerative-sclerotic changes in the detrusor in conditions of its denervation, infection and/or prolonged drainage of the bladder.
Involvement of the area of Lieto's triangle in the process can lead to disruption of the outflow of urine from the upper urinary tract, which requires surgical measures. According to the above etiopathogenetic aspects, the term neurogenic bladder should be understood as dysfunction of the bladder and its sphincters, which develop as a result of neurological diseases and damage to the central and peripheral nervous system. The complexity, the presence of additional nerve pathways, the dominant positions of the autonomic system and a large number of control centers at different levels determine the multiplicity of options and paradoxical manifestations of neurogenic bladder dysfunction. Clinicians are well aware of situations that contradict or do not fit into the pathogenetic classification presented above.
Read also
Arnold-Chiari malformation
Due to the availability of the study and the high resolution of MRI, we quite often come across the conclusion - Arnold-Chiari anomaly.
What is meant by this concept? Arnold-Chiari malformation... Read more
Rehabilitation after stroke
It is very important to begin rehabilitation after a stroke as early as possible, since further recovery and the ability to avoid disability depend on this. For rehabilitation after a stroke in the clinic “First...
More details
Brain concussion
A concussion is a mild traumatic brain injury without damage to the bones of the vault and base of the skull. In this condition, there are no pronounced disturbances in the functioning of the brain and there are no changes...
More details
Vertebral artery syndrome
The main vascular highways carrying blood to the brain pass in the neck - these are two carotid and two vertebral arteries. A decrease in blood flow through the vertebral arteries will lead to the development of acute...
More details
Facial paralysis (Bell's palsy/facial neuritis)
Facial paralysis is spontaneous weakness of ½ of the face. The cause is swelling of the facial nerve, as a result of its compression inside the temporal bone or in the outlet from it. Most often this leads to...
More details
Clinical and urodynamic classification of neurogenic urinary tract dysfunction
In 1992, Wayne proposed a simplified classification of neurogenic bladder dysfunctions in terms of urodynamic disorders:
- Overactive bladder.
- Sphincter-detrusor dyssynergia.
- Detrusor areflexia.
Overactive bladder is a chronic condition characterized by symptoms of frequency, urgency, and nocturia, with or without urgency urinary incontinence. It should be understood that the diagnosis of overactive bladder can be made if these symptoms are not caused by bladder diseases or metabolic disorders. Therefore, the diagnosis of any form of neurogenic dysfunction can be verified only on the basis of a comprehensive neurourological examination, including a mandatory urodynamic study (uroflowmetry, cystometry, profilometry, pressure-flow study, etc.). The most important urodynamic criterion for diagnosing hyperactivity is the appearance of involuntary contractions of the detrusor with a pressure amplitude of more than 5 cm of water. Art. during cystometry. Thus, the term “overactive bladder” should be considered as a diagnosis, and overactive detrusor as its main urodynamic manifestation.
In patients with spinal cord injury (reflex spinal bladder), when cystometry is performed, so-called terminal detrusor overactivity is often encountered, which is characterized by contraction of the detrusor and the occurrence of urination in the complete absence of urge. Detrusor overactivity occurs in 77% of patients with neurogenic bladder dysfunction. This is due to the fact that in most neurological diseases, the spinal link of the voiding reflex - its lumbosacral centers - is usually not completely destroyed. Experimental studies have shown that under conditions of the “decapitated” reflex in the bladder, unmyelinated C-fibers are activated and the content of nerve growth factor in the detrusor increases. The unity of histochemical changes in the bladder wall in patients with neurogenic and idiopathic detrusor overactivity suggests that the formation of overactive bladder syndrome is always a consequence of its complete or partial denervation, which developed for an established or unidentified reason. Sphincter-detrusor dyssynergia is characterized by involuntary contractions of the external urethral sphincter and/or paraurethral muscles during detrusor contraction. Violation of concomitant relaxation of the sphincter and contraction of the detrusor leads to the development of functional bladder outlet obstruction and the appearance of residual urine in patients. Sphincter-detrusor dyssynergia usually occurs in patients with suprasacral spinal cord injuries. Patients with sphincter-detrusor dyssynergia account for 33–55% of all patients with neurogenic bladder dysfunction. To define intermittent urination due to involuntary contraction of the sphincter and periurethral muscles in patients without neurological diseases, the term dysfunctional urination has been proposed. Detrusor areflexia is characterized by a decrease or complete absence of the ability of the detrusor to contract. The main manifestation of areflexia is the complete absence of the urge to urinate in patients. Most often, detrusor areflexia occurs in patients with damage to the sacral and infrasacral centers (meningomyelocele, radical surgery and injuries with damage to the pelvic organs). In this case, 50% of patients have a spastic state of the urethral sphincter. Patients with detrusor areflexia require constant urological supervision due to the high risk of urinary infection and the frequent occurrence of complications from the upper urinary tract. A number of patients with damage to the sacral centers develop obstruction due to sphincter spasm, which is characterized by persistent contraction of the urethral sphincters. In a number of these patients, urodynamic stress incontinence occurs when the bladder is full.
In modern clinical practice, the term stress incontinence is used to define urinary incontinence due to stress (from the English stress - tension), for example, coughing, laughing, sneezing. Involuntary leakage of urine due to stress incontinence is usually not associated with neurological disorders. The main role in the development of stress incontinence belongs to disturbances in the anatomy of the ligamentous apparatus and the function of the pelvic floor muscles and damage to the urethral sphincters.
Diagnostics
A neurourologist diagnoses and treats the disease. The specialist suspects neurogenic weakness of the bladder even at the stage of collecting complaints. To objectively confirm the neurogenic nature of urination disorders, the patient begins to keep a diary (it records the frequency of urges, controlled and involuntary urination, and the approximate volume of urine). By studying the diary, the urologist can objectively assess the clinical situation and the consistency of the patient’s symptoms and complaints.
To exclude organic changes in the urinary system and infectious causes of dysfunction, additional examination is prescribed. The patient donates urine and blood, undergoes an ultrasound of the pelvic organs, excretory urography, and a comprehensive urodynamic study.