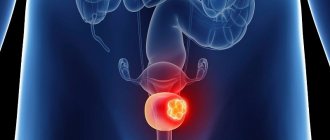
Ureterocele is a specific disease of the urinary tract, which manifests itself in pathological expansion of the distal (intravesical) part of the ureter. A cyst forms in the affected area and protrudes into the bladder. Over time, unpleasant symptoms develop and begin to intensify: urinary disorders, back pain.
Feature of the disease: the cyst deforms the bladder and can increase over time. The disease affects women more often than men.
For diagnosis, you should contact a urologist; you will need to undergo a series of instrumental examinations. Treatment is predominantly surgical. There are several modern and safe ways to get rid of ureterocele. During the operation, not only the pathological area is removed, but also the normal structure of the ureter is restored.
At CELT you can get a consultation with a urologist.
- Initial consultation – 3,000
- Repeated consultation – 2,000
Make an appointment
Why does ureterocele occur?
The proportion of cases of ureterocele in urology does not exceed 3%. Moreover, female representatives encounter it 3-4 times more often. They are diagnosed with predominantly congenital narrowing of the ureteric orifice. This defect leads to the formation of a cystic or spherical protrusion in the bladder.
Ureterocele in men is more often an acquired disease. It is associated with urolithiasis, in which a stone becomes trapped in the ureter. The danger of ureterocele lies in microbial infection, the addition or frequent exacerbation of pyelonephritis and cystitis, and subsequently nephrosclerosis and complete kidney failure up to the need for its removal.
Complications and prevention
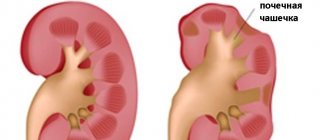
The most common complication is the development of hydronephrosis, in which fluid accumulates in the renal pelvis. The second most common is ureterocele prolapse. The likelihood of infection and strangulation increases. Pyelonephritis may develop. Ureterocele increases the likelihood of developing urolithiasis. Prolonged course of the disease can lead to chronic renal failure.
Prevention consists, firstly, in timely and complete treatment of infectious and inflammatory diseases of all organs of the genitourinary system. Antibiotic therapy must be carried out under the supervision of a physician until the pathogen is no longer isolated in the tests.
If any unpleasant symptoms from the genitourinary system appear, you should immediately contact a urologist. In the multidisciplinary CELT clinic, you can undergo a full examination and begin treatment for ureterocele.
How does a ureterocele manifest?
The main symptom of a ureterocele is difficulty urinating. The patient may complain of frequent urge to go to the toilet. As the disease progresses, the opening of the second ureter may become blocked. In this case, the existing symptoms intensify and hydronephrosis develops. This is indicated by renal colic - acute, severe, paroxysmal pain in the kidney area.
At an early stage, typical symptoms of ureteral narrowing are observed:
- lower back pain;
- signs of exacerbation of cystitis;
- feeling of fullness in one of the sides;
- inability to urinate (with complete blockage);
- impurities of blood and pus in the urine;
- elevated temperature;
- urinary incontinence (in later stages).
2. Reasons
The leading cause in the volume of registered cases of ureterocele is considered to be a congenital anomaly. However, the acquired variant is also not a casuistic accident: “ordinary” strictures, tumors, migrating stones, etc. can lead to a narrowing of the lumen and a chronic increase in pressure in the renal excretory system. In turn, the pressure on the walls stretches the mouth of the ureter in the form of an intravesical “air” ball", but not only; constant stagnation causes the development of a number of dangerous complications in the renal pyelocaliceal system (hydronephrosis, pyelonephritis).
There are two types of ureterocele: orthotopic and ectopic. They differ significantly in clinical presentation, prognosis and therapeutic protocol, but they are based on different localization: an ectopic ureterocele is located lower and can prolapse (protrude) even into the urethra, which in women can lead to strangulation when the ureterocele prolapses outside. In addition, ectopic ureterocele is often accompanied by doubling of the kidney and ureter, reflux of urine into the renal pelvis and/or hydronephrosis.
Visit our Urology page
Types and stages of the disease
Ureterocele has several types and variants of its course. In addition to the one-sided form, there is a two-sided form, when the cyst also forms on the second ureter. Classification of ureterocele according to developmental features:
- Simple. Only one cyst is formed, which is not accompanied by other diseases of the urinary organs.
- Prolapsing. A form of ureterocele that only women experience. It is a prolapsing cyst that can be seen during external examination as it passes through the urethra.
- Ectopic. The cyst spreads to other parts and organs. Associated with low ectopia, i.e. displacement of the mouth relative to the natural location, which is typical for healthy people.
The cyst can have different sizes, which determines the severity of the manifestations of the disease:
- First. The pathological process does not affect the kidneys, and the intravesical part of the ureter is slightly dilated.
- Second. Against the background of an enlarged ureter, stagnation of urine is observed and hydronephrosis begins.
- Third. Against the background of bladder dysfunction, kidney function is significantly impaired.
Rehabilitation regimen after surgery
- Limit active sports and do not lift heavy objects;
- Do not overcool;
- Follow a diet limiting salty and fatty foods;
- Drink enough fluids.
- After surgery, you should be observed by a urologist on an outpatient basis. You can schedule your first visit after 3 months, then every 6-12 months.
Cost of the operation: transurethral resection of ureterocele with ureteral stenting* - from RUB 59,000.
*The basic cost of the operation does not include: preoperative examination, anesthesia, histological examination of surgical material and hospital stay.
Diagnostic methods
Ureterocele is discovered incidentally in most patients. A patient seeks help with complaints of problems with urination. The patient is prescribed additional procedures and the true cause of the symptoms is discovered. Diagnosis of ureterocele is very simple, since the defect can be detected without the use of specific methods. The main studies are:
- general urine analysis;
- ultrasonography;
- X-ray cystography and urography;
- cystoscopy (in the most severe cases).
Ureterocele and urolithiasis
A ureterocele is a developmental anomaly of the urinary system, which is a local cyst-like expansion of all layers of the terminal ureter [1–4]. This type of anomaly is usually classified as combined malformations of the urinary tract [5–7]. Although, we should probably agree that ureterocele is an independent form [8], which requires a qualified classification agreement. The problem of ureterocele and associated complications (the most common of which is urolithiasis) remains relevant to this day, since there are no generalizing studies, and individual fragments in publications cannot reflect the entire problem as a whole [9–15]. In elucidating the etiology and pathogenesis of urolithiasis, exceptional importance is attached to disturbances in the urodynamics of the upper urinary tract with ureterocele. Long-term obstruction and urostasis are ideal conditions for stone formation, and the addition of a urinary infection leads to an acceleration of this process. The combination of ureterocele and urolithiasis remains, in fact, a poorly understood problem. This is explained by a number of circumstances. First of all, there is terminological confusion based on insufficient consideration of the mechanisms of etiology and pathogenesis of this defect of the intramural ureter. Insufficient interpretation of data obtained during a clinical examination of a patient in some cases leads to unfounded conclusions. And finally, the prevailing opinion among clinicians about the low prevalence of this anomaly in the practice of a urologist explains the insufficient readiness of specialists to develop rational treatment tactics for various forms of ureterocele.
Thus, the main unresolved issues include the following. What determines the choice of surgical treatment for ureterocele? What should be the treatment tactics for stones, depending on the type and size of the ureterocele? What should you do if you have a stone-free ureterocele and a unilateral kidney stone?
Materials and methods We observed 51 patients in whom true ureterocele was combined with urolithiasis, which accounted for 43.2% of all patients with this malformation and 9.6% of all manifestations of urolithiasis in abnormal kidneys. The process was more often unilateral (82.3%), although there was also bilateral damage (17.7%). In the overwhelming majority of people (84.3%), the ureterocele was orthotopic in nature. The heterotopic variant, related to the upper segment of the double kidney, occurred in 8 patients (15.7%). A predominance of women was noted in a ratio of 2.7:1.0. The average age of patients was 41.9±2.0 years, with the largest number of patients falling in the age group of 31–50 years (58.8% of observations), which emphasizes the significant social significance of this problem. The analyzed group also included 5 patients in whom the ureterocele did not contain a stone, but the stone was diagnosed in the hollow system of the ipsilateral kidney, as well as 8 patients in whom there was a unilateral combination of a kidney stone with a stone in the ureterocele. In the presence of stones in the kidneys and ureters, the average size of the ureterocele was 20.7±1.3 mm - the size is relatively small. The average conventional area of the stone was 1.4±0.2 cm2. At the same time, stones in ureterocele were present in 46 patients (90.2%). A fairly common complication was the multiple nature of stones (21.6%).
The urodynamic parameters of the upper urinary tract are important for determining treatment tactics and further prognosis. It was assessed on a 4-point scale: 1 point – absence of urodynamic disturbances; 2 – moderate dilation of the ureter without dilation of the pelvis and calyces and with preserved functional condition of the kidney; 3 – total dilatation of the ureter and pelvis without expansion of the calyces with more than 50% of the functional activity of the kidney preserved; 4 – urodynamic disturbances of the upper urinary tract extend to the calyxes, and kidney function is lost by 75%. The average indicators reflecting disturbances in the urodynamics of the upper urinary tract corresponded to 1.6±0.2 points.
In addition to the shape and size of the ureterocele, the anatomical and functional state of the upper and lower urinary tract, as well as the age of the patients, the degree of activity of chronic pyelonephritis is assessed when developing a treatment strategy. If in previous studies concerning ureterocele, the basis of diagnosis was the quantitative determination of leukocyturia [8], then at present it is not possible to judge the degree of activity of chronic pyelonephritis without conducting a bacteriological examination of urine. Initial bacteriuria was detected in 23 patients, which accounted for 45.1% of all cases of a combination of ureterocele and urolithiasis, and exceeding the threshold of 105 CFU/ml was observed in 68.2% of patients. In the treatment of combinations of ureterocele and urolithiasis, preference was given to endoscopic interventions, which were performed in 43 adult patients. All manipulations were performed under anesthesia. Advantage was given to epidural anesthesia (25), which, with minimal impact on the cardiovascular and respiratory systems, provided the possibility of bilateral contact with the patient during the entire procedure, allowing for postoperative pain relief with lower anesthetic costs.
Results The main goals of any operation are to restore normal urodynamics of the upper urinary tract while maintaining the functional state of the kidney, remove stones, and also prevent possible associated complications, the main one of which is the development of vesicoureteral reflux. In the majority of patients (87.8% of all those operated on) with both orthotopic and heterotopic variants of the defect complicated by urolithiasis, the main surgical interventions were endoscopic perforation (5) and dissection of the ureterocele wall (38).
The necessary conditions for these operations were the presence of small and medium-sized ureteroceles (no more than 30 mm), the absence of impaired contractility of the terminal ureter, moderate impairment of the urodynamics of the upper urinary tract (no more than 2 points), as well as preserved kidney function in the absence of exacerbation of pyelonephritis. When choosing a modification of endovesical surgery, preference was given to dissecting the ureterocele using a “Hook” type loop and a Ho:YAG laser, since the incision of the cyst wall is more controlled, and the inflammatory swelling of the tissues, as a rule, is less pronounced. The main argument was that in this case, ureterolithoextraction of stone or its fragments after contact ureterolithotripsy is easier.
Wanting to minimize the risk of developing postoperative complications, including vesicoureteral reflux, special attention was paid to anti-reflux modifications of transurethral dissection of the ureterocele. The results obtained correlate with literature data [16–19], indicating that the best task for decompressing ureteroceles, restoring impaired urodynamics of the upper urinary tract, removing stones and preventing vesicoureteral reflux is transverse incision of the ureterocele using the “smiling mouth” type. The resulting upper part of the anterior wall of the ureterocele, floating in the bladder, acts as a valve leaflet when intravesical pressure increases, preventing the reverse flow of urine into the ureter.
Longitudinal dissection of the ureterocele wall was attempted, if possible, from a visually defined area of the narrowed ureteral orifice along the interureteral fold medially for 5–8 mm. Further actions were determined by a number of circumstances. We paid special attention to careful coagulation of blood vessels in the incision area. When the stone size is up to 10 mm in maximum dimension and there are no secondary inflammatory changes on the side of the cyst wall, ureterolithoextraction (7) was performed using a Dormia basket (1) or endoscopic gripping forceps (6), trying to grab the stone along its smallest diameter. This technique allows for reliable fixation of the calculus and is a method of actively preventing its migration proximally along the ureter. The manipulation itself was carried out under direct visual control or under X-ray television control. We avoided sharp, violent actions when removing the stone, trying to achieve the goal not by minimizing manipulation time, but in accordance with the principle of “maximum efficiency with minimum complications.” If the size of the stone does not correspond to the diameter of the incision made in the ureterocele wall, we believe that additional enlargement of the incision is less dangerous than forcible removal of a disproportionately large stone. To prevent iatrogenic trauma to the urethra associated with removing the entire stone through the urethra, cystolithotripsy was previously performed in 15 patients - mechanical in women (9) and electrohydraulic in men (6).
Large stones in the ureterocele, one of the sizes of which exceeded 10 mm, required more extensive incision of the ureterocele to perform simple ureterolithoextraction, which increased the likelihood of the formation of vesicoureteral reflux in the postoperative period. In a number of clinical situations, it was necessary to resort to ureteroscopy and contact ureterolithotripsy to remove the stone (19 patients). When choosing a specific lithotripsy method, we gave preference to ultrasound and ureterolithotripsy using a holmium (Ho:YAG) laser, abandoning the electrohydraulic method of stone destruction. This is explained by the fact that with these methods the stone is not destroyed into several large fragments at once, as with the electrohydraulic method, creating the prerequisites for retrograde migration of fragments with the flow of washing liquid, but is bitten into small parts, which are immediately aspirated [20–23].
A special clinical group of patients consisted of patients who had unilateral stones in both the ureterocele and the kidney (8), as well as patients with small acalculous ureterocele and stones in the homolateral kidneys (5). Common to all patients in this situation is the need to solve a two-pronged problem when drawing up a treatment plan: elimination of ureteral obstruction in the form of ureterocele and the subsequent use of extracorporeal shock wave lithotripsy (ESWL) for kidney stones. When deciding on the method of decompression of an uncomplicated ureterocele, we preferred electrodissection of the wall to the electroperforation method, since we considered the volume of the latter to be insufficient for future passage of stone fragments. ESWL was performed on average after 27.5±3.2 days. The number of sessions per patient was 1.33±0.44 per session, including twice in 2 patients.
Particular difficulty arises in patients with large orthotopic ureterocele – more than 30 cm3 with significant impairment of urodynamics (3–4 points) of the upper urinary tract. Transurethral endoscopic surgery in such situations is not justified due to the fact that it is not able to provide radical elimination of the anatomical defect and potentially significantly increases the risk of vesico-renal reflux and exacerbation of pyelonephritis. In this regard, the justified and only possible method of treatment is ureterocystoneostomy according to the Politano-Leadbetter method. It was performed in 6 patients. This operation, technically tested in uncomplicated conditions, in the presence of a calculus in exceptional cases may be accompanied by additional difficulties. This is due to the fact that before performing reconstructive plastic surgery, it is necessary to solve the problem of removing the stone, which can migrate proximally along the dilated ureter. In such situations, we divided the surgical intervention into 2 stages. First, transurethral electroincision of the ureterocele wall was performed under epidural anesthesia, followed by ureteroscopy and ureterolithotripsy. The next stage was reconstructive plastic surgery. Questions about the timing of staged treatment have not yet been finally resolved. In the case of an uncomplicated course of the 1st stage, under the conditions of one anesthetic provision, it was considered acceptable to perform 2 stages in 1 treatment session.
The results of treatment were assessed by the level of complications encountered and auxiliary manipulations, on the one hand, as well as by the degree of stone elimination from the ureter, on the other. It should be noted that complications directly related to ureterolithoextraction were not noted in any case. The most common complication of the immediate postoperative period was the development of acute pyelonephritis (6), the prevention of which was adequate antibacterial therapy with mandatory consideration of bacteriological examination of urine culture obtained separately from the kidney and bladder. In addition, endoscopic operations were necessarily completed with bladder drainage using a 12–14 Fr Foley catheter. This approach, in our opinion, provides functional rest to the bladder, improving the process of regeneration of the wound surface, and is also a method of active prevention of high-pressure vesicoureteral reflux and activation of pyelonephritis. The timing of postoperative drainage is purely individual, however, in the most general form, the urinary catheter was removed after 3–5 days. In 1 patient, after longitudinal dissection of the wall of a heterotopic ureterocele followed by ureterolithoextraction, vesicoureteral reflux occurred into the upper half of the double kidney. In our opinion, this is due to deformation of the mouth of the terminal part of the ureter against the background of a violation of its contractility and a pronounced disturbance of the urodynamics of the upper urinary tract. Note that, among others, for this type of defect, treatment options include heminefroureterectomy with transvesical excision of the ureterocele membranes or its intraoperative aspiration, and ureterocystoneostomy using the antireflux technique, as well as interureteral or ureteropyeloanastomosis in combination with aspiration of the ureterocele contents and antegrade ureterolithoextraction.
The most severe complication in the postoperative period in patients with ureterocele is vesicoureteral reflux. If its presence was suspected, ultrasound diagnostics were initially performed: the volumes of the upper urinary tract were compared at low intravesical pressure, with tension in the muscles of the anterior abdominal wall under conditions of threshold filling of the bladder with urine and immediately after its voluntary emptying. Micture cystourethrography was resorted to according to strict criteria, mainly when there was a lack of information obtained from ultrasound scanning, and when deciding on the advisability of performing reconstructive plastic surgery. Auxiliary procedures were determined by the need for postoperative temporary drainage of the kidney with a ureteral catheter (9) or a stent (1). The level of auxiliary procedures per 1 patient was 0.25. The completeness of clearance of the urinary tract from stones associated with ureterocele at discharge was generally 81.6%. Successful use of ESWL for kidney stones for up to 2 months. after elimination of the ureterocele, this figure increased to 87.7%.
Discussion The main place in the diagnosis of ureterocele belongs to survey and excretory urography, which allows one to obtain information not only about the presence of the defect itself and the topical diagnosis of urolithiasis, but also indirect data about the anatomical and functional state of the kidney and upper urinary tract. The effectiveness of urography in diagnosing this defect reaches 95.8% [8]. Difficulties arise in the case of a “dumb” kidney or one of the duplicated segments. The widespread introduction of echotomography has increased the level of diagnosis verification to almost 100%. In our practice, we have practically abandoned cystoscopy as an independent research method, regardless of the form of combination of urolithiasis and ureterocele, considering endoscopic examination of the bladder as the first stage, which is inextricably linked with the implementation of a specific therapeutic procedure. The question of choosing tactics for surgical treatment of ureterocele in combination with urolithiasis still does not have a clear answer, which is largely due to the presence of various forms of this defect in combination with different options for localization, size and duration of presence of stones. Of no small importance are the age factor, the severity of urodynamic disorders of the upper urinary tract and the anatomical and functional state of the kidneys.
The development of minimally invasive technologies in recent decades could not but affect modern methods of treating ureterocele complicated by urolithiasis. However, unlike other forms of renal anomalies, the use of ESWL as a first-line treatment, despite the small size of the stones, is limited by the anatomical obstacle in the form of a narrowed ureteral orifice, which causes disturbances in the urodynamics of the upper urinary tract.
The best way to decompress the upper urinary tract and, as a consequence, eliminate the ureterocele is by electroperforation and electrodissection of its wall in both orthotopic and heterotopic variants. These operations are indicated for patients with small and medium-sized ureteroceles (no more than 30 mm), in the absence of impaired contractility of the terminal ureter, with moderate impairment of the urodynamics of the upper urinary tract, preserved kidney function and no exacerbation of pyelonephritis. These factors are decisive in the prevention of postoperative complications, including vesicoureteral reflux, regardless of the type of ureterocele (ortho- or heterotopic).
Electrical dissection of the ureterocele wall and subsequent ureterolithoextraction are permissible for relatively small stones that do not exceed the size of the incision. In other cases, after incision, it is preferable to perform ureteroscopy and contact ultrasound or ureterolithotripsy using a holmium laser. The issue of drainage of the upper urinary tract after stone extraction from an ureterocele does not have a clear solution. On the one hand, catheterization prevents obstructive complications after endoscopic intervention on the ureter. On the other hand, internal drainage of the kidney can serve as an entry point for infection and contribute to the formation of vesicoureteral reflux. In this regard, indications for internal kidney drainage are determined by the following conditions: the presence of unilateral “symptomatic” stones in the kidneys and ureters; initial bacteriuria in a diagnostic titer exceeding the threshold value; local secondary inflammatory reaction of the tissues of the walls of the ureterocele; pronounced disturbance of the urodynamics of the upper urinary tract. For all patients with initial bacteriuria, it is reasonable to undergo a 7-10-day course of antibacterial therapy, prescribed 1-2 days before the expected date of endoscopic manipulation. In case of initially “sterile” urine, patients should be prescribed a short - 3-5-day preventive course of treatment with tablet forms of antibiotics from the group of fluoroquinolones, cephalosporins and protected aminopenicillins (amoxicillin + clavulanic acid) with mandatory bacteriological examination of a urine culture obtained separately from the kidney and bladder . This approach corresponds to modern principles of antibacterial therapy of chronic pyelonephritis and prevention of hospital infections [24, 25].
Literature 1. Lopatkin N.A., Lyulko A.V. Anomalies of the genitourinary system. Kyiv: Health, 1987. 416 p. 2. Derevianko T.I. Anomalies of the uretero-vesical segment: abstract. dis. ... doc. honey. Sci. M., 1998. 53 p. 3. Brueziere J. Ureteroceles // Ann. Urol. (Paris). 1992. Vol. 26(4). R. 202–211. 4. Coplen DE, Duckett JW The modern approach to ureteroceles // J. Urol. 1995. Vol. 153(1). R. 166–171. 5. Bukharkin B.V. Kidney anomalies (clinical and diagnostic): Dis…. Ph.D. honey. Sci. M., 1978. 181 p. 6. Abramyan A.Ya., Trapeznikova M.F., Bukharkin B.V. Classification of kidney anomalies // Act. question urology. Vol. 4. M.: MONIKI, 1980. pp. 1–12. 7. Trapeznikova M.F., Sobolevsky A.B., Urenkov S.B. Combined anomalies of the urinary system / In the book: Act. problems of medicine. M.: MONIKI, 1993. pp. 52–55. 8. Urenkov S.B. Ureterocele: clinical picture, diagnosis and treatment: abstract. dis. ...cand. honey. Sci. M., 1988. 19 p. 9. Evlanov A.P. Combination of ureterocele with multiple stones in it and a large number of stones in the lower third of the ureter // Urol. and nephrol. 1972. No. 2. P. 58. 10. Dolgatov V.G. Surgical treatment of ureterocele in children: abstract. dis. ...cand. honey. Sci. L., 1976. 17 p. 11. Rumyantseva G.N., Latyshev M.M. Results of treatment of ureterocele // Urol. and nephrol. 1977. No. 1. P. 31–33. 12. Nash AG, Knight M. Ureterocele calculi // BJU 1973. Vol. 45. R. 404–407. 13. Vexler L. Calculi in ureterocele // Rev. Med. Chir. Sec. Med. Nat. Jasi. 1974. Vol. 78. R. 157–159. 14. Mosbah A., Bouchallouf A., Aziz E. Les ureteroceles compliquees de lithiase. A propos de quatre cas // Ann. Urol. (Paris). 1990. Vol. 24 (5). R. 386–387. 15. Jemni M., Loussaief H., Ben Fadhel S., Ben Hassine L., El Ouakdi M., Ayed M. Traitement des ureteroceles compliquees de lithiase // Ann. Urol. (Paris). 1994. Vol. 28(2). R. 102–104. 16. Sapozhnikov I.M. Clinic, diagnosis and treatment of ureterocele in adults: Dis. ...cand. honey. Sci. M., 1993. 117 p. 17. Rodriguez JV Endoscopic surgery of calculi in ureteroceles // Eur. Urol. 1984. Vol. 10 (1). R. 36–39. 18. Rich MA Low transurethral incision of single system intravesical ureteroceles in children // J. Urol. 1990. Vol. 144. R. 120–121. 19. Uberreiter S., Janetschek G. Therapiekonzept der komplizierten Ureterozele im Kindesalter // Urologe A. 1991. Vol. 30(2). R. 106–110. 20. Lopatkin N.A., Mazo E.B., Chepurov A.K. and others. Endoscopic ureterolithotripsy with a holmium laser // Urol. and nephrol. 1997. No. 3. pp. 25–29. 21. Dondukov Ts.V. Endoscopic ureterolithotripsy with holmium (Ho-YAG) laser: Author's abstract. dis. ...cand. honey. Sci. M., 1999. 26 p. 22. Taari K., Lehtoranta K., Rannikko S. Holmium: YAG laser for urinary stones // Scand. J. Urol. Nephrol. 1999. Vol. 33(5). R. 295–298. 23. Aron M., Costello AJ Case report: holmium laser resection and lasertripsy for intravesical ureterocele with calculus // Lasers. Surg. Med. 2001. Vol. 29(1). R. 82–84. 24. Perepanova T.S. Complex treatment and prevention of hospital-acquired urinary tract infection: Abstract of thesis. dis. ... doc. honey. Sci. M., 1996. 42 p. 25. Derevianko I.I. Modern antibacterial chemotherapy for pyelonephritis: abstract. dis. ... doc. honey. Sci. M., 1998. 57 p.
Effective treatment
The urologist chooses how to treat narrowing of the ureter based on the severity of the ureterocele. It is not possible to solve the problem in a conservative way, and operations for narrowing of the ureter can be reconstructive or organ removal.
If the disease has spread to the kidney, it is removed along with the cyst in an operation called nephrectomy. If the kidneys are able to perform their function, then doctors make do with a less traumatic endoscopic operation, during which the cyst is removed.
At the State Urology Center you can receive qualified medical care under the compulsory medical insurance program. Make an appointment with a urologist right now using the online appointment form. Remember that the smaller the cyst, the simpler and less dangerous it will be to remove.
On weekdays you can get an appointment with a urologist on the day of your visit
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Ultrasound of the bladder | 2 500 |
| Urography intravenous | 6 000 |
| Cystoscopy | 5 000 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Hakobyan Gagik Nersesovich – professor, doctor of medical sciences, oncologist, urologist in Moscow
The appointment is conducted by a doctor of the highest category, urologist, oncologist, doctor of medical sciences, professor. Author of more than 100 scientific papers.
Urological oncology experience – more than 15 years. Helps men and women solve urological and oncourological problems.
Conducts diagnostics, treatment and complex operations for such diagnoses as:
- tumors of the kidneys and upper urinary tract;
- prostate and bladder cancer;
- urolithiasis disease;
- BPH;
- hydronephrosis, ureteral stricture, etc.
1.General information
Almost all anomalies and pathological conditions of the urinary tract, taking into account its main and only function, lead to disturbances in the passage of urine, i.e. evacuation of renal blood filtration waste from the body. These are all kinds of strictures (narrowings) and obliterations (complete blockages), which are formed due to congenital or acquired reasons - anomalies of intrauterine development, infectious and inflammatory processes, urolithiasis, autoimmune sclerosing disorders (proliferation of scar connective tissue with compaction and thickening of the walls), injuries, medical interventions, cancer, etc.
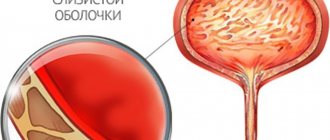
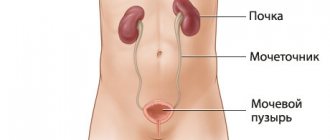
If we consider the kidney to be a source of waste to be removed, then the urinary tract actually refers to three anatomical structures: the ureter (ureter), the bladder and the urethra (urethra). Each of these formations is subject to many misfortunes; Some of them are widely known and widespread, for example, cystitis, i.e. inflammation of the bladder walls - others are quite rare. An example is a special type of ureteral stricture, which has two distinctive characteristics: firstly, localization at the mouth itself, i.e. already inside the bladder, and, secondly, a specific “swelling” of the walls of the ureter in the form of a spherical diverticulum (pouch, protrusion). This pathology is called ureterocele. Regarding the etiopathogenesis, the causes and mechanisms of development, not everything has been clarified yet, but in general, ureterocele has been quite well studied and is effectively eliminated by modern urology. According to medical and statistical data, ureterocele occurs up to three times more often in women than in men.
A must read! Help with treatment and hospitalization!
During your consultation, the urologist will answer all your questions in detail.
If you are bothered by difficulty or frequent urination, pain in the lumbar region, blood in the urine, as well as other symptoms (read about what else should alert you here), seek help from a urologist.
Admission includes:
- familiarization of the doctor with the patient’s medical history;
- inspection;
- making a preliminary diagnosis, prescribing tests and necessary procedures.
*If you plan to get tested immediately after your appointment with your doctor, go to the clinic with a full bladder.
Do not delay your visit to the clinic - come for a consultation with a urologist at the State Urology Center in Moscow - the R. M. Fronshtein Urology Clinic of the First Moscow State Medical University named after I.M. Sechenov. Entrust your health to a competent specialist!
Medicines
Photo: kvd-moskva.ru
There is no medical treatment for ureterocele as such. Medicines are necessary in the presence of complications and during preoperative preparation.
The most common complication is urinary tract infection. In this case, broad-spectrum antibiotics are prescribed: fluoroquinolones, cephalosporins, nitrofuran derivatives with adjustment of antibacterial therapy depending on the results of urine culture for bacterial flora. Anti-inflammatory therapy: diclofenac, ketorolac, nimesulide, meloxicam. Combined herbal preparations: phytohol, canephron.
Preoperative preparation also includes a course of antibiotic drugs, prevention of thromboembolic complications (unfractionated or low-molecular-weight heparin in small doses). In case of severe intoxication (temperature above 38 degrees Celsius, weakness), ureteral catheterization and infusion therapy are indicated.
Folk remedies
Photo: pinterest.fr
Ureterocele is a serious pathology, the result of which can be loss of the kidney, therefore no traditional treatment methods are acceptable.
Various folk recipes are used to treat urinary tract infections. Infusion of lingonberry leaves: 1 tablespoon of leaves per glass of boiling water, leave for half an hour. Apply three times a day.
Corn silk has an excellent diuretic effect. Pour boiling water over 2 tablespoons of crushed corn silk and leave for half an hour. Use half a glass three times a day. Before use, the infusion must be strained.
Bearberry leaves. You need to take 30 grams of leaves per 0.5 liter of water, bring to a boil and boil for 3-5 minutes. Let it brew and take a glass three times a day.
To prepare infusions, you can also use nettle leaves, birch leaves, lingonberries, red currants, juniper, elderberry, dry watermelon rind, St. John's wort, marsh calamus and rose hips. All of the above has an excellent diuretic effect, which prevents stagnation of urine, which means the development of infectious processes.
The information is for reference only and is not a guide to action. Do not self-medicate. At the first symptoms of the disease, consult a doctor.