Currently, morbidity, disability and mortality from acute pancreatitis and pancreatic necrosis occupy one of the leading places among acute surgical pathologies in young people, mainly males. One of the characteristic features of recent times is that the disease is observed among people in demand for work, which is associated with the patient’s satisfactory financial situation and, as a result, overeating, alcohol abuse and increased body weight, which in turn is the trigger of the disease and factors that complicate all types of treatment and aggravating the prognosis of the disease. According to the literature, the overall mortality rate from acute destructive pancreatitis exceeds 30%, and with the development of severe forms of complications it reaches 100%.
According to the Department of Health of the Krasnodar Territory (“Main indicators of health and healthcare of the Krasnodar Territory for 6 months of 2005”), the demographic situation in the region, as well as in the Russian Federation as a whole, remains difficult, due to the increasing depopulation of the population. In the overall structure, mortality from digestive diseases increased by 10.2%. The increase in overall mortality occurred due to the population of working age and older than working age. It should be noted that the increase in mortality from diseases of the digestive system in the Krasnodar Territory exceeds the figures for the Southern Federal District as a whole. The rate of disability in the region in 2004 increased compared to 2002-2003. and amounted to 84.2 per 10 thousand population, exceeding the Russian figure by 11%. In the structure of mortality in the region for 5 months of 2004-2005. 274 patients died from pancreatitis.
According to medical institutions dealing with the problem of destructive pancreatitis, significant progress and improvement in treatment results from the widespread use of generally accepted tactics and methods of surgical treatment have not been observed.
It is believed that the main elements of complex treatment of acute pancreatitis and pancreatic necrosis are: intensive therapy and numerous open surgical interventions on the pancreas, retroperitoneum and abdominal cavity, including those aimed at sanitizing purulent-necrotic foci. However, the fragmentation in the application of various methods of treating this extremely complex surgical pathology in the clinics of the region and the lack of necessary attention from the heads of healthcare institutions determine the stability of disappointing mortality and disability rates for patients in this group over the past decades.
More than 13 years of experience of the Russian Center for Functional Surgical Gastroenterology (FSI "RCFCHG Roszdrav"), on the basis of which the most severe patients with acute destructive pancreatitis, pancreatic necrosis, as well as literary data were supervised, indicate the need to make significant additions to the basic elements of complex treatment , without which it is impossible to overcome the crisis in the problem of treating this pathology.
The presence of our own scientific fundamental, experimental, clinical and practical developments, qualified medical personnel capable of performing the full range of modern interventions on the organs of the abdominal cavity and retroperitoneal space, conducting anesthesiology and intensive care, in combination with the latest technical advances in instrumentation, allowed scientists of the Federal State Institution "RCFHG" Roszdrav" to form a new functional unit - "Innovative Center for Emergency Pancreatology".
The Center for the Treatment of Emergency Conditions Associated with Pancreatic Pathology is the result of established functional interactions between the clinical and scientific departments of the Federal State Institution “RCFHG Roszdrav”, which ensures constant updating through the continuous implementation of scientific developments and technical improvements. Being a structural basis for the use of modern medical technologies in the treatment of destructive pancreatitis, the innovation center accumulates the main tools of visualization and intrascopic manipulation.
The pancreatology center is based on a radically changed ideology for the treatment of destructive pancreatitis, which is based on the following principles:
The principle of minimal invasiveness.
The main surgical intervention is minimally invasive (low-traumatic) surgery under intrascopic control (ultrasonic, x-ray, endoscopic).
As is known, laparotomy (opening the abdominal cavity) and lumbotomy (opening the retroperitoneal space) were required to open purulent foci in the pancreas and retroperitoneal tissue, remove necrotic tissue and sequestration. Laparotomy usually ended with the formation of a laparostomy (no sutures were placed on the wound, the abdominal cavity remained open), after which the outflow of inflammatory exudate and pancreatic secretion was ensured, through the laparotomy wound repeated access to the gland was achieved for subsequent sequestrectomies (removal of necrotic areas of the gland) and other sanitizing procedures.
Currently, all these problems can be solved without resorting to open intervention, and laparotomy, lumbotomy and laparostomy are no longer the basis of surgery for acute destructive pancreatitis. Refusal to perform open interventions on the organs of the abdominal cavity and retroperitoneal space and directly on the pancreas is the main psychological barrier for all surgical institutions that had to be overcome. It is the laparotomy itself, as a severe traumatic factor against the background of an existing catastrophe and multiple organ failure, numerous complications such as intestinal fistulas and bleeding from direct open intervention on altered tissues and organs, which are one of the main reasons for the unfavorable outcome.
The current level of development of medical technology (technological progress) allows the use of equipment exclusively for closed interventions on all organs. Intestinal, biliary, and pancreatic fistulas that arise during minimally invasive surgical treatment do not require open surgical interventions, but are available for conservative treatment.
Thus, open interventions on the abdominal cavity and retroperitoneal organs for this pathology are transferred from the rank of primary to secondary.
How is diagnostics carried out?
To diagnose the disease, doctors resort to the following methods:
- blood and urine test for alpha-amylase enzyme;
- Ultrasound of the pancreas, during which you can see swelling and affected areas;
- computed tomography, during which you can examine the heterogeneity of pancreatic tissue;
- Laparoscopy is a minimally invasive procedure during which it is possible to detect organ swelling, record the inflammatory process and differentiate the type of pathology.
Cascading principle
Minimally invasive surgical procedures are performed continuously; the end of one procedure is the start of the next one.
The development of post-necrotic complications is considered as a single, inextricable pathological process that occurs simultaneously with changes in the pancreas and surrounding tissues, and the defining feature of the course of acute destructive pancreatitis is multiple proteolytic damage to organs and toxic damage to body systems. Therefore, the patient spends most of the time in the intensive care unit, and in extremely severe cases - in the intensive care unit, where from the first day of the patient’s stay a complex of surgical and therapeutic measures is used: Syndromic correction of cardiovascular and respiratory disorders (new generation respiratory equipment - Puritan , Pulmonetic, etc.), treatment of shock and multiple organ failure. Modern methods of extracorporeal detoxification (efferent methods - plasmapheresis, plasmafiltration, hemodiafiltration, hemosorption, ultrafiltration). Antibiotic therapy of choice is the latest generation of broad-spectrum antibiotics (carbopenems, fluoroquinolones (pefloxacin) + antianaerobic drugs; III-IV generation cephalosporins + antianaerobic drugs), up to obtaining microflora sensitivity results. Early total parenteral (intravenous) nutrition before restoration of full tube feeding and early enteral nutrition.
A distinctive feature of the new approach to intensive care is the use of the latest generation of antibiotics from the first day of hospitalization and early nutrition of patients. Replacing breathing and monitoring equipment with the most modern devices and using the entire range of efferent detoxification methods make it possible to provide functional support at the stage of multiple organ failure.
When a patient approaches in the first hours of the disease, when it is not possible to unambiguously assess which “scenario” in the retroperitoneal space the disease will flow in a particular patient and whether the process will be limited or widespread, primary surgical minimally invasive intervention under ultrasound control (preventive “small-caliber” parapancreatic “drainage” ) is performed for the purpose of surgical detoxification and prevention of purulent-septic complications. In this case, it is possible to administer medicinal substances through drainage tubes, to carry out objective monitoring of the zone of pathological changes by the presence and changes in the characteristics of the exudate. By means of preventive “small-caliber” drainages, the primary outflow of inflammatory exudate is carried out.
In the case when the patient’s disease upon admission to the center has already reached the phase of purulent-septic complications, then minimally invasive surgical intervention is considered as the main surgical method for the sanitation of purulent-necrotic foci.
Popular questions about pancreatic necrosis
What kind of disease is pancreatic necrosis?
Pancreatic necrosis is a serious, life-threatening complication of acute pancreatitis, in which pancreatic tissue partially or completely dies. The condition is accompanied by severe intoxication and can lead to multiple organ failure and death.
How does pancreatic necrosis begin?
Pancreatic necrosis usually appears several hours after drinking alcohol or overeating. The first symptoms of the disease are pain in the left hypochondrium, radiating to the side, shoulder, arm, back or heart area. Acute pain is accompanied by severe intoxication, intestinal upset, and vomiting.
How long can you live after surgery for pancreatic necrosis?
Mortality during surgical intervention for pancreatic necrosis is about 50% of cases. If the patient undergoes the operation safely, he has a chance to live a full life, however, following a strict diet.
Intrascopic surgical technologies
Ultrasound examination reveals accumulations of enzymatic effusion in the abdominal cavity, omental bursa, retroperitoneal space and the zones of penetration of retroperitoneal tissue characteristic of each form of lesion. Drains with a diameter of 3 mm are installed in these areas according to the principle of “at least two in one drainage object.”
After fistulography, which assesses the nature of the spread of the process in the necrosis phase, the drains are replaced under x-ray control with double-lumen ones of larger diameter. This procedure must be repeated daily, every other day or two, depending on the specific clinical situation and the patient’s condition. Ultimately, depending on the size of the cavities being drained, drainages can reach a diameter of 5 – 20 mm. Subsequently, using a video endoscope, transfistula sanitation of retroperitoneal necrotic cavities and sequestral “fields” is performed, with correction and replacement of drainages. In this case, necrotic tissue and formed sequestration are removed.
The greater the number of “small-caliber” (thin – 1.5 – 3.3 mm in diameter) drainages are initially installed in each area of exudate and necrosis, the easier it is to perform sanitizing procedures in the future, because The location of the tube does not always allow you to change its direction or replace it with a “large-caliber” one (wider - 5 - 20 mm). In addition, in the event of a fistula of a hollow organ due to a bedsore, one of the drains can be removed without compromising the drainage of this cavity.
The use of a video fiber endoscope allows you to visualize the affected retroperitoneal space, the pancreas and objectively assess the adequacy of the removal of necrotic tissue with the possible placement of the next double-lumen “large-caliber” drainage into a hard-to-reach “pocket”, even at an acute angle to the trajectory of the first “small-caliber” drainage.
As the cavities are cleaned and their size decreases, the reverse process occurs, replacing the drains with a smaller diameter and gradually removing them until the fistula tracts are closed. Simultaneously with the introduction of new technological techniques, a restructuring of medical and nursing care is required, a change in some key principles of the formation of medical personnel and instrumental support: The principle of highly qualified medical versatility. New treatment technologies require a doctor to perform almost daily minimally invasive surgical interventions (major surgical interventions) to sanitize foci of necrosis and suppuration under combined sonographic, endoscopic and x-ray control in a cath lab under general anesthesia. Thus, a doctor who treats destructive pancreatitis using modern methods must be fluent in several specialties - surgery, intensive care, ultrasound diagnostics, X-ray diagnostics, endoscopy. A different approach - several specialists, each of whom has only his own specialty, does not allow for treatment at the required modern level, maintaining the continuity of stages of treatment and the integrity of understanding the problems of a patient with pathology of the retroperitoneal space hidden from reliable visualization. The use of one universal specialist to solve the assigned problems meets the requirements of an intensive technological approach to complex minimally invasive surgical treatment of pancreatic necrosis. The principle of manipulation hierarchy. Minimally invasive technology for the treatment of destructive pancreatitis requires hourly sanitary surgical procedures in the intensive care unit (auxiliary surgical interventions). This surgical procedure is based on the sanitation of drainage systems installed in the patient in areas of necrosis and purulent process. In the intervals between medical surgical interventions, the affected areas are washed, sanitized, and drainage systems are corrected by the medical staff of the ward. For these purposes, a highly specialized physician assistant is required. His role can be played by: a nurse with a special surgical education (currently, a system of obtaining higher medical nursing education for nursing staff on the basis of medical universities is being formed); medical assistant (surgical nurse with higher education; medical student of 3-6 years); junior doctor (intern, clinical resident, graduate student, doctor on internship, doctor with up to 3 years of experience). A feature of surgical care is the control and implementation of active fractional and constant drainage-washing and corrective procedures within 24 hours with a minimum break of 30-60 minutes. The principle of instrumental accumulation. Since minimally invasive treatment methods for pancreatic necrosis require a combination of several intrascopic methods, the equipment of the operating room and the entire treatment process must meet modern standards. The main instrumental equipment of the operating room for manipulations under intrascopic control includes a surgical ultrasound scanner, an X-ray television installation and an endoscopic stand with a system of rigid and flexible endoscopes. The complex of visualization tools required by the technology for treating pancreatic necrosis necessarily includes computed tomography or magnetic resonance imaging, as an indispensable stage in the diagnosis of certain areas of necrotic and purulent lesions that are not accessible to sonographic techniques. A necessary condition for the implementation of the above principles is a change in the doctor’s psychology to acquire the skills of minimally invasive surgical interventions on the pancreas and retroperitoneal tissue for pancreatic necrosis under combined intrascopic control. The objective result of the work of the new functional unit in the Federal State Institution “RCFHG Roszdrav” was a steady decrease in mortality. During the period of prevalence of open methods of surgical treatment of pancreatic necrosis, with an insignificant proportion of minimally invasive technologies, the mortality rate in this group of patients was more than 50%. At the same time, a third of patients died in the first 10 days after hospitalization from progressive circulatory-toxic shock, 28% of patients died within more than 60 days from arrosive bleeding. The remaining causes of mortality were mainly sepsis and multiple organ failure syndrome.
At the stage of gradual abandonment of open operations, mortality experienced a fairly steady downward trend and, despite the “neglect” of patients entering the pancreatology center, ranged from 4% to 8% in the period 2003 - 2005.
Open surgical interventions on the abdominal cavity and organs of the retroperitoneal space remained in service with the surgeons of the Center only as a means of combating massive arrosive bleeding that is not amenable to conservative and angio-roentgensurgical methods of hemostasis, or to perform colo- and ileostomy in case of acute intestinal obstruction.
Treatment of pancreatic necrosis in the traditional way
Treatment of pancreatic necrosis using minimally invasive technologies
Treatment with folk remedies
When a patient's pancreatic necrosis worsens, he experiences severe pain. Folk remedies that are used in parallel with the main treatment can help improve the condition a little. But, before practicing such methods, it is necessary to visit a doctor, establish a diagnosis and begin practicing the correct treatment regimen.
- The fruits of Japanese Sophora - a decoction is prepared from them. A spoonful of raw materials should be filled with 1 tbsp. boiling water and leave for 5 hours. Drink warm before every meal. The course of treatment is 10 days.
- Blueberry berries and leaves - a decoction is prepared from them by pouring boiling water over dried or fresh raw materials and boiling for 5 minutes. (2 tbsp. raw materials per 250 ml of water). Drink instead of tea.
- Immortelle herb - a decoction helps relieve pain and inflammation. To prepare the decoction, take 1 tbsp. l. dry herbs and a glass of water, cook for 5 minutes. Strain the resulting broth and drink throughout the day.
- Oat decoction helps relieve irritation and restore organ cells. To prepare the product, you need to soak the grains and wait a few days for them to sprout. Sprouted grains need to be dried and ground. Pour the mixture with cold water (1 tablespoon of oats per 1 glass of water) and leave for about half an hour. You need to drink 2 glasses of this product a day.
- Lemon – helps reduce pain. To do this, boil the lemon in water for 5 minutes, then squeeze the juice out of it and mix with raw yolk. Drink the product on an empty stomach and do not eat for three hours after it. Take it five times a day, once every three days. The course of treatment lasts several months.
- Licorice root - to prepare it you need to take 1 tbsp. l. chopped dry licorice root, the same amount of dandelion and burdock leaves. Pour the mixture with 2 cups of boiling water, drink the infusion hot, half a glass 3-4 times a day.
There are also special herbal mixtures used to treat the pancreas. But it is important to take into account that they bring benefits to the body if such preparations are taken regularly and according to the scheme approved by the doctor. Under no circumstances should you practice self-medication with folk remedies for such a terrible diagnosis as pancreatic necrosis.
Summary
Advantages of complex minimally invasive surgical technology for the treatment of acute destructive pancreatitis:
- Prevention of the development of pancreatic necrosis and purulent complications in destructive pancreatitis (abortive course of acute pancreatitis).
- Reduced mortality caused by bleeding, purulent-septic complications, and general surgical trauma.
- Reducing the number of complications associated with intraoperative bleeding.
- Reducing the amount of secondary intrasecretory insufficiency.
- Reducing patient disability.
- Good cosmetic effect (no laparotomy or lumbotomy scars, including those from wounds healed by secondary intention, no need for subsequent plastic surgery of skin wounds and hernias).
Author: Ph.D. Novikov S.V.
Prevention
To prevent pancreatic necrosis, you need to follow some simple recommendations:
- Limit the amount and frequency of alcohol consumption.
- Avoid junk food – fast food, processed foods, soda, and minimize the consumption of fatty and fried foods.
- Do not take medications without a doctor’s prescription, especially do not abuse them.
- Try to create a diet based on natural products, try to practice split meals in small portions.
- Treat cholelithiasis in a timely manner.
- At the first symptoms indicating problems with the pancreas, consult a doctor immediately.
- Follow the principles of a healthy lifestyle.
List of sources
- Dibirov M.D., Yuanov A.A. Pancreatic necrosis. Diagnostic and treatment protocol. Educational and methodological manual. Moscow, 2012, p. 366
- Ermolov A.S., Ivanov P.A., Blagovestnov D.A. and others. Diagnosis and treatment of acute pancreatitis. M., 2013, “VIDR”, p. 382
- Mitryakov P.S. Modern methods of treating patients with pancreatic necrosis // International Journal of Experimental Education. – 2021. – No. 9-2. – P. 221-224;
- Acute pancreatitis (Diagnosis and treatment protocols) / S.F. Bagnenko [and others]; St. Petersburg Research Institute of Emergency Medicine named after. I.I. Dzhanelidze. - St. Petersburg, 2004.
- Savelyev V.S., Filimonov M.I., Burnevich S.Z. Pancreatic necrosis. MIA, 2008, p. 259
- Sakhno V.D., Mainulov A.M., Vlasova N.V., Bochkareva I.V. Necrotizing pancreatitis, treatment protocols. Annals of Surgical Hepatology, 2005, vol. 10, no. 1, p. 107 – 112
Relevance of the problem and epidemiology
The most pressing problems of surgery remain: early prognosis of the occurrence of pancreatic necrosis, prevention of infection of the pancreas, diversity of the clinical picture (difficulties in quickly making a diagnosis), choice of surgical tactics at the early stage of pancreatic necrosis.
Another problem is the social aspect - patients’ awareness of the risk factors and the scale of this pathology. That is, deviations from the doctor’s preventive instructions are one of the most common causes of the development of acute pancreatitis and pancreatic necrosis.
Symptoms
Pancreatic necrosis has a pronounced clinical picture, so it is difficult to confuse it with another pathology. Symptoms include:
- Pain. It arises in the left side of the abdomen and radiates to the shoulder, back, groin and chest. The patient cannot describe the localization of sensations. The intensity of the pain depends on the severity of the disease.
- Nausea and vomiting. Immediately after the pain, vomiting appears, which is not associated with food intake. It doesn't bring relief. In addition to bile, the vomit contains blood clots.
- Dehydration. Since vomiting is very difficult to stop, it causes dehydration. The skin and mucous membranes become dry, diuresis decreases.
- Bloating. Since the pancreas ceases to function, the processes of rotting and fermentation intensify in the intestines. This leads to increased gas formation and bloating.
- Intoxication. Bacterial toxins circulating in the bloodstream lead to an increase in body temperature. General weakness appears, heartbeat increases.
- Paleness of the skin. At the first stage, vasoactive substances appear in the blood, which is manifested by redness of the dermis. When intoxicated, the skin turns pale, gray or jaundiced.
Complications
Pancreatic necrosis is complicated not only by purulent processes, but also by disturbances in the functioning of other organs.
The incidence of infectious complications occurs in every third patient. The likelihood of their occurrence depends on the area of the lesion. The most life-threatening are the first three weeks of illness.
Complications include:
- shock,
- peritonitis,
- abdominal abscess,
- bleeding,
- enzyme deficiency,
- ulcers,
- thrombosis,
- fistulas
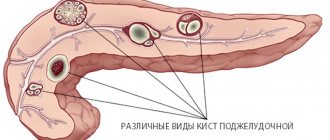
Kinds
The following types are distinguished:
- fatty,
- hemorrhagic,
- mixed.
Fatty
As the disease develops, metabolic processes and the normal functioning of pancreatic cells fail. There may be a sharp drop in blood pressure.
The disease is characterized by the rapid formation of an inflammatory infiltrate. If the disease is recurrent in nature, then such a focus may appear later. This form is formed with the participation of lipase.
This type of disease progresses slowly. Peripancreatic tissues are gradually involved in the inflammatory process. Patients with this form show fluctuations in alpha-amylase, but changes in its amount do not play a role in the pathological process itself.
Hemorrhagic
With this form, an irreversible process of cell death occurs. The form occurs during acute pancreatitis or develops during exacerbation of the chronic form.
The disease necessarily affects the secretory part of the pancreas. Its cells produce cells that are part of pancreatic juice.
The hemorrhagic form develops due to the aggressive effects of trypsin and some other enzymes that break down protein molecules.
The cause of the development of the disease may be a complex humoral process of regulation and production of digestive enzymes.
Mixed
This form is characterized by signs of several types of necrosis. Under the influence of negative factors, a sharp stimulation of the production of pancreatic juice begins. The ducts can no longer cope with the load, so the juice begins to concentrate.
Young people and middle-aged people are more prone to the disease. The mixed type does not appear at first. When symptoms appear, we are talking about the active phase.