Who is allowed or prohibited from taking Vermox?
The abstract recommends therapy if:
- alveococcosis;
- hookworm;
- ascariasis;
- capillariasis;
- strongyloidiasis;
- taeniasis;
- trichinosis;
- trichocephalosis;
- enterobiasis;
- echinococcosis.
Vermox exhibits sufficient activity against mixed helminthiasis.
The drug is contraindicated in patients:
- with liver failure;
- ulcerative colitis;
- intolerance to the component composition;
- Crohn's disease.
The medication is prohibited for use in children under 2 years of age, pregnant and lactating women.
Vermox tablets 100 mg No. 6x1
Name
Vermox tablet 100 mg in bl. in pack №6x1
Description
Round, flat, pale orange tablets, scored on one side, with a beveled edge, printed "Me/100" on one side and "JANSSEN" on the other.
Main active ingredient
Mebendazole
Release form
Pills
Dosage
100 mg
Pharmacological properties
Pharmacodynamics
Mebendazole is a broad-spectrum anthelmintic that prevents the formation of cellular tubulin in helminths, thus disrupting the utilization of glucose and the digestive functions of helminths, which leads to autolysis of the parasite.
Pharmacokinetics
Absorption. After oral administration, less than 10% of the dose reaches the systemic circulation due to incomplete absorption and extensive first-pass metabolism (first-pass effect). Maximum plasma concentrations are achieved 2–4 hours after administration. Simultaneous use of the drug with high-calorie food leads to a slight increase in the bioavailability of mebendazole. Distribution. 90–95% of the drug dose is bound to plasma proteins. The volume of distribution is 1–2 l/kg, indicating that mebendazole penetrates beyond the blood vessels. This is supported by data on the presence of mebendazole in tissues in patients on long-term therapy (eg, 40 mg/kg per day for 3 to 21 months). Metabolism. After oral administration, mebendazole is metabolized primarily in the liver. Plasma concentrations of its main metabolites are significantly higher than those of mebendazole. Impaired liver function, metabolic disorders or impaired bile secretion may lead to increased plasma levels of mebendazole. Excretion. Mebendazole, conjugated forms of mebendazole and its metabolites are partially subject to enterohepatic recirculation and are excreted in urine and bile. The half-life after oral administration is 3–6 hours in most patients. Pharmacokinetics with long-term use. With long-term use (for example, 40 mg/kg per day for 3 to 21 months), the concentration of mebendazole and its main metabolites in the blood plasma increases, resulting in an approximately 3-fold increase in the effect of the drug with long-term use compared to a single dose.
Indications for use
Vermox® is indicated for the treatment of mono- or mixed infestations caused by Enterobius vermicularis (pinworms); Ascaris lumbricoides (large roundworms
roundworms
); Trichuris trichiura (whipworm); Ancylostoma duodenale (common hookworm); Necator americanus (necator); Strongyloides stercoralis; Taenia saginata and Taenia solium (tapeworms
bovine tapeworm and pork tapeworm
).
Directions for use and doses
For enterobiasis, adults and children over 2 years of age are prescribed 1 tablet (100 mg) of the drug once. To prevent re-infestation, you should repeat taking 1 tablet (100 mg) of the drug after 2 or 4 weeks. For ascariasis, trichuriasis, hookworm or their combinations, adults and children over 2 years of age are prescribed 1 tablet (100 mg) twice a day (morning and evening) for 3 days. For taeniasis and strongyloidiasis, adults are recommended to take 2 tablets (200 mg) twice a day (morning and evening) for 3 days; Children over 2 years of age are prescribed 1 tablet (100 mg) twice a day (morning and evening) for 3 days. Information on the use of the drug in children under 2 years of age is contained in the “Children” section. The tablets can be chewed or swallowed whole, regardless of the time of meal. For young children, the tablet must be crushed before use. If the next dose of the drug was missed, then you should not double the dose during the next dose.
Use during pregnancy and lactation
Since Vermox® is contraindicated during pregnancy, patients who are pregnant or who suspect pregnancy should not use the drug. It is not known whether mebendazole is excreted in breast milk, therefore breastfeeding is not recommended when using the drug Vermox®. Ability to conceive The results of studies of the effect of the drug Vermox® on reproductive function demonstrated no effect on the ability to conceive when taken in doses up to 10 mg/kg per day inclusive. Children Used to treat children over 2 years of age. Due to the lack of experience with the use of the drug in children under 2 years of age, and also because there are isolated reports of the occurrence of seizures during the use of the drug in children of this age group, Vermox® should be prescribed only if the presence of helminthic infestation is seriously noted on the their nutritional status and physical development.
Interaction with other drugs
Concomitant use with cimetidine can lead to an increase in the effect of Vermox due to inhibition of its metabolism in the liver and an increase in the concentration of mebendazole in plasma. The simultaneous use of mebendazole and metronidazole should be avoided.
Contraindications
Vermox® is contraindicated in patients with hypersensitivity to mebendazole or any of the excipients. Vermox® is contraindicated during pregnancy.
Compound
active ingredient: 1 tablet contains 100 mg of mebendazole; excipients: microcrystalline cellulose, sodium starch glycolate (type A), talc, corn starch, sodium saccharin, magnesium stearate, hydrogenated cottonseed oil, orange flavor, colloidal anhydrous silica, sodium lauryl sulfate, orange-yellow S (E 110).
Overdose
In patients who used doses higher than recommended or were treated for a long time, alopecia, reversible liver dysfunction, hepatitis, agranulocytosis, neutropenia and glomerulonephritis were rarely observed. Such adverse reactions, with the exception of agranulocytosis and glomerulonephritis, were also observed in patients who used mebendazole in standard dosage (see section "Adverse reactions"). Symptoms. In case of accidental overdose, cramping abdominal pain, nausea, vomiting and diarrhea may occur. Treatment. There is no specific antidote. If warranted, activated charcoal may be prescribed.
Side effect
By frequency, adverse reactions that were observed are classified as follows: very often (? 1/10), often (? 1/100 to
Storage conditions
Store out of the reach of children at a temperature of 15 °C to 30 °C.
Adverse reactions
The instructions indicate that therapeutic procedures with Vermox may cause the development of non-standard responses of the body. Common side effects include:
- discomfort in the abdominal area;
- dizziness and nausea;
- dyspeptic disorders;
- cephalgia, active hair loss;
- dermatological rash, Quincke's edema;
- increased creatinine levels;
- the appearance of cylinders and blood particles in urine;
- increased activity of liver enzymes;
- anemic conditions.
Laboratory diagnostics may reveal a decrease in the number of white blood cells and eosinophils in blood tests.
Therapy methods
The instructions for the tablets indicate that Vermox should be taken after meals. The dosage of the medication depends on the type of pathological process occurring:
- enterobiasis - for patients over 10 years of age and adults: a single dose of 100 mg, if there is a risk of relapse, repeated therapy is prescribed after 14 days in a similar dosage;
- ascariasis, mixed helminthiasis, etc. – 100 mg twice a day for three days;
- trichinosis - from 200 to 400 ml daily, for 72 hours, from 4 to 10 days - from 400 to 500 mg of medication.
The annotation states that for the first 24 hours after the procedure, the patient should abstain from alcoholic beverages, fatty foods and laxatives. After completion of therapy, laboratory diagnostics are needed to determine the presence of eggs and adult helminths (carried out within a week). Long-term measures to combat parasitic organisms require regular checks of blood composition, kidney and liver functionality.
Treatment of children
Children more often suffer from enterobiasis, ascariasis, and giardiasis. Pathological processes are registered within certain age limits, the problem arises:
- due to enzyme deficiency;
- deviations in the acid-base balance of the gastrointestinal tract;
- immature motor skills;
- unstable intestinal microflora.
A child’s body becomes vulnerable after suffering from intestinal diseases and undergoing therapy with antibacterial drugs. Treatment procedures are carried out in accordance with the dosages and recommendations from the instructions for Vermox:
- Ascariasis - from 2 to 10 years, 0.5 g per day, over 11 years - 0.1 g per day. The total amount of medication is divided into three procedures. Therapy takes no more than 3 days.
- Enterobiasis - in the period of 2-5 years, a quarter of a tablet, 5-10 years - 0.5 tablets, after 11 years - a whole tablet. The medicine is given once a day, a second course is prescribed after a two-week break, maintaining the original dosage.
During medical procedures, it is necessary to wash underwear at high temperatures - above 90 degrees. The rule applies not only to the clothing of a sick child, but also to all family members.
A modern view of the problem of helminthiasis in children and effective ways to solve it
According to the World Health Organization, of the 50 million people who die annually in the world, more than 16 million are caused by infectious and parasitic diseases. In the structure of infectious diseases, intestinal helminthiases are in third place. The World Bank estimates that the economic cost of intestinal helminthiases ranks fourth among all diseases and injuries. Given the importance of the control of parasitic diseases for many countries, the 54th World Health Assembly in 2001 approved a strategy for the control of soil helminthiasis until 2010 [5].
In the Russian Federation, more than 10 million people are examined annually for helminth infections, most of them are children. In 2002, 813 thousand infected were identified, of which 681 thousand (83.8%) were children under the age of 14 [4]. More than 15 types of helminths are found in children, of which the most common are enterobiasis, ascariasis, opisthorchiasis, diphyllobothriasis, trichocephalosis, and hymenolepiasis. In recent years, toxocariasis has been increasingly recorded, which is associated with the widespread introduction into practice of a diagnostic test system for its detection.
In the structure of helminthiasis, the leading place is occupied by enterobiasis (91%) and ascariasis (8%). Among all infected children, 92.3% of cases of enterobiasis, 71.1% of ascariasis, 61.5% of trichuriasis and 66.2% of toxocariasis occur.
The incidence of enterobiasis and ascariasis in children in rural areas is significantly higher than in cities, which is apparently due to different sanitary and hygienic conditions in child care institutions in the city and village, as well as the degree of contamination of the environment with helminth eggs (Fig. 5).
Ascariasis is one of the most common helminthiasis, in the formation of foci of which soil contamination with ascaris eggs is of primary importance. In 2002, 74,196 cases of ascariasis were identified, including 52,801 in children under 14 years of age; compared to 2001, the incidence increased by 3.5% and amounted to 217.7 per 100 thousand children.
The incidence of trichuriasis, with a clear downward trend over the last decade, in 2002 increased by 2.8% and amounted to 7.4 per 100 thousand children. Trichocephalosis is registered mainly in the Southern Federal District (Republic of Dagestan, Chechen Republic).
Enterobiasis still ranks first in terms of prevalence among other helminthiases. In 2002, 614,955 cases of the disease were registered among children, which amounted to 2535.5 per 100 thousand patients.
The maximum number of people infected with enterobiasis in 2002 was identified in the Siberian, Northwestern, Ural, Far Eastern, and Volga federal districts.
A feature of most helminthiasis is the chronic course of the disease, associated with the long-term presence of the pathogen in the body and repeated repeated infections. Helminth infections in children, as a rule, are accompanied by a variety of nonspecific clinical manifestations: weakness, fatigue, irritability, sleep disturbances, dyspeptic symptoms, slower growth and weight gain, and decreased immune status. The most important component of the pathology of helminth infections is the sensitizing effect of metabolic products and excretion of helminths, leading to the development of allergic reactions in the form of atopic dermatitis, asthmatic bronchitis, rhinitis, blepharitis, etc.
A selective analysis of the results of clinical examination of 520 children, carried out in the Sverdlovsk region of Perm in 2002, showed that ascariasis was detected in 1.35%, and enterobiasis in 5.8% of those examined. At the same time, on average, the number of health problems per child in children with enterobiasis in the group of preschoolers was 2.5, and in schoolchildren - 2.9. More often than others, diseases of the genitourinary system (in girls), allergic dermatitis, anemia, vegetative dystonia syndrome, neuropathic conditions and diseases of the gastrointestinal tract were noted. Of the diseases diagnosed in children with ascariasis, the most common were vegetative dystonia syndrome, functional diseases of the gastrointestinal tract, pneumonia, and allergic dermatitis. Among children with ascariasis, the incidence rate per child averaged 2.0. In the control group, which included children without parasitic diseases (37 people), the average number of health problems was significantly lower than among those infected with ascariasis and enterobiasis, and amounted to 0.2. Thus, the presence of ascariasis and enterobiasis leads to a deterioration in the general health of children. At the same time, children with various underlying diseases that lead to weakening of the body are more often infected with them.
Let us dwell in more detail on the importance of the most common helminthiasis in the development of pathology in children - ascariasis and enterobiasis [1, 3].
Ascariasis. The development of the causative agent of ascariasis (Fig. 2, 3) in the human body occurs with the migration of larvae emerging from the eggs along the bloodstream through the lungs; the larvae are then swallowed with sputum and develop into adults in the intestine. The lifespan of roundworm in the human body is several months. Ascariasis has a significant impact on the quality of nutrition and immunological mechanisms in children. Ascaris allergen is the most powerful of allergens of parasitic origin. It can cause reactions in the lungs, skin, conjunctiva, and gastrointestinal tract. Allergic reactions can be so severe that they often pose a threat to the child’s life.
The immunosuppressive effect of roundworms is due to the lack of effect of vaccination and revaccination against measles, diphtheria, tetanus, and polioviruses in children.
The leading mechanisms of pathogenesis of the migratory stage of ascariasis are the traumatic effect of larvae and sensitization by parasitic antigens. In this case, 2 main types of lesions occur in different organs and tissues.
- The traumatic effect of migrating larvae in organs and tissues along the migration route. At the beginning of migration, the larvae are still small (no more than 0.5 mm long) and cause limited hemorrhages in the wall of the small intestine and in the liver. By the end of migration, the larvae reach 2 mm in size and, penetrating into the alveoli and bronchioles, and then into the bronchi, cause more significant hemorrhages.
- Eosinophilic inflammation of the tissues in which the larvae develop. The tissue phase of ascariasis occurs during the migration of ascaris larvae to the liver and lungs. The metabolites released in this process cause serious immunological changes and inflammatory reactions. In the migration phase, ascariasis can cause hepatomegaly and asthmatic syndrome. In this case, the clinical picture resembles respiratory allergosis.
In the intestinal phase of ascariasis, important pathogenetic factors are the ability of roundworms, reaching a length of 20–40 cm, to spiral forward movements and the desire to penetrate small openings (Vater's nipple, drainage tubes, etc.). The presence of invasion leads to hypertrophy of the muscular layers of the intestinal wall, a decrease in the depth of the crypts, changes in the chemical composition of the intestinal contents, and disruption of the motor-secretory function of the stomach and intestines. Roundworms secrete inhibitors of trypsin and chemotrypsin, as a result of which the absorption of nutrients, proteins, and fats worsens. With ascariasis, functional deficiency of pyridoxine develops, the level of retinol and ascorbic acid decreases, and lactase tolerance decreases. Ascariasis is usually accompanied by intestinal dysbiosis.
Often symptoms of the intestinal phase of ascariasis are nausea, vomiting, diarrhea, fatigue, dizziness, poor sleep, and abdominal pain. An increased level of eosinophils in the peripheral bloodstream is characteristic of the migratory phase of ascariasis.
Complications of the intestinal phase of ascariasis: intestinal obstruction caused by a ball of adult roundworms; peritonitis due to perforation of the intestinal wall or penetration of roundworms into the abdominal cavity through a surgical suture; obstructive jaundice during migration of helminths into the common bile duct; blockage of the pancreatic ducts; asphyxia due to the migration of roundworms into the upper respiratory tract.
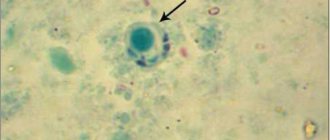
Enterobiasis. The development of the enterobiasis pathogen (Fig. 1) in the human body occurs within the gastrointestinal tract. The larvae emerge from the eggs (Fig. 4) and, on average, develop into adults within 2 weeks, which parasitize the lower parts of the small intestine and the upper parts of the large intestine. The lifespan of pinworms can reach 100 days, and the state of infestation in children due to repeated infections can last much longer.
| Figure 1. Life cycle of the enterobiasis pathogen (according to HC Jeffrey, RM Leach, 1975) |
Inflammatory reactions during enterobiasis develop under the influence of larvae, which produce hyaluronidase, proteolytic enzymes, lectin-like substances that promote the activation of the complement system, the release of prostaglandins by the cells of the host tissues surrounding the helminth [1, 2, 3].
With enterobiasis, the processes of absorption and digestion of food products are disrupted. In 30–40% of infected people, the acidity of gastric juice decreases, up to anacidosis and inhibition of pepsin-forming function. In most children, the intestinal microbiocenosis changes. Impaired absorption and digestion of nutrients in the intestines lead to weight loss and delay the growth and development of the child.
An additional factor in the pathogenesis of enterobiasis is the mechanical effect of pinworms in the intestines, leading to pinpoint hemorrhages, erosions, and penetration of bacterial flora, in particular pathogens of intestinal infections.
A striking symptom of enterobiasis is perianal itching, which occurs when the female moves during oviposition (Fig. 6). Severe itching occurs, as a rule, during sleep, more often at night, from 23.00 to 1.00 am. It is at this time that helminths can, remaining unnoticed, lay eggs that will mature to the invasive, contagious stage by the morning. Despite its apparent harmlessness, perianal itching is difficult for children to tolerate and can persist for quite a long time after enterobiasis is cured as a result of the formation of a persistent focus of excitation in the cerebral cortex. Complications that arise as a result of perianal itching are skin damage when scratching, perianal pruritis, eczema, weeping dermatitis. The etiological agent of the inflammatory process is most often streptococci.
| Figure 2. Roundworm egg (70 microns) |
| Figure 3. Adult roundworms |
| Figure 4. Pinworm egg (50–60 µm) |
Abdominal pain is a common symptom of enterobiasis. Pain of a transient nature is observed in the majority of infected people. Sometimes acute abdominal pain may be the reason to seek surgical help. In such cases, it is often not possible to detect a specific pathology; only the accumulation of gases is detected.
In recent years, the number of cases of the formation of perianal granulomas or abscesses in children, inside which female pinworms or helminth eggs were found, has increased. In this regard, it is advisable to screen all children with these conditions for enterobiasis.
In many cases, enterobiasis occurs over a long period of time and is repeated many times. As a result, the intestinal biocenosis is disrupted and the antagonistic properties of the intestinal microflora in relation to pathogens of acute intestinal infections are reduced. In the majority of infected children, the number of E. coli decreases and the proportion of lactonegative intestinal flora increases. The activity of enterokinase and alkaline phosphatase in feces increases. Since the intestinal microflora is one of the factors that supports the activity of intestinal enzymes, disturbances in the processes of digestion and absorption of nutrients that develop as a result of enterobiasis lead to loss of body weight and retard the growth and development of the child. Pinworms have a mechanical effect on the intestinal mucosa, which leads to pinpoint hemorrhages, erosions, and penetration of bacterial flora, in particular pathogens of intestinal infections. The antagonistic properties of the flora in relation to the causative agents of typhoid fever and other intestinal infections are reduced [1, 3].
If pinworms migrate into the abdominal cavity, urinary and genital tracts, inflammatory and allergic reactions outside the intestine may develop.
| Figure 5. Incidence of enterobiasis and ascariasis in urban and rural children in 2002. |
One of the common complications of enterobiasis is vulvovaginitis due to the penetration of pinworms into the genital tract and the addition of bacterial infections. If vulvovaginitis develops in a girl, a parasitological examination for enterobiasis should be prescribed and, if the result is positive, this invasion should be treated with simultaneous bacteriological examination and, if necessary, antibacterial therapy.
Against the background of enterobiasis, children often develop urinary tract infections, especially girls, since enterobiasis is a factor predisposing to the development of this complication.
Parasitism by pinworms in children leads to suppression of nonspecific immunity, manifested by a decrease in the level of interferon a in the blood serum. A decrease in the nonspecific resistance of the child’s body leads to an increase in the incidence of viral and bacterial infections.
| Figure 6. Tail end of a female pinworm |
The presence of enterobiasis leads to a decrease in the effectiveness of preventive vaccinations. The immune layer against diphtheria was initially lower among children infected with pinworms. Protective immunity does not develop during primary vaccination against this dangerous infection, and during revaccination in many cases there is no immune response. It is difficult to develop immunity when vaccinated against measles and tetanus, so to increase the effectiveness of vaccinations, you first need to make sure that the child’s body is free from helminthiasis pathogens.
In children with allergic diseases, enterobiasis develops much more often. Due to the relatively high probability of detecting enterobiasis in children with allergic diseases, patients in this group should be recommended to be examined for enterobiasis and deworming if infestation is detected.
Enterobiasis negatively affects the neuropsychic development of children. This invasion leads to a lag behind the corresponding age norms. Among those infected with enterobiasis, there is a high percentage of irritable children, with a disruption in the process of falling asleep, and with negative habits (biting nails, sucking fingers, etc.).
With enterobiasis in children, the level of copper, zinc and magnesium in the blood decreases significantly. Since the lack of these microelements can negatively affect the physical and mental development of children, their loss should be compensated by introducing certain foods into the child’s diet, prescribing medications (or nutritional supplements) until these indicators are normalized after enterobiasis is cured.
Main indications for examination for helminth infections:
- stomach ache;
- frequent nausea, vomiting;
- diseases of the gastrointestinal tract;
- fatigue, irritability, restless sleep, grinding teeth in sleep;
- allergic conditions;
- perianal itching (enterobiasis);
- vulvovaginitis (enterobiasis);
- urinary tract infections (enterobiasis);
- increased level of eosinophils in the blood;
- retardation in height, weight;
- untidiness.
The diagnosis of enterobiasis and ascariasis is made only upon receipt of positive results from a laboratory parasitological examination of the patient. If enterobiasis is suspected, a perianal scraping (imprint) is examined, and fecal samples are examined for ascariasis. On the laboratory referral form, you should indicate what kind of helminthiasis the doctor suspects in the child. The choice of the most effective research method by laboratory specialists will depend on this.
Treatment of ascariasis and enterobiasis
The search for remedies for the treatment of helminthiases, including enterobiasis and ascariasis, began many centuries ago. To expel pinworms, Ibn Sina recommended taking elecampane and celandine with sugar, washing them down with water. The medicine for expelling worms (“killing worms”), indicated in the Ebers Papyrus, contains, among other components, date seeds and the plant disart, sweet beer. The Salerno Health Code, which dates back to the early 16th century, recommends another remedy: mint [3].
The modern arsenal of drugs used to treat intestinal helminthiases includes a significant number of drugs of various chemical classes. They are used both in clinical practice for the treatment of identified patients or parasite carriers, and for the purpose of mass prevention.
The Russian pharmaceutical market currently offers several anthelmintic drugs that act on the causative agents of ascariasis and enterobiasis (Table 1).
The most effective drugs for the treatment of enterobiasis and ascariasis are derivatives of carbamate benzimidazole (mebendazole, medamine) and tetrahydropyrimidine (pyrantel). In addition to the ability to influence mature forms of helminths, they are distinguished by high ovicidal and larvicidal activity. Drugs of these pharmacotherapeutic groups disrupt oxidative processes, inhibit glucose transport in helminths, act on the muscles of intestinal nematodes by depolarizing their neuromuscular junctions and block the action of cholinesterase.
The effectiveness of medicines used to treat enterobiasis and ascariasis is very high, the method of administration is very simple and is designed primarily for children. It is very important that as a result of their intake, the process of releasing the pathogen into the environment is not activated. Thus, during treatment the person does not become more dangerous to others. However, pinworm eggs that have already entered the environment, in particular indoors, persist for a long time - more than 2 weeks. Therefore, it is recommended to repeat the treatment of enterobiasis after 2-3 weeks at the same dose in case hygienic measures were not effective enough. For the same reason, simultaneously with the treatment of infested people, everything possible must be done to clear the premises of pathogens.
For many years, pyrantel has been used throughout the world to treat ascariasis and enterobiasis, and has gained popularity among pediatricians and patients. According to recommendations developed in the USA (Medical Letter, 2002), pyrantel is considered a first-line drug for the treatment of enterobiasis in children and adults.
The anthelmintic effect of pyrantel pamoate is associated with a stimulating effect on the H-cholinergic receptors of the ganglion synapses of helminths, leading to spastic paralysis and their subsequent expulsion from the human body. Clinical trials of the effectiveness and tolerability of pyrantel showed its high medicinal activity against enterobiasis and ascariasis - 94-100%, as well as good tolerability [1, 3].
Pyrantel for the treatment of enterobiasis is prescribed at a rate of 10 mg/kg per day once during or after meals. For the treatment of ascariasis, pyrantel is prescribed at a dose of 5 mg/kg once. The drug is well tolerated by children; in some cases, nausea, vomiting, diarrhea, abdominal pain may develop; very rarely, a transient increase in the activity of liver transaminases, headache, dizziness, and sleep disturbances may occur. Pyrantel is contraindicated in children with liver disease.
We have extensive experience in treating enterobiasis in children with the drug Pyrantel (tablets, suspension). Pyrantel is well known on the world market of anthelmintic drugs and is widely used for the treatment of enterobiasis in Russia by many generations of doctors. In our opinion, this drug has a number of advantages compared to other anthelmintic drugs. Firstly, the drug in the form of a suspension is easy to give to children, secondly, Pyrantel has a pleasant peach taste, as a result of which the child does not experience negative emotions during treatment, and, finally, thirdly, Pyrantel has a reasonable price and is widely sold in pharmacies. The bottle is equipped with a measuring spoon with a division scale of 2.5 and 5.0 ml, which makes it easy to dose the drug depending on the body weight of the infected child (or adult). Pyrantel suspension can be used in children from 6 months of age.
Along with pyrantel, mebendazole and medamine have a good anthelmintic effect against enterobiasis and ascariasis.
Mebendazole (Vermox) for the treatment of enterobiasis is prescribed to children 2–5 years old at the rate of 5 mg/kg per day, over 5 years old - 100 mg per day. For the treatment of ascariasis in children 2–5 years of age, the drug is prescribed at a dose of 5 mg/kg in 2 doses per day for 3 days; for children over 5 years of age, mebendazole is prescribed at a dose of 10 mg/kg per day in 2 doses for 3 days.
Mebendazole is not recommended for use in the first trimester of pregnancy. It must be remembered that the drug is contraindicated in children under 2 years of age. Side effects of mebendazole include abdominal pain and loose stools.
Medamine (2-medoxycarbanylamino-benzimidazole) is close in chemical structure and spectrum of anthelmintic action to mebendazole. For the treatment of enterobiasis, it is prescribed at a dose of 10 mg/kg per day in 2-3 doses (simultaneous administration is also possible) after eating a small amount of food; it is recommended to chew the tablets and wash them down with water. For the treatment of ascariasis, medamine is prescribed in the same doses for 3 days.
Side effects of medamine include nausea and weakness. In case of allergic manifestations, the drug is discontinued. Medamin is contraindicated in the first trimester of pregnancy.
To restore the microbiocenosis of the colon in patients with intestinal nematodes, including enterobiasis and ascariasis, and to increase the effectiveness of specific therapy, it is recommended to prescribe bificol, milk bifidum-bacterin. Food products and medicinal plants that can be used for the treatment and prevention of enterobiasis have long been known. Carrots and carrot juice have a good anthelmintic effect. You can also use the anthelmintic activity of walnuts, wild strawberries, pomegranate (especially pomegranate juice), garlic and lovage.
Among the medicinal plants, St. John's wort is used in the form of decoctions and infusions, tea, as well as elecampane (Inula helenicum). The effectiveness of herbal medicine for enterobiasis is low, but the introduction of foods with anthelmintic effects into the diet is a good measure for the prevention of enterobiasis and enhances the effect of medications prescribed by a doctor.
The criteria for the effectiveness of treatment of helminthiases are a negative result of a control parasitological study of fecal samples (for ascariasis) and a perianal scraping or print (for enterobiasis), as well as the disappearance of clinical symptoms of invasion.
Prevention of helminthiases
Features of the prevention of helminthiases depend on the characteristics of their epidemiology. With enterobiasis and ascariasis, the only source of infection is humans. Infection occurs when mature infective helminth eggs are ingested. However, the epidemiology of these helminthiases is otherwise very different. Pinworm eggs mature indoors and on the human body within a few hours and last on average up to 1 month on various household items. Ascaris eggs mature when dropped into the soil within several months and remain there for up to 10 years or more. Enterobiasis is transmitted indoors from one person to another mainly through dirty hands, bed and underwear, toys, dishes and other household items contaminated with pinworm eggs.
A person becomes infected with ascariasis by ingesting soil particles containing invasive roundworm eggs (with unwashed vegetables, herbs, and fruits). The risk of infection (in the case of ascariasis) increases if a child has such a bad habit as geophagy (tasting or eating earth, sand, clay), which occurs quite often (in 3-10% of children under 7 years of age).
Prevention of enterobiasis and ascariasis is the most important task of medical and educational institutions and parents. It can be solved by simultaneously implementing a set of measures, the main components of which are the identification and treatment of infected people and sanitary and hygienic measures. Prevention of ascariasis, enterobiasis and other helminth infections in the Russian Federation is regulated by new sanitary standards and rules approved by the Ministry of Health of the Russian Federation in 2003.
For questions regarding literature, please contact the editor.
T. I. Avdyukhina, Candidate of Medical Sciences, Associate Professor T. N. Konstantinova, Candidate of Medical Sciences, Associate Professor M. N. Prokosheva RMAPO, Moscow Children's Clinical Hospital named after. P. I. Pichugina, Perm
Symptoms of overdose, nuances of interaction
If the recommended amount of Vermox is accidentally exceeded, patients experience the appearance of non-standard symptoms. Patients complain:
- for discomfort in the abdominal area;
- attacks of vomiting with nausea;
- dyspeptic disorders.
High dosages with long-term use can provoke the development of hepatitis, neutropenia, and liver dysfunction. First aid consists of gastric lavage and the use of sorbents. Complex intoxications require symptomatic therapy.
The instructions indicate the possible interaction of Vermox and other agents with the subsequent occurrence of effects:
- combination with Cimetidine – increases the amount of mebentazole, reduces the volume of carbamezine in the blood;
- combination with insulin drugs requires a reduction in their dose.
The abstract advises avoiding the simultaneous use of Vermox and lipophilic drugs.
Vermox 100 mg No. 6 tablet.
Instructions for medical use of the drug VERMOX Trade name Vermox International nonproprietary name Mebendazole Dosage form Tablets 100 mg Composition One tablet contains the active substance - mebendazole 100 mg excipients: sodium lauryl sulfate, colloidal anhydrous silicon dioxide, magnesium stearate, sodium saccharin, talc, corn starch, lactose monohydrate. Description Tablets, white or almost white, flat, disc-shaped with a bevel, with the inscription “Vermox” on one side and a score on the other, with a slight characteristic odor, about 10.0 mm in diameter. Pharmacotherapeutic group Preparations for the treatment of nematodes. Benzimidazole derivatives ATC code P02 CA 01 Pharmacological properties Pharmacokinetics Poorly absorbed after oral administration. The bioavailability of a conventional anthelmintic dose is insufficient due to low solubility and intensive primary metabolism. 90% of the absorbed fraction binds to plasma proteins. Bioavailability increases when taking the drug simultaneously with fatty foods. It is excreted mainly unchanged in feces. Pharmacodynamics Broad-spectrum antihelminthic agent. It disrupts the tissue respiration of worms and causes degeneration of the cytoplasmic microtubules of the worm, prevents the utilization of glucose, reduces energy metabolism, reduces the formation of ATP in tissues and thereby causes irreversible muscle paralysis and death of the parasite. Indications for use Diseases caused by infections: - enterobiasis (Enterobius vermicularis) - ascariasis (Ascaris lumbricoides) - trichinosis (Trichuris trichiura) - hookworm disease (Ancylostoma duodenale) - necatoriasis (Necator americanus) - strongyloidiasis (Strongyloides stercoralis) - taeniasis (Taenia spp) and mixed infections. Method of administration and dosage For enterobiasis, children from 6 to 10 years old - 25-50 mg per day in one dose for 3 days. Children over 10 years of age and adults, regardless of body weight, take 100 mg of the drug (1 tablet) once. Treatment should be repeated after 2-4 weeks, due to frequent relapses of infection. Simultaneous treatment of all family members is recommended. For ascariasis, trichinosis, hookworm and mixed infections: adults, 200 mg/day for 3 days. (1 tablet morning and evening). Children from 6 to 10 years old - 25-50 mg per day in one dose for 3 days. For taeniasis, strongyloidiasis: - adults for three days, 2 tablets morning and evening (400 mg/day); - children for three days, one tablet in the morning and evening (200 mg/day). Maximum single doses - for children from 6 years to 10 years - 50 mg, for children over 10 years - 100 mg, for adults - 200 mg, daily doses for children under 10 years - 50 mg, for children over 10 years - 200 mg , for adults - 400 mg. Side effects - dizziness, headache, weakness, drowsiness, muscle incoordination Rarely - convulsions in infants - nausea, vomiting, abdominal pain, diarrhea - allergic reactions (urticaria, angioedema, angioedema) - toxic epidermal necrolysis, Stevens syndrome - Johnson, rash - neutropenia When used in high doses for a long time: - impaired liver function, hepatitis - glomerulonephritis Contraindications - hypersensitivity to any of the components of the drug - impaired liver function - hereditary intolerance to galactose, lactose, lactase deficiency, glucose malabsorption /galactose - pregnancy and lactation - children under 6 years of age Drug interactions Simultaneous administration of cimetidine with Vermox increases the concentration of the latter in plasma during long-term treatment. It is recommended to determine plasma concentrations of the drug to ensure the required doses of both drugs. The simultaneous use of mebendazole and metronidazole should be avoided. Special instructions For long-term use, monitoring of general blood count, liver and kidney function is necessary. The drug is incompatible with alcohol. During the treatment period there is no need to prescribe laxatives or follow a diet. Vermox reduces the need for insulin in patients with diabetes. In case of lactose intolerance, please note that each tablet of the drug contains 110 mg of lactose monohydrate. Peculiarities of the drug's influence on the ability to drive a vehicle and operate potentially dangerous machinery. Vermox does not affect the ability to drive a car or control working mechanisms. Overdose Symptoms: spasmodic abdominal pain, nausea, vomiting, diarrhea. Treatment: there is no specific antidote. In the first hour after an overdose - gastric lavage, taking activated charcoal. Release form and packaging 6 tablets in a blister pack made of polyvinyl chloride film and aluminum foil. 1 contour package along with instructions for medical use in the state and Russian languages is placed in a cardboard box. Storage conditions Store at temperatures from 15 ºС to 30 ºС. Keep out of the reach of children! Shelf life: 5 years Do not use after expiration date. Conditions for dispensing from pharmacies By prescription Name and country of the manufacturing organization Gedeon Richter Romania A.O., Romania Name and country of the owner of the registration certificate JSC Gedeon Richter, Budapest, Hungary Name and license holder Janssen Pharmaceutica, Belgium Address of the receiving organization in the Republic Kazakhstan claims from consumers regarding product quality Representative office of JSC Gedeon Richter in the Republic of Kazakhstan E-mail Telephone: 8-(7272)-58-26-22, 8-(7272)-58-26-23
Analogs
The occurrence of adverse reactions to therapeutic measures requires stopping treatment and replacing the drug. Popular analogues of Versmox are presented:
- Vormin, Vero-Mebendazole;
- Vermakar, Mebex;
- Mebendazole, Telmox 100.
The choice of a suitable substitute is the responsibility of the therapist. The doctor is based on the causes of intolerance to the drug and selects a safer analogue.
Reviews
On the forums there are positive responses from patients who have been treated with anthelmintic medications. The effectiveness of Vermox for children and adults is proven by the results obtained. Parents believe that the medicine is more effective than analogues, but due to its toxicity it is not suitable for prophylactic use.
Patients note that accurate implementation of the therapy regimen allows you to quickly get rid of painful sensations in the abdomen and normalize the functioning of the gastrointestinal tract. In rare cases, negative reviews are associated with the development of side effects during procedures.