Syphilis: symptoms and first signs, how to treat syphilis
Symptoms of syphilis depend on the stage of the disease, age and gender of the patient. The course of this venereal chronic disease may have its own characteristics in each specific case. It is even capable of being asymptomatic for the time being in a latent state.
A distinctive feature of treponema pallidum is its exceptional contagiousness, which is why it is so important to survey the population in order to avoid an epidemic of this disease.
The worst thing is when it has a hidden course and the person does not even realize that he is a carrier of syphilis and poses a danger to his family and others.
How is it transmitted?
Syphilis is caused by Treponema pallidum, which lives in the external environment for only 3 minutes. Therefore, the main route of transmission of the disease is sexual. Infection of the fetus is possible in utero (vertical route) or intrapartum, when the child passes through the mother’s birth canal.
The household route of transmission is uncommon; infection is possible from persons with the tertiary stage of syphilis, when treponema pallidum gets on dishes, linen, towels, etc. from decaying gums. Hematogenous transmission of syphilis through blood transfusion cannot be ruled out.
Cases of infection of medical workers through contact with the blood of a patient are not that rare. It is possible to become infected through “bloody” objects: a shared toothbrush, razor, manicure set, etc.
Causes
Syphilis is caused by a bacterium called Treponema pallidum.
Treponema pallidum
Infection most often occurs through sexual contact, somewhat less often - through blood transfusion or during gestation, when the bacterium falls from mother to child.
Bacteria can enter the body through small cuts or abrasions on the skin or mucous membranes. Syphilis is contagious during its primary and secondary stages, and sometimes during the early latent period.
Syphilis is not spread by sharing toilets, bathtubs, clothing or utensils, through door handles and swimming pools.
After treatment, syphilis itself does not recur, but you can become infected again by coming close to an infected person.
Risk factors
You are at increased risk of contracting syphilis if you:
- participated in unprotected sex;
- participated in sex with multiple partners;
- a man who has sex with men;
- infected with HIV, the virus that causes AIDS.
Syphilis - incubation period
The incubation period is a period of illness that lasts from the moment Treponema pallidum enters the body until the appearance of the first signs of syphilis (see photo), including chancre in combination with regional lymphadenitis. During this period, there is a gradual increase in the number of pathogen cells at the site of their introduction into the patient’s body. Treponema reproduces by division on average once every 30-32 hours.
This period of the disease is characterized by the absence of registered clinical and serological changes in the patient’s body; it lasts on average 3-4 weeks, it can be shortened to 8-15 days or lengthened to 108-190 days. A shortening of the incubation period occurs, as a rule, when the body is simultaneously infected from 2 sources; it is lengthened when taking antibiotics after the moment of infection, for example, for a sore throat, although it should be noted that an increase in the incubation period is not always due to the use of antibiotics.
Publications in the media
Syphilis is an infectious disease caused by Treponema pallidum, transmitted primarily through sexual contact, with a chronic relapsing course and a characteristic periodicity of clinical symptoms, which can affect all organs and systems. Frequency . In Russia in 2001, the incidence was 143.6 per 100,000 population.
Classification • Primary syphilis •• Seronegative •• Seropositive • Secondary syphilis •• Fresh •• Recurrent •• Latent • Tertiary syphilis •• Active •• Latent • Latent syphilis •• Seropositive early •• Seropositive late • Congenital early syphilis •• Late • • Latent • Neurosyphilis • Visceral syphilis.
Etiology. The causative agent is pale treponema (Treponema pallidum), spiral-shaped, 4-14 microns long and 0.2-0.25 microns in diameter, has 8-12 uniform curls, can exist in three forms - spiral, cystic and L-form. The most common (classical) course of syphilis is due to the presence of a spiral form of the pathogen; other forms probably maintain a long latent course.
Epidemiology. The source of infection is a sick person. Conditions of infection: the presence in the material from the patient of a sufficient number of virulent Treponema pallidum and violation of the integrity of the skin and mucous membrane. The main route of infection is direct contact (usually sexual) with a sick person. With congenital syphilis, infection occurs in utero - through the vessels of the placenta. Treponema pallidums that have entered the body spread through the lymphatic system, actively multiply and enter various organs and tissues, which causes certain manifestations of the disease. Over time, the number of Treponema pallidum in the patient’s body decreases, but the tissue reaction to the pathogen becomes more violent. They admit the possibility of a long (many years) asymptomatic course of syphilis from the very beginning of the disease with the subsequent development of damage to the nervous system and visceral forms of the disease.
CLINICAL PICTURE. In untreated patients, acquired syphilis lasts for many years. In the classical course of the disease, there are 4 periods: incubation, primary, secondary, tertiary.
The incubation period lasts from the moment of infection until the appearance of the first clinical symptom - chancre (on average - 20-40 days). Sometimes it is reduced to 10–15 days with massive infection, which is accompanied by multiple or bipolar chancre, as well as with superinfection. An extension of the incubation period to 3–5 months is often observed with severe concomitant diseases or after treatment with low doses of antibiotics.
Primary period
• Continues from the moment of appearance of chancroid until the appearance of generalized rashes (6–7 weeks). It is characterized by the development at the site of penetration of pale treponema (usually in the genital area), chancre (ulсus durum, primary syphiloma) and regional lymphadenitis.
• Clinical signs of chancre •• Erosion (or ulcer) with the absence of acute inflammatory phenomena •• Regular round or oval outline, clear boundaries •• Size of a small coin •• Raised above the surrounding healthy skin (mucous membrane) •• Smooth, shiny, bluish-red bottom, flat (saucer-shaped) edges •• Scanty serous discharge •• Densely elastic (cartilaginous) infiltrate at the base, painlessness •• Chancre is often single, multiple chancre is rarely observed (in about 20% of patients) •• Atypical hard ones are also isolated chancre: indurative edema (painless dense swelling of the foreskin or labia), chancre-amygdalitis (dense swelling of the tonsil) and chancre-felon (simulates ordinary felon).
• Chancre can be complicated by a secondary infection: acute inflammatory reactions in the circumference of the chancre (if localized in the genital area - vulvitis or balanoposthitis, often leading to phimosis or paraphimosis). When complicated by fusospirillosis symbiosis, necrosis of the bottom and edges (gangrenization) of chancre occurs. Repeated gangrenization (phagedenism), usually observed in persons suffering from alcoholism, leads to significant tissue damage.
• Regional lymphadenitis (accompanying bubo, regional scleradenitis) is the second obligatory symptom of primary syphilis, occurs 7–10 days after the appearance of chancre •• Enlargement and hardening of the lymph nodes closest to the chancre •• When chancre is localized on the genitals, the inguinal lymphatics undergo changes nodes: they are enlarged to the size of a bean, sometimes larger, dense, not fused to each other and to the surrounding tissues, mobile, painless on palpation, the skin over them is not changed •• Characterized by enlargement of several lymph nodes. Scleradenitis can be bilateral or unilateral. Sometimes a strand of regional lymphangitis can be seen and palpated between the chancre and enlarged lymph nodes. •• At the end of the primary period, specific polyadenitis develops (moderate enlargement of all groups of lymph nodes), sometimes low-grade body temperature and general weakness are noted.
Secondary period
• Characterized by generalization of infection and lasts 3–4 years.
• All organs and systems can be affected, but the main manifestations are rashes on the skin and mucous membranes (secondary syphilides). The rashes of each of the attacks of the secondary period, having existed for about 1.5–2 months, undergo spontaneous regression, and after a more or less long latent period they appear again.
• The first rash, which marks the beginning of the secondary period, is particularly bright and abundant in the rash (secondary fresh syphilis). It is usually accompanied by fading chancroid and pronounced polyadenitis.
• Repeated episodes of rashes (secondary recurrent syphilis) alternate with periods of complete absence of manifestations (secondary latent syphilis). The rash with secondary recurrent syphilis is less abundant and tends to cluster. In the first half of the year, the rashes are accompanied by gradually fading polyadenitis.
• Secondary syphilides have a number of common features that distinguish them from other skin rashes: they are ubiquitous, have a benign course, there are no febrile symptoms, there are also no acute inflammatory phenomena and subjective sensations, they are resistant to local treatment, and quickly disappear under the influence of therapy. In the secondary period, 5 groups of syphilides are distinguished •• Syphilitic roseola (observed in 75–80% of patients): a pink spot 0.5–1 cm in size, irregularly rounded in outline, does not peel off, disappears with pressure •• Syphilitic papule (observed just as often , like roseola): a bluish-red nodule of dense consistency with peeling along the periphery (Biette's collar). Varieties of syphilitic papules ••• Lenticular (lenticular): size 0.3–0.5 cm ••• Miliary: the size of a poppy seed ••• Nummular (coin-shaped): the size of a large coin, tendency to cluster ••• Seborrheic: localized on the face, forehead skin and is distinguished by oily scales on the surface ••• Erosive (weeping): characterized by an erosive or weeping surface, localized on the mucous membrane or in the folds of the skin ••• Condylomas lata (vegetative papules) are located in places of skin friction (inguinal region), are distinguished by their large size, vegetation, erosive surface ••• Horny papules of the palms and soles are characterized by a powerful development of the stratum corneum on the surface, very reminiscent of calluses ••• Psoriasiform papules: pronounced peeling on the surface •• Syphilitic pustule (rarely observed): noted in weakened patients with a severe (malignant) course of the process. Clinical varieties: acne, smallpox, impetiginous, syphilitic ecthyma, syphilitic rupee •• Syphilitic baldness - rapidly developing small-focal or diffuse hair loss on the head without inflammatory changes in the skin, usually observed in the second half of the disease •• Syphilitic leukoderma (syphilide pigmentosa), more often noted in women, it is localized on the lateral and back surfaces of the neck (necklace of Venus), often on the skin of the torso; On the affected areas, against the background of hyperpigmentation, hypopigmented round spots 0.5–1 cm in size appear.
• The mucous membrane of the pharynx is often affected, where syphilitic tonsillitis occurs (erythematous, papular and pustular-ulcerative), differing from ordinary tonsillitis by sharp boundaries, the absence of acute inflammatory reactions, fever and pain. With rashes on the vocal cords, hoarseness of the voice is noted.
• With secondary syphilis, damage to internal organs, the central nervous system, bones, joints, organs of vision, hearing, etc. is possible. •• Bone damage is noted in 5% of patients in the form of diffuse periostitis with painful swelling, night pain in the bones; osteoperiostitis is observed less frequently. The bones of the skull and tibia are most often affected •• Joint damage usually occurs as a polyarthritic synovitis with the formation of effusion in the joint cavity •• The most important specific lesions of the internal organs of the secondary period include syphilitic hepatitis (enlarged and painful liver, increased body temperature, jaundice) , gastritis, nephrosonephritis, myocarditis •• Damage to the central nervous system in the secondary period is called early neurosyphilis. Damage to the meninges and blood vessels is typical. During a neurological examination, as well as during the analysis of cerebrospinal fluid, syphilitic meningitis (often asymptomatic), syphilis of the brain vessels (meningovascular syphilis), rarely - syphilitic neuritis and polyneuritis, neuralgia are diagnosed.
Tertiary period
• Develops in approximately 40% of patients in the 3rd–4th year of the disease and continues indefinitely. The transition of the disease to the tertiary period is facilitated by inadequate treatment or its absence, severe concomitant diseases, alcoholism, etc.
• Distinctive features of the tertiary period are the appearance of false inflammatory infiltrates in the form of tubercles and gummas, prone to decay, followed by extensive destructive changes in the affected organs and tissues; productive nature of inflammation with the formation of infectious granuloma; a small number of rashes (the number of tubercles is in the tens, gumma - in units); ubiquity of lesions, undulating course.
• In case of clinical manifestations, tertiary active syphilis is diagnosed; in the absence of such, tertiary latent syphilis is diagnosed.
• Relapses of tertiary lesions are observed infrequently, they are separated from each other by a long (sometimes many years) latent period. The lifespan of tertiary syphilides is calculated in months or years; they are characterized by low infectivity due to the small number of pale treponema in the tissues. Classic serological reactions are negative in 30% of patients with tertiary syphilis. The skin, mucous membrane and skeletal system are most often affected. Skin lesions are represented by tubercular and gummous syphilides.
• Tuberous syphilide is a small dense tubercle located in the thickness of the skin, hemispherical in shape the size of a cherry pit, bluish-red in color. After a few weeks or months, the tubercle softens and ulcerates to form a round, rather deep ulcer, with smooth, steep, dense edges. Gradually, the ulcer epithelializes and turns into an atrophic scar pigmented along the periphery, on which new rashes never appear.
• Gummous syphilide (gumma) is a node of dense consistency the size of a walnut, rising above the skin level, painless on palpation, not fused with the surrounding tissues. The skin over it is initially unchanged, then becomes bluish-red. Subsequently, the gummous node softens in the center and is opened with the release of a glue-like exudate. The resulting defect quickly increases in size and turns into an ulcer. It is painless, clearly demarcated from the surrounding skin by a ridge of dense, undisintegrated gummous infiltrate, its edges are steep, the bottom is covered with necrotic masses. A gummous ulcer lasts for months, and with secondary infection - even years. After the gumma heals, a characteristic star-shaped scar remains. In some cases, the contents of the gum are replaced by fibrous tissue with the formation of dense nodes. Gummas of the mucous membranes are often noted. Most often the membrane of the nasal cavity is affected, then the pharynx. Gummous lesions of the tongue, hard and soft palate, nose, pharynx, larynx lead to severe, often irreparable disturbances in speech, swallowing, breathing, and change the appearance of the patient (saddle nose, complete destruction of the nose, perforation of the hard palate). Among gummous lesions of other organs, syphilides of the periosteum, bones and joints are most often observed; The bones of the legs, forearms, skull, knee, elbow and ankle joints are affected.
Congenital syphilis is transmitted to the fetus of a sick mother through the placenta, mainly in the first 3 years after the mother is infected.
• Pregnancy outcomes with syphilis: late miscarriages, premature births, full-term births. Stillbirths are frequently reported. Children are born with active manifestations or latent syphilis.
• Depending on the duration of the syphilitic infection, periods of congenital syphilis are distinguished: fetal syphilis, early congenital syphilis (infant syphilis and early childhood syphilis are distinguished), late congenital syphilis (after 4 years) •• Fetal syphilis (fetal damage by syphilis occurs at fifth month of pregnancy) is accompanied by changes in internal organs, and somewhat later in the skeletal system. Specific lesions of the internal organs of the fetus are manifested by intercellular infiltration and proliferation of connective tissue. Widespread and severe lesions of the internal organs of the fetus often lead to late miscarriages and stillbirths •• Early congenital syphilis can first appear both in infancy (up to 12 months) and in early childhood (1–4 years) ••• Syphilis in infants most often manifests itself in the first 3 months of life and is very unique. In children born from untreated mothers with active manifestations of secondary syphilis, congenital syphilis is an extremely severe disease affecting almost all internal organs, the central nervous system and specific changes in the skin and mucous membranes ••• An early manifestation of syphilis in this period is syphilitic pemphigus. The rashes are localized mainly on the skin of the palms and soles, less often on other areas of the skin. Bubbles the size of a pea and a cherry are initially serous, then purulent, sometimes hemorrhagic, located on an infiltrated base and surrounded by a zone of specific papular infiltrate of a bluish-red color ••• Diffuse Hochsinger infiltration is usually localized on the soles, palms, face and scalp. The lesion is clearly demarcated, with a smooth shiny surface of bluish-red color; is distinguished by a densely elastic consistency, leading to the formation of cracks that have radial directions in the circumference of the mouth and leave lifelong radiant Robinson-Fournier scars ••• Widespread or limited roseolous, papular and pustular rashes in all their varieties, similar to those in the secondary period of syphilis, are also observed. Skin rashes are often preceded by an increase in body temperature ••• Damage to the mucous membranes often occurs in the form of a syphilitic runny nose: specific erosive-papular hyperplastic anterior rhinitis. Breathing through the nose becomes extremely difficult, which makes the act of sucking impossible. As a result of ulceration of the papular infiltrate of the nasal septum, its destruction with deformation of the nose is possible ••• Lesions of the skeletal system: lack of active movements in the limbs and pain in passive movements, caused by the formation of gummas in the epimetaphyses of long tubular bones with a tendency to fractures (Parro’s pseudoparalysis, Wegner’s disease) • •• Specific lesions of internal organs often begin in utero; their diffuse nature causes severe congenital syphilis and significant mortality in the first weeks and months of a child’s life. Liver damage is detected in the form of its enlargement and thickening. Rarely, jaundice is noted with atrophic cirrhosis of the liver. Damage to the spleen is often observed. Specific lung damage in the form of white pneumonia is rarely recorded; often occurs as a complication of pneumonia of various etiologies. Kidney damage (glomerulonephritis, nephritis, nephrosonephritis) is noted in 14% of patients. The cardiovascular system is affected early, but rarely (myocarditis, endocarditis, pericarditis) ••• One of the most common lesions of the central nervous system is specific meningitis with convulsions, paralysis and anisocoria. Increased cytosis, an increase in the amount of protein, and positive globulin reactions are noted in the cerebrospinal fluid. Some children develop hydrocele at 2–3 months of age. Among the sense organs in infants, the eyes are affected. Already at the birth of a child, it is possible to detect changes in the retina and macular membrane (chorioretinitis), damage to the optic nerve ••• Limited large-papular (usually weeping) rashes such as condylomas lata are often observed on the skin, erosive papules are often observed on the mucous membranes; bones are often affected (syphilitic periostitis of long tubular bones) •• Late congenital syphilis appears at the age of 5–17 years and resembles the tertiary period of syphilis in its clinical manifestations. Signs of late congenital syphilis are divided depending on the degree of specificity into absolute, or unconditional; relative, or probable (observed more often with late congenital syphilis, but also noted with other diseases); dystrophies (can be a consequence of both congenital syphilis and other diseases) ••• Absolute signs include Hutchinson’s triad: Hutchinson’s teeth (barrel-shaped or chisel-shaped incisors, hypoplasia of the chewing surface with a semilunar notch along the free edge), parenchymal keratitis (uniform milky white clouding of the cornea with photophobia, lacrimation and blepharospasm), labyrinthine deafness (inflammatory phenomena and hemorrhages in the inner ear in combination with dystrophy of the auditory nerve) ••• Relative signs are assessed in conjunction with other manifestations. These include: syphilitic chorioretinitis (characteristic of the “salt and pepper” pattern on the fundus), saber-shaped shins (the result of diffuse osteoperiostitis with reactive osteosclerosis and anterior curvature of the bones of the legs), Robinson-Fournier scars (in the circumference of the mouth after Hochsinger infiltrations), syphilitic gonitis , occurring as chronic allergic synovitis (distinguished by the absence of sharp pain, fever and dysfunction of the joint), buttock-shaped skull (sharply protruding frontal tubercles with a groove located between them), nasal deformities (saddle-shaped, lorgnette-shaped, etc.), dental dystrophy (tooth Muna - underdevelopment of the chewing tubercles of the first molars, Fournier's pike tooth - a change in the canine with thinning of its free end) ••• Dystrophies with congenital syphilis: Ausitidian sign (thickening of the sternal end of the clavicle), Olympic forehead (increase in the frontal and parietal tubercles), high (Gothic ) palate, infantile (shortened) little finger of Dubois-Hissar, absence of the xiphoid process of the sternum, widely spaced upper incisors, etc. Only the presence of several dystrophies in combination with other signs of syphilis and anamnesis data can, in unclear cases, help make a diagnosis of congenital syphilis.
Research methods • In the primary period: detection of pale treponema in the discharge from chancre • Serological reactions •• RSC (type of von Wasserman reaction) with cardiolipin and treponemal Ag and microprecipitation reaction with cardiolipin Ag (VDRL - with inactivated blood serum, RPR - with plasma blood, UJR - with active blood serum; ART - automated reagin test, etc.). Positive results are expressed by pluses (from + to ++++). In case of a sharply positive reaction, a study is carried out with various dilutions of serum (from 1:10 to 1:320). Reactions are positive from the middle of the primary period and during the secondary period; in the tertiary period they can be negative in 50% of patients •• Treponema pallidum immobilization test: carried out for false-positive serological reactions, assessed as negative when less than 20% of Treponema pallidum are immobilized, weakly positive - 21– 50%, positive - over 50% •• RIF: becomes positive in the majority of patients with syphilis already in the primary seronegative period; the results are assessed as positive (from + to ++++); positive in all periods of syphilis (including late forms) in almost all patients •• ELISA •• Passive hemagglutination test
TREATMENT • Specific treatment is prescribed after clinical and laboratory confirmation of the diagnosis (exception: preventive treatment of persons who have had sexual and close household contact with patients with early forms of syphilis, if no more than 2 months have passed since the contact) • Preventive treatment is carried out for women who received treatment before pregnancy , in whom by the beginning of pregnancy there was no complete negativity of the CSR (a complex of serological reactions, including various methods for detecting antibodies to the pathogen, for example, the von Wasserman reaction, microprecipitation reactions, less often others), as well as all women who began treatment during pregnancy, regardless of its term. And also to children born without manifestations of syphilis from an untreated mother; with late specific treatment for the mother (from 32 weeks of pregnancy); in the absence of negativity of CSR at the time of birth or seroresistance in the mother.
Drug therapy • Causal therapy: benzylpenicillin preparations are the mainstay in the treatment of all forms of syphilis. In case of intolerance: penicillin drugs, alternative drugs specified in the guidelines are prescribed (erythromycin, tetracycline, oleandomycin + tetracycline, doxycycline, cefazolin, etc.).
Treatment of primary syphilis: method No. 1 - two injections of benzathine benzylpenicillin at a dose of 2.4 million units with an interval of 7 days, or three injections of benzathine benzylpenicillin at a dose of 2.4 million units once every 5 days; Method No. 2 - benzathine benzylpenicillin + benzylpenicillin procaine + benzylpenicillin at a dose of 1.8 million units 2 times a week, a total of 5 injections, or benzathine benzylpenicillin + benzylpenicillin procaine at a dose of 1.5 million units 2 times a week, a total of 5 injections; Method No. 3 - penicillin procaine at a dose of 1.2 million units daily for 10 days or 600,000 units 2 times a day for 10 days; Method No. 4 - water-soluble penicillin intramuscularly every 6 hours for 10 days.
Treatment of secondary and early latent syphilis: method No. 1 - three injections of benzathine benzylpenicillin at a dose of 2.4 million units with an interval of 7 days, or six injections of benzathine benzylpenicillin at a dose of 2.4 million units once every 5 days; Method No. 2 - benzathine benzylpenicillin + benzylpenicillin procaine + benzylpenicillin at a dose of 1.8 million units 2 times a week, a total of 10 injections, or benzathine benzylpenicillin + benzylpenicillin procaine at a dose of 1.5 million units 2 times a week, a total of 10 injections; Method No. 3 - penicillin procaine at a dose of 1.2 million units daily for 20 days or 600,000 units 2 times a day for 20 days; Method No. 4 - water-soluble penicillin intramuscularly every 6 hours for 20 days.
Treatment of other forms of syphilis - see Methodological recommendations “Treatment and prevention of syphilis”, approved by the Ministry of Health of the Russian Federation (1999).
Contraindications. Tetracyclines - during pregnancy and children under 8 years of age.
Clinical and serological control after the end of treatment • After preventive treatment, once 3 months after treatment • For primary seronegative syphilis - 3 months • Patients with early forms of syphilis who had positive DSR results before treatment are subject to clinical and serological control until the DSR is completely negative and then another 6 months • For late forms, latent, visceral and neurosyphilis - 3 years.
Prevention • Public: free treatment, active detection, examination and involvement of contact persons in treatment, screening for syphilis of donors, pregnant women, all inpatients, workers of food enterprises and child care institutions • Individual: use of condoms.
ICD-10 • A50 Congenital syphilis • A51 Early syphilis • A52 Late syphilis • A53 Other and unspecified forms of syphilis
Primary syphilis
After the end of the incubation period, the characteristic first symptoms of syphilis appear. At the site of penetration of the treponemas, a hard chancre is formed, a specific round erosion or ulcer, with a hard, smooth bottom and “turned-up” edges. The size of the formations can vary from a couple of mm to several centimeters. Hard chancre can disappear without treatment. Erosions heal without a trace, ulcers leave flat scars.
The disappearance of chancre does not mean the end of the disease: primary syphilis only passes into a latent form, during which the patient is still infectious to sexual partners.
After the formation of hard chancre, local enlargement of the lymph nodes begins after 1-2 weeks. When palpated, they are dense, painless, and mobile; one is always larger than the others. After another 2 weeks, the serum (serological) reaction to syphilis becomes positive, from this moment primary syphilis passes from the seronegative stage to the seropositive stage. The end of the primary period: body temperature may rise to 37.8 - 380, sleep disturbances, muscle and headaches, and joint aches appear. Dense swelling of the labia (in women), the head of the penis and the scrotum in men is possible.
Chancre
It is formed, as a rule, at the site of penetration of Treponema pallidum (with genital contact - in the genital area, with oral-genital contact - in the oral cavity, in the lip area, etc.).
The formation of chancre occurs in several stages:
- formation of a small spot, pink-red color;
- formation of an erosive defect;
- compaction of the erosion bottom, color change to bright red. The erosion is covered with a transparent or brown film.
With timely treatment or, on the contrary, transition to the next stage of syphilis, the chancre again enters the spot stage and then completely disappears. As a rule, such a tumor does not cause discomfort in an infected person. Slight itching may occur in the area of erosion.
You might be interested! The first signs and causes of the development of Quincke's edema in children
Chancre is classified according to the following criteria:
- by quantity (single, multiple);
- according to the depth of the skin lesion (erosive - affects only the superficial layers, ulcerative - the lesion affects the deep layers of the skin);
- by size (dwarf - less than 10 mm, medium - 10-20 mm, giant - more than 40 mm).
There are also atypical forms of chancre, which are extremely rare.
These include:
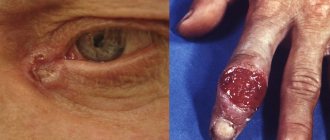
- chancre-amygdalid : a hard chancre located on the tonsil (in the ulcerative form of this process, a single tonsil is affected, it becomes compacted and a bright red ulceration with smooth edges is formed on the surface; in the angina-like form, a tissue defect does not form, the tonsil is dense, painless, pale treponema are found on its surface);
- chancre-felon (the clinical picture is similar to streptococcal felon, however, with a syphilitic nature, acute inflammation does not develop);
- indurative edema manifests itself in the genital area in the form of sharp swelling and changes in tissue turgor.
As a rule, diagnosing a typical chancre does not cause much difficulty. Its distinctive feature is the enlargement of regional lymph nodes, which remain dense and painless throughout the course of the primary stage.
Complications of chancroid:
- balanitis;
- balanoposthitis;
- phimosis;
- paraphimosis;
- phagedenism;
- gangrene.
Photo
The photograph shows the typical shape of chancre. There is a clear demarcation of this formation from healthy skin, a hyperemic surface of erosion, covered with a thin transparent film.
Secondary syphilis
The infection generalizes by 3 months from the moment of infection and lasts 3-5 years, this period is characterized by multiple different-looking rashes in various organs and tissues, and therefore absolutely any symptoms depending on which system/organ is affected more and how much it is affected was previously compromised, that is, was he healthy at the time of the defeat - if so, then the manifestations of syphilis will be minimal.
During this period, there are prodromal symptoms (as with colds - general malaise, pain in muscles, joints, the appearance of fever), they last 7-10 days until the appearance of syphilomas (roseolous-papular rashes) - often these are small red spots with clear boundaries , not merging with each other. When pressed, they disappear, and then appear, or may turn yellow due to the destruction of red blood cells. These rashes do not destroy tissue and, with antisyphilitic treatment, disappear instantly. These rashes are recurrent in nature, that is, they appear again, but are not as pronounced and in much smaller quantities.
Papular syphilide
Papular syphilide is a dermal papule that is formed as a result of an accumulation of cells (cellular infiltrate) located under the epidermis in the upper dermis. The elements of the rash have a round shape, are always clearly demarcated from the surrounding tissues, and have a dense consistency. Their main locations are the trunk, limbs, face, scalp, palms and soles, oral mucosa and genitals.
- The surface of the papules is smooth, shiny, and smooth.
- The color is pale pink, copper or bluish red.
- The shape of the papules is hemispherical, sometimes pointed.
- They are located in isolation. Papules located in skin folds tend to grow peripherally and often merge. Vegetation and hypertrophy of papules leads to the formation of condylomas lata.
- With peripheral growth, the resorption of papules begins from the center, resulting in the formation of various figures.
- Papules located in the folds of the skin sometimes erode and ulcerate.
- Depending on the size, miliary, lenticular and coin-shaped papules are distinguished.
Papular syphilides are extremely contagious, as they contain a huge number of pathogens. Particularly contagious are patients whose papules are located in the mouth, perineum and genitals. Handshakes, kisses and close contact can cause transmission of infection.
Papular syphilides resolve within 1 to 3 months. When the papules dissolve, peeling is observed. Initially, it appears in the center, then, like a “Biette collar,” on the periphery. In place of the papules, a pigmented brown spot remains.
Papular syphilide is more typical for recurrent secondary syphilis.
Rice. 5. Rash due to secondary syphilis - papular syphilide.
Miliary papular syphilide
Miliary papular syphilide is characterized by the appearance of small dermal papules - 1 - 2 mm in diameter. Such papules are located at the mouths of the follicles; they are round or cone-shaped, dense, covered with scales, sometimes with horny spines. The trunk and limbs are their main places of localization. Resolution of papules occurs slowly. A scar remains in their place.
Miliary papular syphilide should be distinguished from lichen scrofulous and trichophytosis.
Miliary syphilide is a rare manifestation of secondary syphilis.
Lenticular papular syphilide
Lenticular papules form in the 2nd to 3rd year of the disease. This is the most common type of papular syphilis, occurring in both early and late secondary syphilis.
The size of the papules is 0.3 - 0.5 cm in diameter, they are smooth and shiny, round in shape with a truncated apex, have clear contours, pink-red color, and are painful when pressed with a button probe. As the papules develop, they become yellowish-brown in color, flatten, and become covered with transparent scales. A marginal appearance of peeling (“Biette’s collar”) is characteristic.
During early syphilis, lenticular papules can appear on different parts of the body, but most often they appear on the face, palms and soles. During the period of recurrent syphilis, the number of papules is smaller, they tend to group, and bizarre patterns are formed - garlands, rings and arcs.
Lenticular papular syphilide should be distinguished from guttate parapsoriasis, lichen planus, vulgar psoriasis, and papulonecrotic tuberculosis of the skin.
On the palms and soles, papules are reddish in color with a pronounced cyanotic tint, without clear boundaries. Over time, the papules acquire a yellowish color and begin to peel off. A marginal appearance of peeling (“Biette’s collar”) is characteristic.
Sometimes the papules take on the appearance of calluses (horny papules).
Palmar and plantar syphilides should be distinguished from eczema, athlete's foot and psoriasis.
Lenticular papular syphilide occurs in both early and late secondary syphilis.
Rice. 6. Lenticular papules in secondary syphilis.
Rice. 7. Palmar syphilide with secondary syphilis.
Rice. 8. Plantar syphilide with secondary syphilis
Rice. 9. Secondary syphilis. Papules on the scalp.
Coin-shaped papular syphilide
Coin-shaped papules appear in patients during the period of recurrent syphilis, in small quantities, bluish-red in color, have a hemispherical shape, measuring 2 - 2.5 cm in diameter, but can be larger. When resorption occurs, pigmentation or an atrophic scar remains in place of the papules. Sometimes there are many small ones around the coin-shaped papule (bursant syphilide). Sometimes the papule is located inside a ring-shaped infiltrate; between it and the infiltrate there remains a strip of normal skin (a type of cockade). When coin-shaped papules coalesce, plaque syphilide is formed.
Rice. 10. A sign of syphilis of the secondary period is psoriasiform syphilide (photo on the left) and nummular (coin-shaped) syphilide (photo on the right).
Wide type of papular syphilide
The broad type of papular syphilide is characterized by the appearance of large papules. Their size sometimes reaches 6 cm. They are sharply demarcated from healthy areas of the skin, covered with a thick stratum corneum, and dotted with cracks. They are a sign of recurrent syphilis.
Seborrheic papular syphilide
Seborrheic papular syphilide often appears in places with increased sebum secretion - on the forehead (“the crown of Venus”). On the surface of the papules there are fatty scales.
Rice. 11. Seborrheic papules on the forehead.
Weeping papular syphilide
Weeping syphilide appears in areas of the skin where there is increased humidity and sweating - the anus, interdigital spaces, genitals, large folds of skin. Papules in these places undergo maceration, become wet, and acquire a whitish color. They are the most contagious form among all secondary syphilides.
Weeping syphilide must be distinguished from folliculitis, contagious molluscum, hemorrhoids, chancroid, pemphigus and epidermophytosis.
Rice. 12. Secondary syphilis. Weeping and erosive papules, condylomas lata.
Erosive and ulcerative papules
Erosive papules develop in the event of prolonged irritation of their localization sites. When a secondary infection occurs, ulcerative papules are formed. The perineum and anal area are common places for their localization.
Condylomas lata
Papules that are subject to constant friction and weeping (anal area, perineum, genitals, inguinal, less often axillary folds) sometimes hypertrophy (increase in size), vegetate (grow) and turn into condylomas lata. Vaginal discharge contributes to the appearance of condylomas.
Rice. 13. When papules grow, condylomas lata are formed.
Tertiary syphilis
Tertiary syphilis is characterized by a long latent course. It can appear after 3-4 years (with complete absence of treatment, or with insufficient treatment). Most often, this form of pathology can be found in patients suffering from chronic alcoholism, tuberculosis or other infections.
During this period, a small amount of dense infiltrates, localized in the subcutaneous tissue or in deeper tissues, is found on the patient’s skin and mucous membranes. After some time, they disintegrate, and in their place painless ulcers appear, which scar only after a few months or years. It should be noted that such syphilides are not accompanied by subjective disorders and do not disturb the general condition of the patient. They contain very little pathogen, and therefore are practically non-contagious.
Third stage of the disease
Nowadays, stage three syphilis is not often encountered. This is very good news not only for doctors, but also for the patients themselves. Due to the fact that the infection is diagnosed in time, doctors prescribe the optimal treatment, which allows stopping the disease in the initial stages. If the disease is not treated, it may not make itself felt for the first couple of years, slowly affecting the body from the inside.
In no more than five years, syphilis will slowly but surely enter its third stage. During this period, internal organs and the endocrine system are seriously damaged. The disease greatly affects the senses. Even at this stage, the patients' bodies are covered with small tubercles called syphilides. When they are opened, pus is released. Sometimes syphilides appear only on the body, but with advanced disease they can form on internal organs, which in turn is fatal.
Cartilage and other soft tissues will undergo severe deformation. They can degenerate into tumors, which are called gummas.
Syphilis is not only a serious, but also a very dangerous disease. The danger lies in the fact that for many years it may not manifest itself, proceeding exclusively in a latent form. Sometimes external signs appear only at the third stage. To protect yourself from troubles and identify the infection at the earliest stages, you need to undergo a routine examination with a doctor.
Congenital syphilis
It is transmitted from a sick mother when treponemes penetrate the placenta into the fetus. Syphilis infection can occur both during conception and much later. Regardless of the time of infection, pathological tissue changes are observed only in the VI-VII months of pregnancy, so active prevention of syphilis in the early stages will help give birth to a healthy child.
The possibility of transmitting pathogens through the father's sperm has not yet been proven, so all preventive measures usually concern the expectant mother. These include: identification of sick women in the early stages, full registration of pregnant women, monitoring the treatment of infected persons. In order to prevent the development of negative changes, mandatory regular examinations of pregnant women are carried out for the presence of treponemas and external signs of congenital syphilis.
Complications associated with syphilis
Pregnant mothers and newborns
Mothers infected with syphilis are at risk of miscarriage and premature birth. There is also a risk that a mother with syphilis will pass the disease to her fetus. This type of disease is known as congenital syphilis (discussed above).
Congenital syphilis can be life-threatening. Babies born with congenital syphilis may also have the following conditions:
- external deformity;
- developmental delays;
- seizures;
- rashes;
- fever;
- inflammation of the liver or spleen;
- anemia;
- jaundice;
- infectious diseases.
If a child has congenital syphilis and it is not detected, the child may develop late stage syphilis. This can lead to problems with:
- skeleton;
- teeth;
- eyes;
- ears;
- brain.
Neurological problems
Syphilis can cause a number of problems with your nervous system, including:
- stroke;
- meningitis;
- hearing loss;
- loss of pain and temperature sensations;
- sexual dysfunction in men (impotence);
- urinary incontinence in women and men;
- sudden, lightning pain.
Cardiovascular problems
These can include an aneurysm and inflammation of the aorta—your body's main artery—and other blood vessels. Syphilis can also damage the heart valves.
HIV infection
People with syphilis are much more likely to become infected with HIV. Ulcers on the patient’s body facilitate the penetration of the human immunodeficiency virus (HIV) into the body.
It is also important to note that people with HIV may experience different symptoms of syphilis.
Features of syphilis symptoms in men and women
The secondary and tertiary periods have almost the same symptoms. Differences in symptoms for men and women are present only in the primary period, when chancre appears on the genitals:
- gangrenous chancre on the penis - there is a possibility of self-amputation of the distal part of the penis;
- chancre on the cervix. Signs of syphilis, when hard chancre is located on the uterus in women, are practically absent and can only be detected during a gynecological examination;
- chancre in the urethra is the first sign of syphilis in males, which is manifested by discharge from the urethra, a dense penis and an inguinal bubo.
Manifestations of the disease in both sexes
In men, syphilis most often affects the penis and scrotum - it is on the external genitalia that the disease primarily manifests itself in the form of negative symptoms.
In women , the disease most often affects the labia minora, vagina and mucous membranes. If sexual partners practice oral or anal sex, infection and subsequent damage to the circumference of the anus, oral cavity, mucous membrane of the throat and skin in the chest and neck area occurs.
The course of the disease is long-term, if it is not treated in a timely manner, it is characterized by a wave-like manifestation of negative symptoms, a change in both the active form of the pathology and the latent course.
Diagnostics
Syphilis is diagnosed by examination, characteristic signs and laboratory tests:
- Examination by a dermatovenerologist. He asks the patient in detail about the course of the disease, examines the skin, genitals, and lymph nodes.
- Detection of treponema or its DNA in the contents of gummas, chancre, syphilides using dark-field microscopy, direct immunofluorescence reaction, and PCR.
- Instrumental studies: search for gummas using ultrasound, MRI, CT, X-rays, etc.
- Carrying out various serological tests: Non-treponemal - search for antibodies against treponema membrane lipids and phospholipids of tissues destroyed by the pathogen (Wassermann reaction, VDRL, rapid plasma reagin test). The result obtained may be false positive, i.e. show syphilis where there is none. Treponema - search for antibodies to Treponema pallidum (RIF, RPHA, ELISA, immunoblotting, RIBT).
Remember that for such a serious disease you cannot diagnose yourself “on the Internet” by reading about syphilis and its symptoms. The fact is that the rash and other changes can visually copy those of completely different diseases, so that even doctors are periodically misled.
The difference between acne due to syphilis and chickenpox
Smallpox syphilide is most easily confused with chickenpox.
This disease is diagnosed mainly in childhood.
In adults it is more severe.
The difference is a pronounced intoxication syndrome.
It occurs 2-3 days before acne appears.
Severe hyperthermia, cephalalgia, myasthenia gravis, and sore throat are noted.
There are many foci of rashes, and they are located in groups.
While with syphilis there are few of them, and they are single.
Another feature of chickenpox is the extremely rapid transformation of morphological elements.
The entire cycle can take only 8 hours.
First, pink spots form.
From them papules are formed.
They turn into bubbles.
They usually contain completely clear liquid.
Unlike syphilis, in which the contents of the vesicles are often purulent.
With chickenpox, there is severe itching of the skin.
Consequences of syphilis
If left untreated, syphilis gradually spreads throughout the body and affects more and more healthy tissues and organs. Sometimes there is temporary relief, after which the patient’s condition sharply worsens. Complications of syphilis depend on its stage.
Primary syphilis can be complicated by the following conditions:
- tissue necrosis at the location of the chancre;
- balanitis;
- phimosis;
- paraphimosis
With secondary syphilis, the following complications are noted:
- damage to internal organs by syphilis;
- damage to the nervous system;
- bone damage.
Complications of tertiary syphilis are:
- damage to internal organs;
- brain damage;
- Treponema damage to the tissues of the neck and face;
- pathological fractures of bones when they are affected by syphilis;
- bleeding as a result of vascular rupture.
Pustular syphilide
Pustular syphilide, like vesicular syphilide, is rare, usually in weakened patients with low immunity and has a malignant course. When the disease occurs, the general condition of the patient suffers. Symptoms such as fever, headache, severe weakness, joint and muscle pain appear. Often, classical tests for syphilis give negative results.
Acne, smallpox, impetiginous, syphilitic ecthyma and rupiah are the main types of pustular syphilide. Rashes of this type are similar to dermatoses. Their distinctive feature is a copper-red infiltrate located along the periphery in the form of a roller. The occurrence of pustular syphilide is promoted by diseases such as alcoholism, toxic and drug addiction, tuberculosis, malaria, hypovitaminosis, and trauma.
Acne-like (acneiform) syphilide
The rashes are small pustules of a rounded conical shape with a dense base, located at the mouths of the follicles. After drying, a crust forms on the surface of the pustules, which falls off after a few days. A depressed scar remains in its place. The scalp, neck, forehead, and upper half of the body are the main locations for acne syphilide. Elements of the rash appear in large numbers during the period of early secondary syphilis, and scanty rashes appear during the period of recurrent syphilis. The general condition of the patient suffers little.
Acne syphilide should be distinguished from acne and papulonecrotic tuberculosis.
Rice. 14. Rash due to syphilis - acne syphilide.
Smallpox syphilide
Smallpox syphilide usually occurs in weakened patients. Pea-sized pustules are located on a dense base, surrounded by a copper-red ridge. When the pustule dries out it becomes like a smallpox element. In place of the fallen crust, brown pigmentation or an atrophic scar remains. The rashes are not abundant. Their number does not exceed 20.
Rice. 15. The photo shows manifestations of secondary syphilis - smallpox syphilide.
Impetiginous syphilide
With impetiginous syphilide, a dark red papule the size of a pea or more appears first. After a few days, the papule festeres and shrinks into a crust. However, the discharge from the pustule continues to be released to the surface and dries out again, forming a new crust. The layering can become large. The formed elements rise above the skin level. When syphilides merge, large plaques are formed. After peeling off the crusts, a juicy red bottom is exposed. Vegetative growths resemble raspberries.
Impetiginous syphilide, located on the scalp, nasolabial fold, beard and pubis, is similar to a fungal infection - deep trichophytosis. In some cases, the ulcers merge, forming large areas of damage (corrosive syphilide).
Healing of syphilide is long. Pigmentation remains at the site of the lesion, which disappears over time.
Impetiginous syphilide should be distinguished from impetiginous pyoderma.
Rice. 16. In the photo, a type of pustular syphilide is impetiginous syphilide.
Syphilitic ecthyma
Syphilitic ecthyma is a severe form of pustular syphilide. Appears 5 months after infection, earlier in weakened patients. Deep pustules are covered with thick crusts up to 3 or more centimeters in diameter; they are thick, dense, and layered. Elements of the rash rise above the surface of the skin. They have a round shape, sometimes irregular oval. After the crusts are rejected, ulcers with dense edges and a bluish rim are exposed. The number of ecthymas is small (no more than five). The main places of localization are the limbs (usually the lower legs). Healing occurs slowly, over 2 or more weeks. Ecthymas can be superficial or deep. Serological tests sometimes give negative results. Syphilitic ecthyma should be distinguished from vulgar ecthyma.
Rice. 17. Secondary syphilis. A type of pustular syphilide is syphilitic ecthyma.
Syphilitic rupee
A type of ecthyma is syphilitic rupee. The rashes range in size from 3 to 5 centimeters in diameter. They are deep ulcers with steep, infiltrated edges, covered with dirty and bloody discharge, which dry to form a cone-shaped crust. The scar heals slowly. It is often located on the shins. It spreads both peripherally and deeply. Combines with other syphilides. It should be distinguished from rupoid pyoderma.
Rice. 18. Rash due to secondary syphilis - syphilitic rupee.
Rice. 19. In the photo, the symptoms of malignant syphilis of the secondary period are deep skin lesions: multiple papules, syphilitic ecthymas and rupees.
How to treat syphilis?
The treatment of syphilis is approached in a comprehensive manner, taking into account many individual factors (age, gender of the patient, stage of development of the disease, the presence of concomitant diseases, general condition of the body, etc.). In addition, all sexual partners of the suspected patient should also be examined for the presence of syphilis and, if necessary, undergo a course of therapy.
If a patient has primary syphilis, then everyone who has had sexual intercourse with him over the past three months must undergo examination and tests. In the case of secondary syphilis - everyone who had contact with the patient over the past year. The timeliness of the therapy itself, as well as the correct selection of modern medications, is important for achieving success in the treatment of this disease.
The most effective method of treating syphilis is the introduction of water-soluble penicillins into the body. This therapy is carried out in a hospital setting for 24 days with injections every 3 hours. The causative agent of syphilis is quite sensitive to penicillin antibiotics, but there is a possibility of an allergic reaction to these drugs or the ineffectiveness of such therapy. In this case, penicillin is replaced with drugs of the tetracycline, macrolide, and fluoroquinolone groups. In addition to antibiotics, natural immune stimulants, vitamins, and immunostimulants are also indicated for syphilis.
Follow-up
After you are treated for syphilis, your doctor will ask you to:
- periodically take blood tests to ensure that the body responds positively to the usual dosage of penicillin;
- avoid sexual contact until treatment is completed and blood tests show that the infection has been completely cured;
- inform your partners about the disease so that they also undergo diagnosis and, if necessary, treatment;
- be tested for HIV infection.
Prevention
Standard preventive measures include avoiding casual sex, using condoms, and to prevent occupational syphilis, wearing disposable latex gloves before examination, manipulation and surgery.
Condoms are not 100% protection - the chancre can be located extragenitally (pubis, perineum), and with secondary syphilis, a “necklace of Venus” is formed on the skin. In these cases, the infection from syphilis is transmitted by contact to the partner’s skin.
With syphilis, lifelong immunity is not formed. Having successfully recovered from this disease, you can become infected and get sick again. In this case, the disease will be just as severe. Therefore, there are no vaccinations against syphilis, and there cannot be.
Necklace of Venus (syphilitic leucoderma)
It is a specific sign of syphilis. It forms in the neck area and appears as light, round lesions on the skin that look like a necklace.
Photo
The photograph shows a large number of light spots on the brown surface of the patient's skin, forming a characteristic Venus necklace .
Photo
The photograph shows a patient with a roseola rash , a characteristic manifestation of secondary syphilis.
Forecast
It all depends on the stage of development of the disease and the treatment method. If therapy was started in the early stages of the disease (primary, secondary and early latent syphilis) and is carried out using treponemocidal antibiotics, then in almost all cases without exception, a complete clinical cure occurs, and relapses of early syphilis and the occurrence of late forms of syphilis are prevented.
Treatment of syphilis in pregnant women in the first half of pregnancy in most cases guarantees the birth of a healthy baby. In the case of congenital syphilis, the prognosis is favorable if treatment of the disease was started in a timely manner. Treatment of later forms of the disease is less successful, since it only slows down the progression of the disease, but in all cases it can restore the impaired function of the affected organs and lead to negative serological reactions.
Basic terminology
Tripper, Lewis or syphilis are all names for the same disease, caused by the bacterium Treponema pallidum. This microorganism does not care whose body it infects. At the same time, syphilis occurs more often in women than in children and men. The following photos will help you understand all the main features of this insidious and extremely dangerous disease.