The word “leprosy” is familiar to many people - it is the name of a group on many social networks, in which a kind of cynical humor reigns on a variety of topics. In medical circles, the Greek term "lepra" is translated as "leprosy" and means Hansen's disease. What kind of illness is this? How dangerous is he?
Leprosy is a chronic infectious disease caused by the bacteria Mycobacterium leprae. First of all, bacilli affect the skin, peripheral nervous system, respiratory and visual organs.
In the old days, people with leprosy were called lepers and were almost always sent into exile (by decision of the community through a popular vote of shards - ostracism). Even the most experienced healers of Ancient Egypt, China, and India considered it incurable. For this reason, lepra has received many names: the mournful or Phoenician disease, the lazy death, the disease of St. Lazarus.
The modern name for leprosy is hansenosis, hanseniasis (from the name of the Norwegian scientist Gerhard Hansen, who discovered the leprosy bacterium in 1873).
The pathogen is an acid-resistant rod with pointed ends, which is capable of forming a granular form and an A-form. This mycobacterium multiplies slowly and over time forms a whole family in the body that resembles a cluster of balls.
Remember: infection occurs through the respiratory tract.
Please note:
- a person can become infected only after close, prolonged contact with a sick person;
- Children are more susceptible to leprosy than adults.
According to statistics, more than 180 thousand people suffer from hansenosis worldwide, most of whom live in Asia, Africa, and the USA. Treatment of sick people takes place in special leper colonies, which protect others from carriers of the disease.
According to the World Health Organization, countries such as Bangladesh, Norway, Angola, Sudan, Ethiopia, Tanzania, Sri Lanka, Nepal, Brazil, the Philippines, Madagascar, the Republic of the Congo, Myanmar, Nigeria, remain areas of high endemicity. Mozambique.
What do we know about leprosy
In the 21st century, leprosy is officially classified as a “neglected disease.” The term can be misleading: in fact, only residents of economically developed countries have managed to forget about many diseases of this group. WHO estimates that about 1.7 billion people annually need prevention and treatment for at least one of these diseases. In 2019, more than 200,000 new cases of Hansen's disease were reported worldwide. In Russia, only a few receive a diagnosis - for example, in 2020, doctors identified six cases of the disease, and in total about two hundred people are registered.
About the history of leprosy in Russia
The limit of grief: how leprosy spread across Russia and why it cannot be called leprosy
The disease can affect the skin, eyes, peripheral nerves, and the mucous membrane of the upper respiratory tract. One of the mysteries of leprosy is its long incubation period. On average, symptoms appear three to five years after infection, but in some cases the disease “sleeps” in the body for decades. It is difficult to become infected with leprosy; this is only possible through long-term household contact with a sick person. Immunity also plays a role: if it is weakened by other diseases or difficult living conditions, the risk increases.
Today, leprosy is curable; the first effective drug was developed back in the 1940s. Today, doctors use a combination of several medications; with their help, a disease detected in time can be overcome in an average of five years, most often it can be overcome in a year.
The disease has many informal names, but the most commonly used term is “Hansen's disease” - in honor of the scientist who managed to discover the bacterium that causes the disease. Activists are calling for the use of this name or the neutral term “leprosy.” The words “leprosy” and “lepers” have developed negative connotations over the centuries, associated with disgust and lifelong exile from society. The use of these terms perpetuates the stigma against patients, which is still strong today, including in Russia. Nevertheless, in the article we will resort to the terms “leprosy” and “lepers” when talking about data from historical sources of the Middle Ages.
Causes of leprosy
The cause of leprosy is Mycobacterium leprae, which was discovered by the Norwegian physician Hansen in 1874. Therefore, another name for leprosy is Hansen's disease. The pathogen looks like a straight or slightly curved stick with rounded ends. The length of the mycobacterium is 1.0 - 7.0 microns, and the diameter is from 0.2 to 0.5 microns. It is resistant to acids and alcohol and is an obligate intracellular parasite, invading tissue macrophages.
The main source of leprosy infection is a sick person who releases mycobacterium leprosy into the environment through saliva, nasal mucus, breast milk, semen, urine, feces and wound discharge. The causative agent of leprosy penetrates the skin and mucous membranes, from there into the nerve endings, lymphatic and blood vessels. With the flow of blood and lymph, they spread throughout the body and affect the internal organs.
A healthy person is practically not susceptible to leprosy. The risk group for infection includes children, alcoholics, drug addicts and people with chronic diseases, especially those with weakened immune systems.
Leprosy in the Middle Ages
For a long time it was believed that the disease came to Europe after the First Crusade (1096–1099). This opinion arose during the Enlightenment. Scientists spared no expense in depicting the atrocities of the Crusaders in the Holy Land, and perceived the disease as fair retribution for violence. However, already in the 19th century it became clear that even before the Crusades, there were many cases of leprosy in European countries and there were even organized “homes” for the sick. Both written sources and excavation data speak about this.
Nevertheless, it was in the 12th century that the number of leper colonies and their inhabitants sharply increased in Europe. For example, at the beginning of the century, French documents mention five institutions, and in the 1130s there were already 18. By the end of the century, Toulouse alone had eight “asylums” for leprosy patients. Modern scientists believe that the matter is not only and not so much about the Crusades. In the 11th century, cities began to grow in Europe. Agriculture and crafts improved, the population grew, and some people left villages and villages for large fortified settlements. At the same time, many new trade connections are emerging. In such conditions, diseases spread much more easily than in the divided Europe of the early Middle Ages.
In the Middle Ages, leprosy was considered incurable - given the level of development of medicine, it was so. Nevertheless, the sick still had hope: what if the suspicious illness turned out to be some other disease?
Medieval diagnostics were much less accurate than modern ones, so this happened from time to time. The inability to be cured eventually became one of the main medieval “diagnostic criteria” for leprosy. Only after trying all the available methods could one be convinced that the disease really could not be healed, which means that the patient was doomed to slowly fade away.
They knew about the contagiousness of the disease in the Middle Ages. It was believed that the disease was transmitted through breathing - doctors and priests examining the sick were recommended to cover their faces. Doctors did not consider the touch of a sick person dangerous, unlike the authorities of some cities: they ordered people with suspected leprosy to wear gloves. Sexual transmission of the disease was considered rare, although in modern times such a stereotype will indeed appear.
At the same time, the “repulsive” appearance of the patients apparently worried Europeans more than the possibility of infection. For example, in Gar's poem the focus is on the disfigured appearance of the leper youth, rather than on the fears of those around him. And in the ancient Russian story from the Kiev-Pechersk Patericon, people began to avoid the sick city dweller only at the moment when a stench began to emanate from his body.
WHO activities
In 2021, to accelerate efforts to control leprosy, WHO launched the Global Leprosy Strategy 2016–2020: Accelerating Action to Eliminate Leprosy in the World. The main focus of this Strategy is on children, as well as on the prevention of disability.
- Global Leprosy Strategy 2016–2020: Accelerating Action to Eliminate Leprosy in the World - in English
Based on the “Global Leprosy Strategy 2016–2020.” There are three main components:
Component I: Strengthen government ownership, coordination and partnerships
Main events
- Provide political commitment and adequate resources for leprosy control programs.
- Promote universal health coverage, with special attention to children, women and disadvantaged groups, including migrants and displaced people.
- Strengthen partnerships with government and non-government actors and promote cross-sectoral collaboration and partnerships internationally and within countries.
- Promote and conduct basic and operational research on all aspects of leprosy and maximize the evidence base for the development of policies, strategies and interventions.
- Strengthen surveillance and health information systems for program monitoring and evaluation (including geographic information systems).
Component II: Stop leprosy and its complications
Main events
- Raise awareness among patients and communities regarding leprosy.
- Promote early case detection through active searches (e.g. campaigns) in areas of high endemicity and follow-up of contacts.
- Ensure prompt treatment initiation and adherence, including work to improve treatment regimens.
- Improve prevention and management of disability.
- Strengthen antimicrobial resistance surveillance, including laboratory network.
- Promote innovative approaches to specific training, referral and professional development in leprosy, such as e-health.
- Promote activities to prevent infections and diseases.
Component III: End discrimination and promote social inclusion
Main events
- Promote social inclusion by taking action against all forms of discrimination and stigma.
- Empower people affected by leprosy and strengthen their capacity to actively participate in leprosy services.
- Engage communities to improve leprosy services.
- Promote the creation of coalitions among people affected by leprosy, and facilitate the association of these coalitions and/or their members with other community-based organizations.
- Promote access to social and financial support services, such as income generation support, for people affected by leprosy and their families.
- Support community-based rehabilitation of people with leprosy-related disabilities.
- Work to repeal discriminatory laws and promote policies for the social inclusion of people affected by leprosy.
Goals of the Global Leprosy Strategy
- there are no disabled people among the new child patients;
- disability of the second group occurs in less than one in a million people;
- No country has legislation allowing discrimination on the basis of leprosy.
In August 2021, WHO published Operational Guidance to support the adaptation and implementation of the Global Leprosy Strategy 2016–2020. This guidance provides guidance to managers of national leprosy programs (or equivalent) on how to adapt and implement the Global Leprosy Strategy to the epidemiological burden in their countries.
- Operational guidance 2021 – Global Leprosy Strategy 2016–2020. - in English
In March 2021, the WHO Global Leprosy Program published “Guidelines for monitoring and evaluating the implementation of the Global Leprosy Strategy.” The Global Leprosy Program is leading efforts to expand the drug-resistant leprosy surveillance network, which is a key activity of the Global Leprosy Strategy. Guidance on surveillance of antimicrobial resistance in leprosy has also been published.
How was the disease identified?
The “diagnosis” was not always made by doctors. At first, this was done by the clergy: most often the sick person was examined by the parish priest. In the middle of the 13th century, the situation changed; by that time, professional doctors and surgeons appeared in Europe. The first were relatively highly educated, knew medical theory and were engaged not only in the treatment of diseases, but also in prevention - for example, they developed an individual diet for the patient. The latter were responsible for performing “dirty” tasks that required direct surgical intervention in the patient’s body. Of course, the functions of a doctor and a surgeon sometimes overlapped. Medical services were expensive, and they tried to save money on them, especially if the sick person paid for the examination himself. Therefore, in the late Middle Ages, the procedure could be carried out by workers of the nearest leper colony, and sometimes by its inhabitants.
Often neighbors would report a person with suspicious symptoms to the authorities. In this way, some settled scores with each other, so over time they began to punish for false denunciations - although not immediately.
Diagnosis did not always take place in private: the examination could be carried out in the doctor’s house, in a church, or even in the city square. The person was questioned about his symptoms, carefully examined and felt from head to toe. This is how areas of the skin that have lost sensitivity were discovered - this is truly a characteristic manifestation of leprosy. A blood sample was then taken from the patient. It was believed that when leprosy occurs, small particles resembling sand appear in it.
Doctors could not always say with certainty whether a person was sick or not. For example, in 1327, in Nîmes, France, two doctors from the University of Montpellier examined six people with suspected leprosy. Only three managed to make a diagnosis right away; the doctors debated about the rest for a long time, but never came to a consensus. Perhaps this is why city authorities began to invite educated doctors for examinations less often: too often they doubted when rendering a verdict. Practitioners from leper colonies, not burdened with the burden of university knowledge, apparently coped with the diagnosis faster. Alas, we can hardly judge who detected the disease more effectively.
Diagnosis was not limited to a medical examination. Sometimes the procedure was completed by a trial. He decided the future fate of the patient: whether he would be recognized as healthy and released or finally declared sick. What rights the sick person retained depended on the region. In some places, lepers were deprived of all property in favor of healthy relatives, and in others they could fully enter into contracts, sell property, and draw up and supplement wills.
Clinical picture
The incubation period for leprosy averages 3–7 years, but can be shortened to 6 months and extended to several decades (15–20 years). Medicine knows a case of the incubation period of leprosy, which lasted 40 years. During this period there are no symptoms of the disease. In addition, leprosy is characterized by a long latent period, during which signs of a prodromal syndrome (weakness, malaise, fatigue, drowsiness, paresthesia) do not necessarily appear.
The clinical manifestations of each form of the disease are different, but there are also general symptoms of leprosy:
- slight low-grade fever;
- weakness;
- headache;
- changes in the skin (appearance of light or dark spots, loss of sensitivity);
- the appearance of areas of skin infiltration;
- arthralgia when moving;
- formation of a vertical fold between the eyebrows;
- lengthening of the earlobes;
- loss of the outer third of the eyebrows;
- violation of the nasal mucosa.
Tuberculoid leprosy
This is the most favorable type of disease, which affects the skin, peripheral nerves and, less commonly, some visceral organs. Skin manifestations vary depending on the stage of the disease and appear as single spots or papular rashes or plaques.
In the early stage of the disease, the spots are somewhat pigmented or may have the appearance of erythematous spots with clear contours. Then, multiple small and polygonal red-bluish papules appear at the border of the spots. They quickly merge into solid plaques that rise above the surface of the skin. As the disease progresses, the center of the plaque thickens and atrophies. Thus, large ring-shaped merging border elements or figured tuberculoids are formed. Their sizes reach 10–15 mm or more, with the formation of extensive lesions located on the back, chest, and lower back. The localization of these rashes is asymmetrical.
The process also involves nails, which become dull and brittle, thicken, flake and crumble. The color of the nails is grayish, longitudinal grooves appear on them.
Symptoms of damage to the peripheral nervous system appear very early. In areas of skin damage, temperature, pain and tactile sensitivity are impaired, vellus hair loss is noted, pigmentation changes, and sebum and sweating are disrupted. The skin becomes dry, sometimes hyperkeratosis occurs. In the initial stage, either dissociation of skin sensitivity disorders or its short-term increase (hyperesthesia) is observed. Then sensitivity decreases and disappears completely.
Near skin plaques and spots, thickened and painful nerve trunks can be easily felt. Most often the radial, ulnar, parotid nerves and branches of the facial nerve are involved in the process. When large nerve trunks are damaged, paresis and paralysis occur, the motor activity of the fingers is disrupted and their contractures develop (“bird’s foot”, “drop foot”), small muscles atrophy, nails change, trophic ulcers and mutilations appear (spontaneous rejection of necrotic areas of the body - fingers , hands, nose). When the facial nerve is damaged, paresis of the facial muscles occurs - “mask-like face” and lagophthalmos (the eyelids do not close completely).
Lepromatous leprosy
The most severe variant of the disease is characterized by numerous clinical manifestations on the skin. The mucous membranes are affected early, and the internal organs and nervous system are involved in the process later. Systematization of clinical manifestations of lepromatous leprosy:
Skin manifestations
All skin rashes contain a large number of Mycobacterium leprosy. Skin rashes are presented in the form of erythematous or erythematous-pigmented spots, which are located symmetrically, are small in size and do not have clear boundaries. These spots are found on the palms, face, extensor surfaces of the legs and forearms, and in the gluteal region. The spots are shiny and have a smooth surface. As the disease progresses, the spots turn from red to brown or yellowish (rusty, copper). Sensitivity disorders and sweating in areas of skin lesions are not observed. Over a long period of time (months and years), the spots either do not change or disappear, but often transform into infiltrates and lepromas. In the case of infiltration, the spots look like plaques or an area of skin infiltration without definite boundaries. When vascular paresis or hemosiderosis occurs, the spots become brown or bluish-brown.
Skin dysfunction
In case of skin infiltration, the work of the sebaceous glands intensifies, and the skin in the affected areas becomes oily, begins to shine and become shiny. The vellus hair follicles and sweat gland ducts expand, which leads to the formation of an “orange peel.” Sweat production in the area of infiltration first decreases and then stops. In the early stage of the disease, there is no disturbance in the growth of vellus hair, but after a few years (3–5) eyelashes and eyebrows, beard and mustache begin to fall out.
Changing face
If diffuse infiltration of the face has occurred, the patient acquires a characteristic appearance - a “lion’s face”. At the same time, natural wrinkles and folds become deeper, the brow ridges protrude significantly, the nose thickens, and the cheeks, lips and chin become lobed.
Leprosy education
In the lepromatous form, the process does not involve: the scalp and eyelids, armpits and elbow bends, popliteal fossae. At the site of infiltrates, single and multiple lepromas begin to form at an early stage, ranging in size from 1 – 2 mm to 3 cm. They are usually localized on the face (on the forehead, brow ridges, wings of the nose, cheeks and chin), as well as on the ears lobes, hands, forearms and shins, in the gluteal region and on the back. Lepromas are clearly demarcated from surrounding tissues and are painless. Such formations have a smooth surface, are shiny, and sometimes peel. Over time, dense lepromas soften, and less often become very dense. Sometimes the formations resolve, leaving behind a sunken pigmented spot. If treatment is not carried out, lepromas ulcerate, and the ulcers are painful; after healing, keloid scars remain.
Damage to mucous membranes
The process always involves the nasal mucosa, and in advanced cases, the mucous membranes of the mouth, larynx, tongue and lips. Rhinitis and nosebleeds develop, nasal breathing is impaired due to the formation of lepromas in the nose, if the leproma is located on the nasal septum, the nose is deformed, and if the vocal folds are affected, the glottis narrows and aphonia (inability to speak) develops.
Other violations
Also, in the lepromatous form, the eyes are often involved in the process with the occurrence of keratitis, conjunctivitis, blepharitis, iridocyclitis and clouding of the lens. In addition, this variant of the disease is characterized by damage to the peripheral nervous system, lymph nodes, liver, vascular walls and testicles. When the nervous system is damaged, symmetrical polyneuritis develops and sensitivity in the area of skin rashes is impaired, but after a long period of time. In a very late stage of neuritis, trophic and motor disorders are formed (paresis of facial and masticatory muscles of the face, lagophthalmos, contractures and mutilations, foot ulcers).
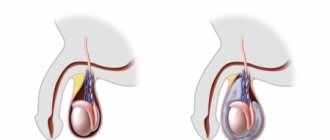
Damage to the liver leads to the formation of chronic hepatitis, and involvement of the testicles in the process leads to orchitis and orchiepididymitis. Later, testicular function is impaired, which causes infantilism and gynecomastia.
Undifferentiated and dimorphic leprosy
The dimorphic (borderline) type of the disease occurs with signs of lepromatous and tuberculoid forms. In the undifferentiated type of leprosy, the nerves (ulnar, auricular and peroneal) are affected. This is accompanied by the appearance of asymmetrical areas of the skin with increased and decreased pigmentation and a decrease in skin sensitivity and sweating until it completely stops. Involvement of nerves in the process leads to the development of polyneuritis, which ends in paralysis, deformation of the limbs and the appearance of trophic ulcers on them.
How they tried to make life easier for patients
Medieval medicine could not rid a person of leprosy, but whenever possible they tried to soften the manifestations of the disease and protect the patient from other diseases. The charter of the Antwerp leper colony of the 15th century stated: if the guests, in addition to leprosy, are struck by any curable disease, the workers are obliged to call a doctor to see them. Judging by the documents, the patients were indeed provided with assistance, although sometimes qualified doctors tried to shift the work to practicing surgeons.
To relieve symptoms, medical treatises sometimes suggested very exotic remedies. For example, the theologian and expert on natural sciences Albertus Magnus in the 13th century believed that hair could grow back on damaged areas of the skin. To do this, he recommended a potion made from the skin of a hedgehog, burned along with the needles. And Moses Maimonides, a thinker, rabbi and doctor of the 12th century, believed that the manifestations of the disease could be moderated with a remedy made from dried porcupine meat. However, these drugs were hardly popular.
The main practical means was considered to be a correct lifestyle. Patients were advised to avoid cold and heat, as well as spicy, sour and salty foods. Doctors also advised sick people - both men and women - to abstain from sex (contrary to the then widespread popular belief that it, on the contrary, helps and even heals completely). Doctors with the most radical views recommended castration - whether anyone actually decided to do this is unknown.
All these restrictions grow from the most important “theory of four bodily fluids (humors)” for medieval medicine. According to it, health depends on whether the body manages to maintain the balance of four substances: blood, phlegm, yellow and black bile. They were attributed certain qualities - “temperature” (hot or cold) and “condition” (dry or wet). For example, blood was considered “wet” and “hot.” To maintain or restore the balance of humors, medieval doctors prescribed a specially selected regimen that compensated for the missing “qualities.”
Diseases were seen as a strong shift in the balance in one direction or another. Even in Antiquity, the idea appeared that leprosy was caused by the accumulation of black or yellow bile in the veins. Both biles were considered "dry", so a regimen capable of retaining moisture in the patient's body was required. Doctors believed that sex warms the body, heats the blood and “dries out” existing moisture - therefore, it is harmful to the already “dry” bodies of patients, just like extreme temperatures or spicy food. Lost water had to be replenished with “wet” food, which primarily included meat, fish and eggs.
Many leper colonies did provide patients with a meat diet. Chickens, pigs and even cows were kept at the “houses”; fishing was allowed in local rivers. Residents of the surrounding area did not forget about the sick. Helping the suffering was considered a charitable deed that increases the chances of saving the soul, so wealthy laymen supplied hospitals with food - donations became smaller only in cases where hunger threatened the donors themselves. Archaeologist Christopher Sylvester studied the remains of people buried in the cemetery at the leper colony in Chichester, England, and found out that his patients actually ate meat much more often than poor townspeople. This was indicated by the condition of the teeth of the deceased.
It is known that the urban poor ate a lot of cheap bread, into which small fragments of stone millstones fell with poorly sifted flour. Therefore, their teeth were noticeably worn out, and the residents of the leper colony had much less such marks.
In addition to diet, measures were also taken to “cleanse” the body. In accordance with medieval ideas, the bodies of patients were from time to time riddled of “bad” blood through bloodletting. But water procedures helped much better: washing and exfoliating the affected skin. They could even temporarily restore the body's sensitivity lost due to illness.
Where and how did the patients live?
In the 21st century, life in a medieval leper colony seems like hell on earth: a place where unfortunate patients were imprisoned forever, cutting off all contact with the world and depriving them of even necessary help. But we have already seen that the condition of the inhabitants of the leper colonies was rather taken care of. It turns out that the restrictions for them were not always strict.
The medieval European leper colony was not a prison where people were locked up for life. The statutes of many institutions stated that the patient could leave the territory of the “house”, while he had to be accompanied by another sick person - the same rule applied in monasteries. Moreover, neither in Roman law nor in the canon law of the Catholic Church are there any general rules that would fundamentally prohibit lepers from contact with healthy people. There was not even a single standard on whether it was possible to divorce a spouse who had contracted leprosy - such divorces were either allowed or prohibited. Some medieval rulers did establish rules for the complete isolation of the sick on their territory, but this was not the case everywhere.
Sometimes the patient could even be evicted from the leper colony. For example, the charter of the “house” in Dudston, England stated: if a resident violated the rules of residence several times, he would have to leave the institution. A person from a rich family in such a situation had to find secluded housing in the wilderness, and a poor man, most likely, went to wander around the area, begging for alms. It was precisely such wandering patients in some regions of Europe who were required to wear a characteristic headdress and carry a rattle with them to warn of their appearance.
In many ways, the life of the leper colony community resembled monastic life. In the 12th and 13th centuries, this even caused debate about whether people with leprosy should be equated with monks. On the one hand, they practiced the same virtues: they renounced personal possessions, obeyed “elders,” and abstained from bodily pleasures. Like the inhabitants of monasteries, the sick were obliged to pray for those who helped their “house” with donations, as well as for deceased patients. Even some household rules were the same: for example, the order not to leave the monastery alone. Therefore, some theologians included leprosy patients in the hierarchy of people living in communities according to the rules established by the church, along with monks and members of spiritual knightly orders.
But the compiler of the anonymous treatise Summa Pastoralis (about 1250), on the contrary, emphasized that lepers were in no way monks: they did not fast, drank too much wine, and did not make their vows voluntarily. In addition, when they came to the “house”, they paid a certain amount or promised to inherit part of their property. If the leper colony could be likened to a monastery, then this, according to the anonymous author, would be simony - the sale of clergy, that is, a sin. Researchers believe that this book marks a turning point in public opinion about lepers from positive to negative. However, the author was largely unfair to the residents of leper colonies. Without payment, they could not settle in the “house” and would be left without help; a less strict fast was allowed to all sick people, and wine in that era could be prescribed by a doctor.
Most leper colonies accepted both men and women. They lived in different rooms, but were present together in the church, in the refectory and at general meetings where the most important matters of the “house” were discussed.
“Sisters” could defend their rights on an equal basis with “brothers.” For example, in 1235, the interests of the inhabitants of the leper colony of St. Agatha in Verona were represented by a female patient named Briana. This “house” was small, and they decided to combine it with a larger leper colony. The administration of this institution hoped not only to shelter the sick, but also to take possession of their property, including renting out their mill. Briana said that the patients at St. Agatha's "house" are against such a plan. The woman demanded that the mill be dismantled and moved to the territory of the new leper colony so that the sick could use it as before. And in one of the “houses” of Genoa at the beginning of the 15th century, a meeting of the inhabitants was once held not in the common hall, but at the bedside of the patient Petrina: she was too weak to go into the hall, but wanted to be present.
How the sick were treated
Stereotypes have preserved the memory of negative attitudes towards leprosy patients. They were ostracized, considered repulsive and dangerous, and suspected of a variety of crimes. For example, in 1321, rumors spread throughout France that lepers intended to poison the water in rivers, springs and wells in order to spread their disease throughout the country. The reason given was the hatred of the sick for their healthy neighbors, the desire to appropriate other people's lands and power, and the assistance of Jewish moneylenders. The panic in society was so strong that many lepers were executed without trial.
Might be interesting
Seeds of disease in the Holy Land: what the crusaders were sick with and how they were treated
Some researchers believed that this attitude towards the sick was rooted in the Old Testament descriptions of lepers as sinners, justly punished by God for their misdeeds.
The translators of the Septuagint, a translation of the Old Testament into ancient Greek, identified leprosy with the biblical concept of tsaraat, a skin condition that makes a person ritually unclean.
Medieval sources directly connect leprosy with various sinful acts: lust, fornication, blasphemy, falling into heresy. Other scientists, on the contrary, see the reasons in the remnants of the pagan view of the world. It is not without reason that it is believed that the most stringent standards for the isolation of lepers arose under the influence of the customs of the Germanic peoples, recorded in the “barbaric truths.” These laws were based on an ethical system, according to which the strongest members of society, those capable of bringing the greatest benefit to it, should have the maximum rights. This position was contrary to the Christian one, which calls for caring for the weak, but its influence remained in Europe for centuries.
Circumstances could also lead to persecution of patients. For example, at the beginning of the 14th century there were many economic problems in France, and rumors spread throughout Europe about a possible Muslim invasion due to the fact that at the turn of the 13th and 14th centuries the Crusaders finally lost all territories in the Holy Land. Thus, leprosy patients became scapegoats on which healthy fellow citizens could take out their discontent, anger and fear.
Negative attitudes towards the sick and the violence associated with them really existed and remained in the memory of Europeans for a long time. However, there was another side to the medieval perception of leprosy. The marks left by the disease were considered a sign of chosenness, of God’s special favor to the unfortunate. It was believed that physical suffering cleanses the soul from sin, therefore such a severe illness serves as a guarantee of the salvation of the soul after death. By sending a person a painful and clearly visible illness from the outside, the Lord gave him the opportunity to live a righteous life, close to a monastic one (remember the debate about whether leper colonies should be equated with monasteries). And in the lives of saints and sermons there are many stories where Christ himself was hiding under the guise of an unfortunate leper.
This view originated in the first centuries of Christianity and is expressed in the writings of many Church Fathers. They actually helped the sick. Having become bishops, John Chrysostom and Basil the Great ordered the opening of “shelters” for lepers in their lands. The leper colony created by Vasily was so large that it was called the “new city.” The situation in Asia Minor in the 4th century was reminiscent of the wave of leprosy that covered Europe in the 12th century, so numerous patients quickly populated new “homes.”
Many early Christian theologians considered the Old Testament references to leprosy to be allegorical. They separated the biblical concept of “tsaraat” from real leprosy, considering the former not so much a physical ailment as a symbolic designation of sin.
According to Cyril of Alexandria, the ritual described in the Bible, when a healed leper was sprinkled with the blood of a sacrificial bird, was a prototype of Christ’s sacrifice for humanity. These authors compared the real illness rather with the suffering of the biblical Job. One of the tests sent to him by God was leprosy, which disfigured the body of the righteous man with terrible scabs. Over time, in the texts of the Church Fathers, the image of a “sacred illness” arose, with which the Lord marks those whom He especially favors. Therefore, it is the duty of a Christian to overcome disgust and fear of the sick and alleviate their suffering in this imperfect life, so that they become intercessors before God in the future life. This point of view was influential along with the “Old Testament” and “barbarian” ones - even centuries after the division of the Christian Church into Catholic and Orthodox. Perhaps it was she who forced the Europeans not only to expel the sick, but to take care of them whenever possible.
People of the Middle Ages perceived leprosy in two ways: both as a disgusting but fair punishment, and as a sign of chosenness and piety. But over time, the second side was almost forgotten - it was replaced by terrible images of lifelong isolation and cruel reprisals against lepers.
New diseases and the dark legacy of medieval leprosy
Today, Hansen's disease is gradually becoming a thing of the past. Modern medicines work, the number of infections is falling all over the world, and many sick people are able to avoid disability. But the stigma surrounding the diagnosis was stronger than the disease itself. Those affected still face leprophobia and a lack of knowledge among those around them, including in clinics and hospitals - for example, doctors in non-specialized institutions sometimes refuse to examine them.
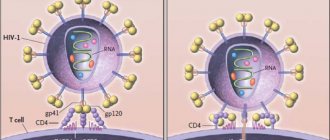
The negative associations that accompany leprosy carry over to other diseases. Thus, in the 1980s, HIV infection was repeatedly called the “new leprosy.” Along with this term, the perception of HIV infection also inherited a negative attitude towards patients.
The diagnosis is often loaded with non-medical associations, linking it with disapproved behavior, promiscuity, and, in a broad sense, with sin. A disease that has specific causes and can be treated begins to be perceived as a punishment from above that cannot be prevented, and those who become ill begin to be perceived as sinners.
Some researchers call this view of illness “diagnostic medievalism,” implying both a moral assessment and “medieval cruelty” in the perception of the disease and people diagnosed. But data from historical sources show that even in the Middle Ages the attitude towards the sick was not entirely negative. By studying these experiences, we can separate the facts from the prejudices of the past.
Diagnosis of leprosy
Diagnosis of the disease is primarily based on the clinical picture. Detection of leprosy in the later stages is not difficult (loss of eyebrows, eyelashes, presence of leprosy, paresis and paralysis, loss of fingers, hands, deformation of the nose, “lion’s face” and other signs). In the early stage of the disease, the signs are blurred and atypical, which leads to difficulties in making a diagnosis. A doctor of any specialty (infectious disease specialist, neurologist, dermatologist and others) can encounter leprosy, which is associated with a variety of skin manifestations and lesions of the peripheral nervous system that do not respond to prescribed treatment.
Laboratory methods, which include bacterioscopic and histological studies, help to accurately diagnose leprosy:
- Scrapings from the nasal mucosa, earlobes, chin and fingers are examined bacterioscopically;
- Lepromas, lymph nodes and wound discharge from trophic ulcers are examined histologically.
The resulting preparations are stained according to Nelson, and Mycobacterium leprosy is detected in the smears.
In order to determine the tactile, pain and temperature sensitivity of the skin, functional tests are performed (with nicotinic acid and histamine, mustard plaster and Minor's reagent).
The body's reaction to lepromin is studied (skin tests). In the tuberculoid form, the lepromin test gives a positive answer, and in the lepromatous form - negative. The undifferentiated version of leprosy gives a weakly positive or negative reaction, and the borderline version gives a negative reaction.