Table of contents
- Etiology and pathogenesis
- Pathogenesis of psoriasis
- Clinical manifestations
- Accurate diagnosis and verification of the severity of psoriasis
- Principles of treatment
Psoriasis is a complex chronic multifactorial inflammatory disease characterized by excessive proliferation of epidermal keratinocytes and an increase in their turnover rate. It can begin at any age, but more often at 20–30 or 50–60 years.
In our company you can purchase the following equipment for diagnosing psoriasis:
- FotoFinder (FotoFinder)
On average, 2–3% of people worldwide suffer from psoriasis, but the incidence varies greatly regionally. For example, in the USA the prevalence is about 2.2%, and among South American Indians it is 0%, i.e. Not a single case of psoriasis was identified in a survey of 26 thousand people. The disease is more often diagnosed in light-skinned people (2.5%) than in dark-skinned people (1.3%).
According to ICD-11, psoriasis is included in group 14 “Skin diseases”, subgroup “Papulosquamous diseases”, section EA90 “Psoriasis”.
Preventive measures
Prevention of the disease requires compliance with simple rules. Firstly, you need to protect your nervous system, because stress factors can trigger psoriasis. Secondly, it is necessary to strengthen the immune system and lead a healthy lifestyle:
- exclude fried, salty, fatty foods from the diet and eat healthy;
- do not smoke or drink alcohol, as this may worsen symptoms;
- take care of your skin - avoid frostbite, prolonged exposure to the scorching sun, avoid mechanical damage;
- wear underwear made from natural fabrics.
Etiology and pathogenesis
Among the causes of psoriasis are the following:
- Genetics - the disease is associated with certain human leukocyte antigen (HLA) alleles, the most “strong” of which is HLA-Cw6. Other associated alleles are HLA-B27, HLA-B13, HLA-B17 and HLA-DR7.
- Immunology - The immunological concept of psoriasis is supported by high levels of cutaneous and circulating tumor necrosis factor alpha (TNF-α), as well as the fact that treatment with TNF-α inhibitors often puts patients into remission. In addition, it was noted that after certain immunological events, guttate psoriasis can occur - for example, after streptococcal pharyngitis, cessation of corticosteroid therapy, etc.
- Obesity is an incompletely studied factor. Whether excess weight alone, a genetic predisposition to obesity, or a combination of these factors influences the development of psoriatic plaques is not known. However, it has been noted that with an increase in body weight, the condition of psoriasis worsens, as well as vice versa, with a decrease in weight, the course of the disease improves.
- Stress and the environment - psychological experiences can both provoke the development of psoriasis and aggravate it. Exacerbations of the disease are also caused by injuries, infections (streptococcus, staphylococcus, human immunodeficiency virus), alcohol, and medications (aspirin, beta-blockers). One study documented an increase in the incidence of psoriasis flare-ups in patients with chronic gingivitis. Treatment of gingivitis allowed us to go into remission, but did not affect the disease in the long term, which once again emphasizes the complexity and multifactorial nature of psoriasis treatment methods.
Interestingly, 2.5% of people with HIV develop progressive psoriasis due to decreased CD4 T cell counts. This does not fit into modern understanding of the disease ( Fig. 1 ), since the leading hypothesis states that T cells are hyperactive in psoriasis , and treatment aimed at reducing their number usually reduces the severity of psoriasis. It is possible that a decrease in the number of CD4 T cells in patients with HIV leads to an increase in the activity of CD8 T cells, which causes the progression of psoriasis.
Rice. 1. General understanding of the etiology and pathogenesis of psoriasis, as well as the development of associated conditions (World Health Organization, WHO)
- The first sector (internal, shaded) is genetics, environmental triggers.
- The second sector is microinflammation, insulin resistance, obesity.
Two internal sectors include the basic predisposing factors and pathogenetic components of psoriasis. The main clinical sign is inflammation ( Inflammation ).
- The third sector is myocardial infarction, atherosclerosis, stroke, metabolic syndrome.
- The fourth sector is depression, anxiety disorders.
The two middle sectors reflect the transition to systemic lesions - from cutaneous psoriasis to psoriatic arthritis ( Psoriasis - Arthritis ) and related problems. Main clinical signs: cardiovascular pathologies ( CVD ), psychiatric complications ( Psychiatry ).
- The fifth sector is patient stigmatization, increased cost and duration of treatment, and lack of satisfaction with therapy.
- The sixth sector (outer, with an arrow) - smoking, alcohol abuse, possible secondary obesity, addiction, compliance (level of adherence to treatment)
The two external sectors reflect the consequences of the disease ( Consequences ) and the patient's quality of life ( Qol ), as well as the burden of psoriasis ( BoD ), i.e. deterioration in a person’s quality of life due to illness.
https://apps.who.int
How is treatment carried out at the Paramita Oriental Medicine Clinic?
But the first step on the path to getting rid of psoriatic plaques is a preliminary appointment with a specialist. At this appointment, the doctor will determine the nature of the disease, its stage of development, the degree of damage to the skin, and the possible causes of this disease in a particular patient.
Based on the data obtained during the survey - and, if necessary, a laboratory examination is also prescribed - the doctor determines the necessary treatment and prescribes a course of complex therapy sessions.
The cost of preliminary admission is 500 rubles.
Pathogenesis of psoriasis
The pathogenesis of the disease is not fully understood. It has been noted that a large number of activated T cells penetrate the epidermis, which trigger the proliferation of keratinocytes . The rate of their renewal changes from the usual 23 days to 3–5 days, which leads to the appearance of pathologically altered cells and peeling of the skin. Keratinocytes, which normally lose nuclei in the granular layer of the epidermis, retain them in psoriasis, which results in a disruption of the keratinization process - parakeratosis .
Against this background, uncontrolled inflammation with excessive production of cytokines: tumor necrosis factor alpha (TNF-α), interferon gamma, interleukin-12. It has been noted that a surge in TNF-α levels corresponds to exacerbations of psoriasis.
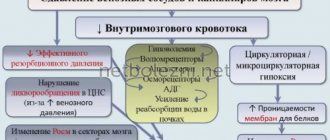
In the affected skin there is increased vascularization and dilation of superficial vessels. The main triggers of angiogenesis in psoriasis come from the epidermis - in particular, keratinocytes secrete vascular endothelial growth factor A (VEGF-A). Sources of angiogenic factors are also macrophages and fibroblasts, and additional participants are hypoxia-inducible factor (HIF), tumor necrosis factor α (TNF-α), interleukins (IL)-1, -6, -8, etc. ( Fig. 2 ) But the most important component is VEGF-A - it activates blood and lymphatic vessels, directly influencing the attraction of inflammatory cells to the psoriatic lesion. Serum VEGF-A levels correlate positively with disease severity and negatively with the success of standard therapy, indicating a critical role for VEGF-A in disease progression.
Rice. 2. The role of the vascular component of the skin and angiogenesis in the pathogenesis of psoriasis (Heidenreich R., et al. Angiogenesis drives psoriasis pathogenesis. Int J Exp Pathol 2009; 90(3): 232–248)
With the participation of vascular endothelial growth factor ( VEGF ), the proliferation of keratinocytes and vascular endothelial cells is triggered, which promotes angiogenesis. T helper cells ( Th ) produce interleukin-17 ( IL -17 ), which triggers the production of pro-angiogenic factors - this further enhances angiogenesis. Against this background, dendritic cells ( DC ) of the epidermis act on the population of T helper cells ( Th ), which begins to synthesize interferon gamma ( IFN -γ ), which suppresses angiogenesis. But this doesn’t help for long, because... other proangiogenic factors are activated: VEGF , bFGF , IL -8 , triggering further growth of small vessels and “unwinding” the pathogenesis of psoriasis.
- VEGF - vascular endothelial growth factor
- IL - interleukin
- IFN - interferon
- TNF - tumor necrosis factor
- TGF - tumor growth factor
- MMP—matrix metalloproteinases
- bFGF - basic fibroblast growth factor
- ECs - endothelial cells
- DC - dendritic cells
- Th - T-helpers
- N - neutrophils
Clinical manifestations
The most common cutaneous manifestations of psoriasis are erythematous patches, papules, plaques, and scaling. Usually the spots appear first, then they transform into papules, then into well-circumscribed silvery plaques covering the erythematous surface of the affected skin.
Patients with psoriasis typically:
- The sudden appearance of small areas of red, scaly skin.
- Family history of a similar condition in the anamnesis.
- Recent streptococcal throat infection, viral infection, antimalarial drug use, trauma, stress.
- Gradual deterioration of the condition of erythematous areas, their enlargement and merging with each other.
- Soreness - with erythrodermic psoriasis.
- Itching - with eruptive or guttate psoriasis.
- Febrile condition - with pustular or erythrodermic psoriasis.
- Dystrophy of the nail plates is possible.
- Joint pain, including without obvious skin manifestations.
- Ophthalmic lesions - occur in 10% of patients, most often these are redness and lacrimation due to conjunctivitis or blepharitis.
Clinical forms of psoriasis (Fig. 3):
- Plaque psoriasis - manifests itself as itchy red patches on the skin, with excess scaling and flaking. Lesions typically occur on the extensor (outer) side of the joints and scalp ( Figure 3A ). Most patients are embarrassed by these plaques, wear covered clothing and avoid exposing the affected areas. 38–76% of patients experience a Koebner reaction—the appearance of new plaques at the site of injury after 7–14 days. In some cases, the Koebner reaction is reversible, i.e. the lesions disappear as the injured area heals. 10–20% of patients experience psoriatic arthritis with joint pain, stiffness and deformity.
- Guttate psoriasis is characterized by the sudden appearance on the body and proximal extremities of pinkish guttate papules with a diameter of 1–10 mm ( Fig. 3B ). They usually do not progress while at the same stage of development, but may be accompanied by itching.
- Inverse psoriasis - irregularly shaped redness occurs on the flexor (inner) surfaces of the joints, in the groin, and armpits ( Fig. 3C ). It may be mistaken for a fungal infection.
- Pustular psoriasis is characterized by typical pustules against a background of erythematous skin that appear on the body, less often on the face, elbow bends, and in the anogenital area ( Fig. 3 D ). There is also an increase in body temperature up to fever (febrile condition), tachycardia, redness of the oropharyngeal mucosa, “geographical” tongue, onychodystrophy (thinning and brittleness of nails).
- Erythrodermic psoriasis - manifests itself as severe redness and peeling over large areas of the body ( Fig. 3 E ). The skin exfoliates not in small scales, as usual, but in large layers. Patients experience moderate to severe itching and pain. Body temperature may rise and fall sharply, especially on very hot or cold days, and tachycardia may occur.
Rice. 3. Clinical forms of psoriasis: A - plaque, B - guttate, C - inverse, D - pustular, E - erythrodermic (Danish national service on dermato-venereology)
On the website you need to put down the letters A-BCDE: plaques A, dots B, redness in the anus C, heel D, crossed arms E
Risk factors
- Heredity.
- Violation of lipid metabolism in the body.
- Disturbances of the endocrine system.
- Infectious diseases
- Stress, depression, nervous disorders and shocks.
Red spots on the skin after stress
Diagnosis of skin diseases
Risk factors that provoke the manifestation of vulgar psoriasis also include mechanical trauma to the skin, taking a number of medications, atherosclerosis and diabetes.
Accurate diagnosis and verification of the severity of psoriasis
The severity of psoriasis depends on the area of skin damage:
- Light - up to 2% of the body surface.
- Average - from 3 to 10%.
- Severe - more than 10% of the body surface.
It is not possible to determine the severity of psoriasis by eye; one can only guess it based on the experience of a specialist and the external signs of the disease in the patient. To accurately diagnose psoriasis, instrumental methods should be used - for example, FotoFinder PASIvision .
FotoFinder PASIvision is based on Automatic Total Body Mapping (ATBM) technology, which allows you to quickly obtain standard images of the patient's entire body. A special camera takes 16 digital photographs, including those using a polarizing filter.
Next, the program automatically analyzes the area of skin lesions and the severity of psoriasis according to PASI - Psoriasis Area and Severity Index . PASI is the most important criterion not only for primary diagnosis, but also for determining the effectiveness of treatment, disease control and prognosis.
To identify the dynamics and choose a method of effective treatment of psoriasis, the doctor can open two images of the same area at once, taken at different times. After selecting the desired comparison method, the program automatically calculates the PASI of the specified areas - this is the most visual and reliable method of monitoring the effectiveness of the therapy.
The doctor has access to convenient sorting of images and patients, as well as a number of reports that can be printed or sent by email.
Advantages of taking tests in the laboratory of JSC "SZDCM"
- Easy registration and no queues.
- Anonymity and confidentiality of data.
- Accurate diagnostics thanks to the latest equipment.
- Quick availability of results.
- Tactful, qualified staff.
Laboratory terminals operate in St. Petersburg and the Leningrad region, Pskov, Veliky Novgorod and Kaliningrad. You can get tested at any of them, regardless of your place of registration and residence. The laboratories have a single database, which means you can get the result in any department, in a way convenient for you.
Principles of effective treatment of psoriasis
- Local therapy:
- Vitamin D analogues
- Topical corticosteroids (hydrocortisone, betamethasone)
- Topical retinoids
- Phototherapy or PUVA therapy
- Systemic therapy:
- Methotrexate
- Cyclosporine
- Acitretin
- Biological agents
The simplest and most effective way to put skin lesions into remission is daily exposure to the open sun , local hydration and general relaxation to avoid stress.
You can find over-the-counter tar or tar-based medications in pharmacies that are suitable for treating psoriatic plaques. Local corticosteroids, anthralin, tazarotene, salicylic acid, calcipotriol (an analogue of vitamin D) are useful. In general, combination treatment is found to be more effective than monotherapy. A combination of calcipotriol or topical retinoids with topical corticosteroids works well.
PUVA therapy is based on the use of local or systemic psoralens and ultraviolet A (UVA, 320–400 nm). Its name comes from the English PUVA therapy, where the abbreviation stands for “ P soralen and U ltra V iolet A ”, i.e. “psoralen and ultraviolet A.” Photosensitizers enter into photo-oxidative reactions in pathologically altered skin cells, inhibiting their excessive mitotic activity. Currently, 8-methoxypsoralen (8-MOP), 5-methoxypsoralen (5-MOP) or 4,5′,8-trimethylpsoralen (TMP) are used. Long-term courses of PUVA therapy help achieve remission, but increase the risk of squamous cell skin cancer and malignant melanoma in fair-skinned Europeans.
Narrowband UVB therapy is less effective than PUVA, but is gentler on the skin.
In severe cases, systemic medications such as acitretin (a retinoid), methotrexate, cyclosporine, 6-thioguanine, azathioprine, etc. can be used to effectively treat psoriasis. Retinoids have been reported to cause dry eyes, blepharitis, corneal opacities, cataracts, and decreased night vision. Other adverse effects include gastrointestinal dysfunction and liver damage (acitretin, 6-thioguanine, azathioprine, methotrexate), bone marrow suppression (6-thioguanine, methotrexate, azathioprine, hydroxyurea), and kidney damage (cyclosporine).
If you have psoriatic arthritis or persistent (often worsening) psoriasis, you can use biological agents - ustekinumab, adalimumab or secukinumab.
Prevention methods
An additional condition for containing the worsening of the disease is to follow several recommendations:
- Switching to dietary nutrition. Experts strongly advise patients with psoriasis to avoid foods containing simple sugars, animal fats, as well as foods with a high degree of allergenicity (nuts, alcohol, chocolate, etc.). The basis of nutrition for psoriasis should be fermented milk products, vegetable oils, cereal-based cereals, as well as dietary types of meat and fish.
- Maintain personal hygiene. For personal hygiene, you should use delicate products that do not contain dyes, artificial fragrances, or aggressive synthetic components. Water procedures should last no more than 15 minutes, and the water should be warm.
- Wearing underwear made from natural soft fabrics. It is better to choose loose-fitting clothes so that they do not rub or restrict movement. Products made from natural cotton and knitwear will be optimal. Synthetics and rigid fabrics must be excluded.
Some patients may require psychocorrection, taking specialized medications with a sedative, sedative or antidepressant effect.