It's all about collagen
By the way, it is believed that this pathology occurs predominantly in female faces. Its prevalence is 5–7% of the total population, but every year the number of gutta-percha women and men is growing. This syndrome is more common among eastern peoples. There are especially many “rubber” people living in Asia, a little less of them in Africa and much less in Europe.
In some families, unusual stretch marks are inherited. But despite the fact that not in all cases people with snake-like flexibility need treatment, sometimes excessive stretchability of the ligaments can lead to problems.
The disease we are talking about today is a consequence of weakness of the ligamentous apparatus. And the reason for this phenomenon lies in molecular changes within the main structural protein of the body - collagen. The same protein is part of the skin, hair, nails, and it also makes up the walls of blood vessels and ligaments that support internal organs (it is due to these “suspensions” that the liver, kidneys, uterus and other organs can occupy the physiologically correct location in the body).
With a gross genetic mutation that disrupts the synthesis of collagen in the body, a person may experience severe, but, fortunately, rare hereditary diseases, in which patients experience excessive flexibility of the joints, and also in the first case, multiple bone fractures, and in the second - very tensile skin and the possibility of spontaneous rupture of blood vessels.
With joint hypermobility syndrome, the situation is less sad, but unpleasant consequences also exist. The altered protein impairs the firmness and elasticity of the ligamentous apparatus, as a result of which the ligament overstretches and becomes flaccid during the movement of the joint. Unfortunately, changes in the molecular structure of collagen in people with joint hypermobility syndrome are inherited and persist for life.
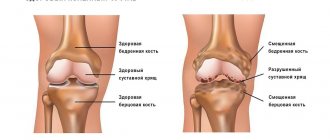
Since almost no system of the body can function without the participation of collagen, there can be many diseases associated with the weakness of connective tissue structures. This includes the early appearance of wrinkles, prolapse of heart valves (excessive sagging of the valves), prolapse of internal organs, and varicose veins. But most often, patients with joint hypermobility have problems with the joints and spine. In particular, this pathology can be considered a risk factor for the development of arthrosis.
Hypermobile type of Ehlers-Danlos syndrome.
One type of Ehlers-Danlos syndrome is hypermobile . It is distinguished from other types by significantly pronounced hypermobility of the joints, often accompanied by chronic pain and numerous dislocations. And since the probable cause of hypermobility is in the genes responsible for collagen synthesis, with this type, as with other types of EDS, the skin, internal organs and body systems suffer. Among the complaints of patients with the hypermobile type of EDS: instability in the joints, chronic and debilitating pain in the joints and ligaments, easy bruising, chronic fatigue, and pulse fluctuations.
To diagnose the hypermobile type of Ehlers-Danlos syndrome, the so-called Villefranche criteria are used.
Benign hypermobility syndrome and hypermobility type of Ehlers-Danlos syndrome - the same thing or different diseases?
Most often, doctors consider benign joint hypermobility syndrome and the hypermobile type of Ehlers-Danlos syndrome as separate diseases. However, in 2014, an article was published [3], refuting this opinion and proving that these are the same disease .
Often the same person at different ages fits different diagnoses. In childhood, he can be diagnosed with the hypermobile type of EDS based on pronounced hypermobility and elastic skin, and in adulthood, when all possible complications and symptoms have already appeared, he is diagnosed with hypermobility syndrome based on the Brighton scale.
The study [3] examined the medical records of 23 Italian families, each of which had patients with hypermobility. It turned out that in almost 90% of families there were several diagnoses within the same family. That is, for example, a parent was diagnosed with ADHS (in the article it is called joint hypermobility syndrome), and the child was diagnosed with a hypermobile type of EDS.
From the article it becomes quite obvious that both of these diagnoses have the same genetic cause. That is, this is, in fact, one and the same disease, or at least two facets of one disease. And while the diagnostic criteria are not developed as well as we would like, the doctor usually makes a diagnosis at his own discretion. The situation is aggravated by the fact that there is no genetic analysis to diagnose this syndrome.
- Simpson MR: Benign Joint Hypermobility Syndrome Evaluation, Diagnosis, and Management. JAOA 2006.
- Simmonds JV, Keer RJ: Hypermobility and the hypermobility syndrome. Manual Therapy 2007.
- Castori M, Dordoni C, Valiante M, Sperduti I, Ritelli M, Morlino S, Chiarelli N, Celletti C, Venturini M, Camerota F, Calzavara-Pinton P, Grammatico P, Colombi M. 2014. Nosology and inheritance pattern(s) of joint hypermobility syndrome and Ehlers-Danlos syndrome, hypermobility type: A study of intrafamilial and interfamilial variability in 23 Italian pedigrees. Am J Med Genet Part A 9999A:1–11.
Pull-pull
Most often, with this syndrome, the first complaints occur during the period of most intensive growth, that is, at approximately the age of 14–18 years. “Gutta-percha” teenagers begin to be bothered by pain in the joints (usually the knees, ankles, small joints of the hands) or in the spine. The pain can range from moderate to very severe. Often, such teenagers have scoliosis, chronic foot fatigue, and flat feet. Patients with this syndrome have a high tendency to frequent injuries (sprains, subluxations of joints). By the way, these symptoms (especially if they appeared at a young age) can disappear as spontaneously as they appear. Therefore, they were previously mistakenly classified as “growing pains.”
A simple screening test using the Beighton method helps the doctor determine whether a teenager has joint hypermobility syndrome. The doctor asks the young patient to do 5 different types of movements and evaluates their performance. But there are 9 exercises in total (since our limbs are paired).
Each movement that demonstrates increased flexibility is worth 1 point. We can talk about the presence of the syndrome if, in addition to joint pain, young people score 4 points or higher, and those over 50 score from 1 to 3 points. And here are the test exercises (all except the last one are performed for both right and left limbs):
1. Bend the little finger back (1 point – if the angle of deviation is more than 90°). 2. Bend the thumb of the hand (1 point - if it easily touches the inside of the forearm). 3. Straighten the arm (1 point – for hyperextension at the elbow joint by more than 10°). 4. Straighten the leg (1 point – for hyperextension in the knee joint by more than 10°). 5. Bend the torso forward with straight legs (1 point for touching the palms to the floor).
However, in the absence of complaints from the musculoskeletal system, excessive joint mobility in comparison with the average can be considered as a constitutional feature and even an age norm. Before prescribing treatment, it is necessary to carry out a differential diagnosis, its purpose is to exclude other diseases that may also affect the joints (arthrosis deformans, rheumatoid arthritis, etc.). The patient will have to take an x-ray of the joints (necessarily symmetrical, on both arms or legs), CT or MRI and take a general clinical blood test.
JOINT HYPERMOBILITY SYNDROME in general practice
Joint hypermobility syndrome (JMS) is a common reason for patients of any age seeking medical help. The clinical manifestations of VHMS are varied and can mimic other, more well-known joint diseases. Due to insufficient familiarity with this pathology among general practitioners, and in some cases rheumatologists and orthopedists, the correct diagnosis is often not established. Traditionally, the doctor's attention is drawn to identifying limited range of motion in the affected joint, rather than determining excess range of motion. Moreover, the patient himself will never report excessive flexibility, since he has coexisted with it since childhood and, moreover, is often convinced that all people have the same capabilities. Two diagnostic extremes are typical: in one case, due to the absence of objective signs of pathology in the joints (except for visible hypermobility) and normal laboratory parameters in a young patient, “psychogenic rheumatism” is determined; in the other, the patient is diagnosed with rheumatoid arthritis or a disease from the group of seronegative spondyloarthritis and prescribe appropriate, by no means harmless, treatment.
What is considered joint hypermobility?
Among the many proposed methods for measuring range of motion in joints, Beighton's method, which is a nine-point scale assessing the subject's ability to perform five movements (four paired for the limbs and one for the trunk and hip joints), has received general recognition. Beighton proposed a simplified modification of the previously known method of Carter and Wilkinson (1964). The movements are shown in Fig. 1.
| Figure 1. Change in range of movements 1. Passive extension of the little finger of the hand more than 90°. 2. Passive pressing of the thumb to the inside of the forearm. 3. Hyperextension of the elbow joint more than 10°. 4. Hyperextension in the knee joint more than 10°. 5. Forward tilt of the body with palms touching the floor with straight legs. |
This is a simple and time-consuming screening procedure that has been widely used in both clinical and epidemiological studies. Based on a number of epidemiological studies, norms of joint mobility for healthy people were determined. The degree of joint mobility is distributed in a population in a normal way, that is, not according to the “all or nothing” principle, but in the form of a sinusoidal curve. The usual Beighton score for Europeans is from 0 to 4. But the average, “normal” degree of joint mobility varies significantly across age, gender and ethnic groups. In particular, when examining healthy individuals in Moscow aged 16-20 years, more than half of women, and more than a quarter of men, demonstrated a degree of HMS exceeding 4 points according to Beighton. Thus, in the absence of complaints from the musculoskeletal system, excessive joint mobility in comparison with the average can be considered as a constitutional feature and even an age norm. In this regard, in pediatric practice there are no generally accepted standards for joint mobility - this indicator changes significantly during the period of child growth.
Can excessive joint flexibility be acquired or is it a hereditary trait?
Acquired excessive joint mobility is observed in ballet dancers, athletes and musicians. Long-term repeated exercises lead to stretching of the ligaments and capsules of individual joints. In this case, local hypermobility of the joint(s) occurs. Although it is obvious that in the process of professional selection (dancing, sports) persons who are initially distinguished by constitutional flexibility have a clear advantage, the fitness factor undoubtedly takes place. Changes in joint flexibility are also observed in a number of pathological and physiological conditions (acromegaly, hyperparathyroidism, pregnancy). Generalized HMS is a characteristic feature of a number of hereditary connective tissue diseases, including Marfan syndrome, osteogenesis imperfecta, and Ehlers-Danlos syndrome. These are rare diseases. In practice, a doctor much more often has to deal with patients with isolated GMS, not associated with training and, in some cases, combined with other signs of weakness of connective tissue structures. It is almost always possible to establish the familial nature of the observed HMS and concomitant pathology, which indicates the genetic nature of the observed phenomenon.
Definition of joint hypermobility syndrome
The term “HMS syndrome” itself belongs to the English authors Kirk, Ansell and Bywaters, who in 1967 thus designated a condition in which there were certain complaints from the musculoskeletal system in hypermobile individuals in the absence of signs of any other rheumatic disease.
Subsequent work made it possible to specify the nosological boundaries of this syndrome, which was defined as “benign joint hypermobility syndrome,” in contrast to the prognostically more severe types of Ehlers-Danlos syndrome and other hereditary connective tissue dysplasias.
The latest, so-called Brighton criteria for benign HMS syndrome (1998) are presented in the table. These criteria also attach importance to extra-articular manifestations of weakness of connective tissue structures, which makes it possible to speak of HMS syndrome in persons with a normal range of motion in the joints (as a rule, we mean older persons).
Prevalence of joint hypermobility syndrome
HMS syndrome is understood as a combination of HMS and any complaints from the musculoskeletal system caused by weakness of the ligamentous system. The true prevalence of HMS syndrome is virtually unknown. Constitutional HMS is detected in 7-20% of the adult population. Although most patients first complain during adolescence, symptoms can appear at any age. Therefore, the definitions of “symptomatic” or “asymptomatic” HMS are quite arbitrary and reflect only the state of an individual with HMS at a certain period of life. We can talk about the frequency of detection of FHMS according to individual clinics. Thus, in one of the large European rheumatology clinics, this diagnosis was established in 0.63% of men and 3.25% of women out of 9275 patients admitted for inpatient examination. But these data do not reflect the true picture, since most patients with HMS syndrome do not require hospital treatment. According to domestic data, the proportion of patients with FHMS is 6.9% at an outpatient appointment with a rheumatologist (Gowert V.R., 1996). Due to the already mentioned insufficient knowledge of doctors about this pathology, these patients are often registered under other diagnoses (early osteoarthritis, periarticular lesions, etc.).
Clinical manifestations of HMS syndrome
The clinical picture of HMS is diverse and includes both articular and extra-articular manifestations, which are generally reflected in the mentioned Brighton criteria for HMS syndrome.
A careful history taking is a significant aid in diagnosis. A characteristic fact in the patient’s life history is his special sensitivity to physical stress and a tendency to frequent injuries (sprains, subluxations of joints in the past), which suggests a failure of the connective tissue. The excess range of motion in the joints detected by the Beighton method complements the actual clinical forms of manifestation of VHMS.
Articular manifestations
- Arthralgia and myalgia. The sensations may be painful, but are not accompanied by visible or palpable changes in the joints or muscles. The most common localization is the knee, ankle, and small joints of the hands. In children, severe pain in the hip joint has been described, responding to massage. The severity of pain is often influenced by the emotional state, weather, and the phase of the menstrual cycle.
- Acute post-traumatic articular or periarticular pathology, accompanied by synovitis, tenosynovitis or bursitis.
- Periarticular lesions (tendinitis, epicondylitis, other enthesopathies, bursitis, tunnel syndromes) occur more often in patients with VHMS than in the general population. They occur in response to an unusual (unusual) load or minimal trauma.
- Chronic mono- or polyarticular pain, in some cases accompanied by moderate synovitis provoked by physical activity. This manifestation of VHMS most often leads to diagnostic errors.
- Repeated dislocations and subluxations of joints. Typical locations are the shoulder, patellofemolar, and metacarpophalangeal joints. Sprained ligaments in the ankle joint.
- Development of early (premature) osteoarthritis. This can be either true nodular polyosteoarthrosis or secondary damage to large joints (knees, hips) that occurs against the background of concomitant orthopedic anomalies (flat feet, unrecognized hip dysplasia).
- Back pain. Thoracalgia and lumbodynia are common in the population, especially in women over 30 years of age, so it is difficult to make an unambiguous conclusion about the connection of these pains with joint hypermobility. However, spondylolisthesis is significantly associated with GMS.
- Symptomatic longitudinal, transverse or combined flatfoot and its complications: medial tenosynovitis in the ankle joint, valgus deformity and secondary arthrosis of the ankle joint (longitudinal flatfoot), posterior talar bursitis, thalalgia, corns, hammertoe deformity, Hallux valgus (transverse flatfoot) ).
Extra-articular manifestations. These signs are natural, since the main structural protein collagen, which is primarily involved in the described pathology, is also present in other supporting tissues (fascia, dermis, vascular wall).
- Excessive extensibility of the skin, its fragility and vulnerability. Striae not associated with pregnancy.
- Varicose veins that begin in youth.
- Mitral valve prolapse (before the introduction of echocardiography into widespread practice in the 70-80s, many patients with HMS syndrome were observed by a rheumatologist with a diagnosis of “rheumatism, minimal degree of activity” due to complaints of joint pain and heart murmurs associated with prolapse valves).
- Hernias of various localizations (umbilical, inguinal, white line of the abdomen, postoperative).
- Prolapse of internal organs - stomach, kidneys, uterus, rectum.
Thus, when examining a patient with suspected VHMS, and this is every young and middle-aged patient with non-inflammatory joint syndrome, it is necessary to pay attention to possible additional signs of systemic connective tissue dysplasia. Knowledge of the phenotypic manifestations of Marfan syndrome and osteogenesis imperfecta allows us to exclude these hereditary diseases. If obvious skin and vascular signs are detected (skin hyperelasticity and spontaneous formation of bruises without signs of coagulopathy), it is legitimate to talk about Ehlers-Danlos syndrome. The question of differential diagnosis of benign HMS syndrome and the “mildest”, hypermobile type of Ehlers-Danlos syndrome remains open. This cannot be done using the Brighton criteria, which the authors specifically mention; in both cases there is moderate involvement of the skin and blood vessels. There is no known biochemical marker for either syndrome. The question remains open and will, apparently, be resolved only with the discovery of a specific biochemical or genetic marker for the described conditions.
Considering the widespread prevalence of constitutional HMS in the population, especially among young people, it would be erroneous to explain all joint problems in this category of people only by hypermobility. The presence of HMS does not at all exclude the possibility of them developing any other rheumatic disease, to which they are susceptible with the same probability as persons with a normal range of motion in the joints.
Thus, the diagnosis of HMS syndrome becomes justified when other rheumatic diseases are excluded, and the existing symptoms correspond to the clinical signs of the syndrome, logically supplemented by the identification of excessive joint mobility and/or other markers of generalized connective tissue involvement.
Treatment of HMS syndrome
Treatment of a patient with HMS syndrome depends on the specific situation. The variety of manifestations of the syndrome also requires a differentiated approach to each individual patient. An important point is to explain in an accessible form the causes of his joint problems (“weak ligaments”) and convince the patient that he does not have a serious illness that threatens inevitable disability. For moderate arthralgia this is sufficient. Recommendations to eliminate stress that causes pain and discomfort in the joints will be useful. Decisive in the treatment of severe pain are non-drug methods, and first of all, optimizing lifestyle. This involves matching the loads and the threshold of their tolerance for a given patient. It is necessary to minimize the possibility of injury, which includes vocational guidance and the exclusion of team sports.
For persistent pain in one or more joints, elastic orthoses (knee pads, etc.) are used. Timely correction of detected flat feet is very important. At the same time, the doctor is required to have basic podological knowledge - the shape and rigidity of the insoles is determined individually, and the success of the treatment largely depends on this. It is often possible to cope with persistent arthralgias of the knee joints using this only method.
In ensuring the stability of the joint, not only the ligaments play a significant role, but also the muscles surrounding the joint. If it is impossible to influence the condition of the ligamentous apparatus through exercises, then strengthening and increasing muscle strength is a real task. Gymnastics for GMS syndrome has a peculiarity - it includes so-called “isometric” exercises, during which significant muscle tension occurs, but the range of motion in the joints is minimal. Depending on the location of the pain syndrome, it is recommended to strengthen the muscles of the thighs (knee joints), shoulder girdle, back, etc. Swimming is useful.
Drug therapy is applicable as symptomatic treatment for arthralgia. Since the pain associated with GMS syndrome is mainly non-inflammatory in nature, it is often possible to see a complete lack of effect from the use of non-steroidal anti-inflammatory drugs.
In this case, greater results can be achieved by taking analgesics (paracetamol, tramadol). Intra-articular administration of corticosteroids in the absence of signs of synovitis is absolutely ineffective.
For periarticular lesions (tendinitis, enthesopathies, bursitis, tunnel syndromes), treatment tactics are practically no different from those in ordinary patients. In moderate cases, these are ointments with non-steroidal anti-inflammatory drugs in the form of applications or compresses; in more persistent cases, local administration of small doses of glucocorticosteroids that do not have a local degenerative effect (suspension of methylprednisolone crystals, betamethasone). It should be noted that the effectiveness of local corticosteroid therapy largely depends on the correctness of the topical diagnosis and the technique of performing the procedure itself.
Note!
HMS is a common rheumatic syndrome that is not prognostically dangerous, but causes serious diagnostic problems in practice. A patient with suspected HMS syndrome requires the physician to pay attention to subtle details during history taking and examination; knowledge and experience are required in the ability to determine to what extent the nature of the complaints corresponds to the unusual joint mobility being detected. Treatment of GMS syndrome also has its own specifics and differs from traditional therapy for other patients with joint diseases
What to tell the patient?
It is important to explain to the patient in an accessible form the cause of his joint problems (“weak ligaments”) and convince him that he does not have a serious illness that threatens inevitable disability. For moderate arthralgia this is sufficient. Recommendations to eliminate stress that causes pain and discomfort in the joints will be useful; Advise on minimizing the potential for injury, which includes appropriate vocational guidance and avoidance of team sports.
Criteria for joint hypermobility syndrome
Large criteria
- Beighton score of 4 or more (at the time of examination or in the past)
- Arthralgia for more than 3 months in four or more joints
Small criteria
- Beighton score 1-3 (for people over 50 years old)
- Arthralgia for less than 3 months in one to three joints or lumbodynia, spondylosis, spondylolysis, spondylolisthesis
- Dislocation/subluxation in more than one joint or repeated in one joint
- Periarticular lesions of more than two localizations (epicondylitis, tenosynovitis, bursitis)
- Marfanoid (tall, thin, arm span/height ratio > 1.03, upper/lower body segment ratio < 0.83, arachnodactyly)
- Abnormal skin: thinness, hyperextensibility, stretch marks, atrophic scars
- Eye signs: drooping eyelids or myopia or antimongoloid fold
- Varicose veins or hernias or uterine/rectal prolapse.
To diagnose FHMS, the presence of two major, one major and two minor or four minor criteria is required
Excluded: Marfan syndrome due to the absence of damage to the lenses and ascending aorta; osteogenesis imperfecta in the absence of multiple bone fractures and “blue” sclera
Physical education, but not any
Treating pain in joint hypermobility with non-steroidal anti-inflammatory drugs (NSAIDs), as is done, for example, with arthrosis, is pointless, since the pain in this case is not caused by inflammation, but by another reason. It is preferable to use analgesics, although drug treatment in this case is far from the main thing. For persistent pain, it is rational to use elastic orthoses (knee pads) and bandages.
The patient will also have to eliminate loads that cause pain and discomfort in the joints, especially for team sports. Jumping, gymnastics and wrestling are prohibited. But swimming is very useful - it harmoniously develops muscles, but most importantly, it does not overload the joints, since body weight is less in water.
Special exercise therapy (isometric gymnastics) is also necessary. Although, unfortunately, it cannot be used to remove excessive stretchability of the ligaments, it can strengthen the muscles surrounding the painful joint or area of the spine. A strong muscle frame will take over the function of the ligaments, helping to stabilize the joint. Depending on the area of the body that hurts, you should choose the distribution of the load: either strengthen the thigh muscles, or work on the muscles of the shoulder girdle, back, etc.
Yoga can help with hypermobility syndrome, namely: static fixations of the body shape (asanas), which improve blood circulation in the joint capsule and strengthen the connective tissue of the joint, eliminating its excessive looseness, but without limiting normal mobility.
If any orthopedic abnormalities are detected, the patient is prescribed special gymnastics, orthopedic insoles, and in advanced situations, surgical treatment.
If the pain is accompanied by inflammation in the periarticular tissues, ointments and gels with NSAIDs will be needed, as well as local or injection administration of drugs that suppress inflammation.
By the way
With the syndrome of “loose” joints, the issue of professional guidance arises especially acutely. Work associated with physical overexertion, long walking or long standing is dangerous for the patient. In these cases, the weak, stretched connective tissue part of the joint (ligaments, capsule) cannot withstand the load, and it “looses,” which contributes to the development of arthrosis. Despite the natural amazing flexibility, which seems to naturally push a person to practice choreography, you should categorically not become a dancer or ballerina with this syndrome - otherwise you may remain disabled.