Limiting the use of medications, antidepressants, alcohol, and nicotine can lead to the development of withdrawal syndrome. This condition is a natural reaction of the body to the cessation of various substances entering the body; it is accompanied in most cases by intense symptoms that a person cannot get rid of on his own.
Specialists at the Yusupov Hospital with many years of experience treat withdrawal symptoms. Highly qualified psychiatrists and narcologists explain to patients how drug withdrawal syndrome is characterized and select the most effective methods for eliminating symptoms for patients.
Causes of withdrawal syndrome
Medicines contain psychoactive substances, therefore, against the background of their long-term use, when stopping therapy, the patient may experience withdrawal symptoms. The action of these substances contributes to changes in the emotional background, psychological state, and functioning of the nervous system.
Various types of addictions also cause this effect. Thus, smokers may experience nicotine withdrawal syndrome, but its formation requires a long period of time. Signs of withdrawal may also occur with alcoholism, opiate addiction, and cocaine addiction.
PsyAndNeuro.ru
In 2021, the June 2021 issue of Lancet Psychiatry published the article “Gradual Withdrawal of SSRIs to Reduce Withdrawal Symptoms” under the Viewpoint section. Authors: Mark Horowitz, a researcher at University College London who is a systematic critic of modern psychiatry, and David Taylor, professor of psychopharmacology at King's College London. The article is devoted to the problem of stopping taking SSRIs.
SSRI withdrawal symptoms may resemble symptoms of the anxiety disorders or depression for which these drugs are prescribed. Withdrawal syndromes can be distinguished from relapse or recurrence by the speed of onset (days rather than weeks), the rapid response to restarting SSRIs (usually within hours, sometimes within days), and the presence of physical and psychological symptoms. which were not present in the initial state (including dizziness, nausea and “brain zaps”, see https://psyandneuro.ru/novosti/brain-zaps/).
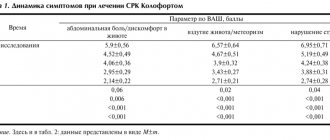
On average, according to 14 studies on SSRI withdrawal, withdrawal syndrome occurs in 53.6% of patients.
Sensory symptoms:
- Paresthesia
- Numbness
- “Brain zaps”
- Noise in ears
- Palinopsia
Somatic symptoms:
- Flu-like symptoms
- Drowsiness
- Headache
- Tremor
- Sweating
- Anorexia
- Weakness
- Tachycardia
Affective symptoms:
- Irritability
- Anxiety or agitation
- Low mood or depression
- Tearfulness
- Fears
Balance imbalance:
- Dizziness
- Loss of coordination
- Unsteadiness when walking
Sleep disorders:
- Insomnia
- Nightmares
- Unusually vivid dreams
Gastrointestinal symptoms:
- Nausea
- Vomit
- Diarrhea
- Anorexia
Sexual disorders:
- Genital hypersensitivity
- Premature ejaculation
Cognitive symptoms:
- Confusion
- Decreased concentration
- Amnesia
Clinical recommendations suggest that to prevent withdrawal symptoms, it is necessary to gradually reduce the dose of SSRIs without stopping the use at once. NIHS, British Association of Psychopharmacology, MIMS, UpToDate guidelines suggest a linear dose reduction over 2-4 weeks to the minimum therapeutic dose or to half the minimum therapeutic dose. Fluoxetine, according to these recommendations, can be discontinued immediately or, if taken in high doses, the dose can be reduced over 2 weeks.
Based on the results of 9 studies (1995-2018), it can be concluded that a two-week dose reduction period is insufficient to prevent withdrawal syndrome.
Gradually reducing the dose of SSRIs gives biological systems more time to adapt to the reduction in available ligands. Drug-activated receptors are often downregulated or the receptors exhibit decreased sensitivity. Abrupt withdrawal of the drug disrupts the homeostatic balance, leading to a decrease in stimulation, which manifests itself in the form of withdrawal symptoms, often opposite in nature to the effect of the drug. For example, withdrawal syndrome from tricyclic antidepressants, which produce a strong anticholinergic effect, is characterized by cholinergic effects. Drugs with shorter half-lives cause withdrawal symptoms with greater frequency, greater severity, and faster onset than drugs with longer half-lives, likely because their withdrawal is associated with a more rapid decrease in the number of available ligands. Resumption of the drug returns the system to homeostatic equilibrium.
The main approach to mitigating withdrawal is to reduce the rate at which this equilibrium is disrupted, allowing time for the system to adapt to the reduced level of ligands, thereby reducing withdrawal to an acceptable degree of severity. This can be achieved either by switching to a longer-acting drug before stopping treatment or by slowly reducing the dose of a drug with a short half-life.
Notably, decreasing the dose by a constant amount (linear decrease) causes more severe side effects over time. This is likely a consequence of the hyperbolic dose-response relationship between the drug and the receptor, which is typical of the effects of diazepam on the γ-aminobutyric acid (GABA-A) receptor. In this regard, recommendations for the withdrawal of benzodiazepines advise, as the dose is reduced, to reduce the amount by which the dose is reduced, according to the principle “the closer to zero, the slower we reduce.”
Benzodiazepines are recommended to be reduced in proportion to the current dose (usually by 10%), changing the dose exponentially rather than linearly. For example, reducing the dose of diazepam from 20 mg by 10% per week means that 2 mg less is taken for the first week, i.e. 18 mg. In the second week, the dose is reduced by 1.8 mg (10% of 18) to 16.2 mg, in the third week by 1.62 (10% of 16.2), etc. Thus, the total reduction in the third week will be 5.42 mg. Reducing the dose according to this exponential schedule produces a linear decrease in the effect on the receptor. The taper continues until the dose is well below the minimum therapeutic dose (which may seem quite minuscule) before stopping the drug completely.
Since withdrawal symptoms are thought to subside due to homeostatic adaptation to reduced drug levels, it is recommended to pause before reducing the dose. Because the exact timing of adaptation has not been studied, most recommendations for discontinuation are based on clinical experience; consensus suggests a period of 1–4 weeks between dose reductions.
SSRI withdrawal syndrome is explained by a relative lack of serotonin during the adaptation of serotonergic receptors. SSRIs reduce the density of serotonergic receptors in rats, and in humans, even short-term administration of SSRIs has been shown to reduce the sensitivity of serotonin receptors in the cerebral cortex. Reversing the effects that SSRIs have on other neurotransmitters, including norepinephrine, glutamate and GABA, also plays a role.
The role of serotonin in coordinating the functions of the sensory and autonomic nervous systems with motor activity explains some of the manifestations of SSRI withdrawal syndrome. Decreased serotonin receptor stimulation in the raphe nuclei is thought to play a role in dizziness, nausea, and somnolence during withdrawal.
Dysregulation of somatosensory functions can lead to paresthesia, while movement disorders (eg, dystonia) may be caused by altered dopaminergic function. Some aspects of SSRI withdrawal syndrome can be attributed to neuronal changes in tissues outside the brain, given that serotonergic receptors are present in the vasculature and intestine.
PET studies in which the ligand was bound to serotonin transporters showed that the dose-response curve between SSRIs and serotonin transporters followed the typical hyperbolic relationship resulting from the Law of Mass Action.
Therefore, it is likely that a linear dose reduction will cause a severe withdrawal syndrome, since the decrease in serotonin transporter inhibition will become more and more significant with each step. For example, reducing the dose of citalopram from 20 mg to 5 mg will result in a hyperbolically increasing attenuation of serotonin transporter inhibition: an absolute decrease in serotonin transporter inhibition by 3% with a reduction in dose from 20 mg to 15 mg, by 6% from 15 mg to 10 mg, by 13% – from 10 mg to 5 mg; by 58% – from 5 mg to 0 mg. Even a dose reduction from 2.5 mg to 0 mg would result in an absolute reduction of serotonin transporter inhibition of 42.9%, and a decrease from 1.25 mg to 0 mg would result in a 28% reduction (greater than a dose reduction from 40 mg). mg to 5 mg, leading to a decrease of 27.3%). These significant reductions in serotonin transporter inhibition may be responsible for the worsening withdrawal symptoms that patients experience toward the end of the withdrawal period.
To achieve a linear reduction in the pharmacological effect, it is necessary to reduce the dose hyperbolically. Rather than reducing the dose by a fixed amount, the dose should be reduced according to a fixed interval of change in biological effect. For example, to gradually reduce serotonin transporter occupancy by 10%, the citalopram dose reduction would be: 20 mg, 9.1 mg, 5.4 mg, 3.4 mg, 2.3 mg, 1.5 mg, 0 .8 mg, 0.4 mg, 0 mg.
We suggest that the appropriate withdrawal regimen for an individual patient can be determined by a trial of SSRI dose reduction resulting in a 10% reduction in serotonin transporter occupancy (or 5% as a precaution), followed by monitoring for withdrawal symptoms. A 10% reduction in serotonin transporter occupancy is suggested because it corresponds to a reduction in the therapeutic minimum dose of approximately 2-fold (eg, from 20 mg to 10 mg citalopram), which is well tolerated by most patients. If after a month the patient has no signs of withdrawal, then the dose can be reduced so that the serotonin transporter occupancy decreases by 10% each month.
The SSRI should be reduced so that the final step to zero is equal to or less than the amount by which the dose was reduced in the previous step. This is done when the dose corresponds to approximately 10 percent serotonin transporter occupancy. This is a very small dose - for example 0.4 mg of citalopram.
It is difficult to say what the optimal interval between dose reductions should be. The pharmacokinetics of all SSRIs, with the exception of fluoxetine, are such that their steady-state levels are achieved 5-14 days after dose reduction. It would be prudent to continue monitoring for delayed withdrawal effects for 4 weeks after tapering the SSRI dose.
The proposed model eliminates the uncertainty that arises when withdrawing SSRIs regarding the question of which strategy to use—micro-tapering or mini-tapering. A micro taper is a tiny reduction in your SSRI dose every day or week. A mini taper is a reduction in dose in larger increments and over longer intervals (several weeks). Mini-declines are associated with more severe withdrawal symptoms, which may last several weeks after discontinuation of the drug. With micro-reduction, there is a cumulative accumulation and overlay of side effects. Because of the nature of this process, it becomes difficult to determine which dose reduction triggered the onset of symptoms.
In the next issue of Lancet Psychiatry, letters to the editor were published reviewing the article “Gradual withdrawal of SSRIs to alleviate withdrawal symptoms.” The authors of the first note represent the University of Leicester (UK) and the Blomenburg Psychiatric Clinic (Germany). They pay attention to three points (Kronenberg G, Desai D, Anghelescu I. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2019 Jul; 6(7):560).
First, the role of the placebo effect in how a patient responds to treatment for mild to moderate depression is known. There must also be a nocebo effect associated with the expectation that the condition will worsen due to discontinuation of the SSRI.
Second, withdrawal symptoms should be distinguished from symptoms of illness (eg, relapse of depression or recurrent depression). To complicate the problem, SSRIs are often prescribed to patients whose symptoms differ from those of a depressive disorder. There is currently no evidence that SSRI withdrawal symptoms can last for months or years. This is at least doubtful. The APPG for Prescribed Drug Dependence study published in 2021, cited by the authors of the article “Grading out SSRIs to alleviate withdrawal symptoms,” only reports the results of an online survey of people who believe that they are experiencing withdrawal syndrome from psychotropic drugs.
Third, discontinuation of SSRIs may be warranted in many situations (eg, due to side effects, drug interactions, during pregnancy, before surgery). Additionally, antidepressants are often prescribed by general practitioners, making complex tapering schedules difficult to follow.
The second review was written by specialists from the University of Texas, Institute of Psychiatry, Psychology and Neuroscience, King's College London, University of Southampton, University of Oxford (Selvaraj S, Jauhar S, Baldwin DS, Cowen PJ, Goodwin G, Hayes JF, Nutt DJ, Veronese M, Young AH . Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2019 Jul;6(7):560-561)
The authors of the article “Gradual withdrawal of SSRIs to alleviate withdrawal symptoms” believe that the severity of withdrawal syndrome can be predicted based on the level of the substance in the blood and PET data. However, the article did not prove that there is a correlation between changes in the level of the substance in the blood and withdrawal symptoms. None of the PET studies known to us indicate a connection between serotonin transporter occupancy and response to treatment at therapeutic doses. Accordingly, it is even more difficult to prove a connection with withdrawal syndrome.
The hyperbolic curve, based on data on the serotonin transporter, dose and blood concentration (derived from studies of healthy volunteers and patients with minimal experience on antidepressants), has no relevance to people taking SSRIs for a long time or to those experiencing long-term withdrawal syndrome.
It is unclear how PET studies of GABA and diazepam dosage might influence the interpretation of data on serotonin and SSRIs, since the actions of GABA and serotonin are quite different from each other.
The incidence and severity of withdrawal syndrome remains a controversial issue. The problem is that symptoms vary markedly by drug, are less common in placebo-controlled studies, and in open-label, unblinded studies, symptoms tend to be particularly severe. Unfortunately, the authors of the article were uncritical of the information about the frequency of withdrawal symptoms.
We agree that the tapering plan should be individualized. But it is unlikely that practitioners will be helped by explaining withdrawal symptoms by theoretical neurobiological changes of dubious clinical significance.
The authors of the third commentary represent the University of Nijmegen (Netherlands), the Royal Dutch Pharmaceutical Association, the Dutch College of General Practitioners (Ruhe HG, Horikx A, van Avendonk MJP, Groeneweg BF, Woutersen-Koch H; Discontinuation of Antidepressants Taskforce. Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2021 Jul;6(7):561-562)
In the Netherlands, discussion of the problem addressed by the article prompted representatives of the Royal Dutch Pharmaceutical Association, the Dutch College of General Practitioners, the Dutch Psychiatric Association and the patient organization MIND to formulate recommendations for the withdrawal of SSRIs and SSRIs. Independently of the authors of the article “Gradual withdrawal of SSRIs to alleviate withdrawal symptoms,” but guided by the same ideas, we proposed a hyperbolic reduction in doses of SSRIs and SSRIs.
Steps to discontinue SSRIs and SSRIs in the presence of one or more risk factors for severe withdrawal syndrome (dose - mg/day)
| Citalopram | Escitalopram | Fluvoxamine | Paroxetine | Sertraline | Duloxetine | Venlafaxine | |
| Step 1 | 20 | 10 | 50 | 20 | 50 | 60 | 75 |
| Step 2 | 10 | 5 | 30 | 10 | 25 | 30 | 37,5 |
| Step 3 | 6 | 3 | 20 | 7 | 15 | 15 | 20 |
| Step 4 | 4 | 2 | 15 | 5 | 10 | 10 | 12 |
| Step 5 | 3 | 1,5 | 10 | 3 | 7,5 | 6 | 7 |
| Step 6 | 2 | 1 | 5 | 2 | 5 | 4 | 5 |
| Step 7 | 1 | 0,5 | 2,5 | 1 | 2,5 | 2 | 3 |
| Step 8 | 0,5 | 0,25 | 0 | 0,5 | 1,25 | 1 | 2 |
| Step 9 | 0 | 0 | 0 | 0 | 0 | 1 | |
| Step 10 | 0 |
Calculations are made based on a desired reduction in serotonin transporter occupancy of 10% at each stage, according to the Michaelis-Menten Equation. The time interval between steps should be determined depending on the patient's condition.
The optimal rate of withdrawal is unknown, and not all patients need to follow a hyperbolic dose reduction model. We identified three risk factors for antidepressant withdrawal syndrome:
- Dose above the minimum effective dose
- The appearance of withdrawal symptoms on days when the drug was interrupted for one reason or another
- History of unsuccessful attempts to stop taking SSRIs or SSRIs.
Tapering the dose in 1-month increments can be very effective, but at the same time it is a very conservative and very long-term regimen. In cases where a hyperbolic model is in demand, we suggest initially taking a step of 1 week, and then monitoring the patient’s condition. If severe symptoms appear, you should return to the dose at which there were no withdrawal symptoms and continue to slowly reduce the dose.
The section ends with a response from the authors of the article (Horowitz MA, Taylor D. Tapering of SSRI treatment to mitigate withdrawal symptoms – Authors' reply. Lancet Psychiatry. 2019 Jul;6(7):562-563)
The claim that changes in blood levels are not associated with withdrawal symptoms is unproven. The more sharply the concentration of an antidepressant with a short half-life in the blood decreases, the more severe the symptoms and the faster they appear. A 2000 study that did not find a correlation between withdrawal symptoms and changes in blood concentrations of specific antidepressants did, however, report that there was a statistically significant correlation across the drug group as a whole. Attenuation of the effects of antidepressants on brain receptors is likely a key factor in the onset of symptoms, and blood concentrations may not accurately reflect the extent of the drug's effects on the brain due to a number of individual pharmacokinetic differences.
Our critics argue that the hyperbolic relationship between dose and serotonin transporter occupancy does not persist over long-term treatment. We agree that neuroadaptation likely occurs with long-term antidepressant use. However, this does not abolish the Law of Mass Action; There will be a shift in the dose-response curve, but its hyperbolic shape will remain. The law of mass action is a fundamental pharmacological principle that explains the sharp increase in the effect of small doses of a drug, which levels off as the receptors become saturated.
As for the analogy with benzodiazepine withdrawal: The law of mass action applies to representatives of different species of creatures, to different classes of drugs, to different receptors. Therefore, we believe that dose reduction should be made according to receptor activity, as is done with benzodiazepines, rather than simply tapering the dose linearly.
There are few studies on withdrawal syndrome, so we have to work with potentially unrepresentative samples. At the same time, there is no need to exaggerate the uncertainty of ideas about the frequency and severity of withdrawal symptoms.
The nocebo effect may play a role in the development of withdrawal symptoms. But this syndrome is observed in double-blind studies, and the presence of certain symptoms, such as “brain zaps,” casts doubt on the significance of the nocebo effect.
Author of the translation: Filippov D.S.
Source: Horowitz MA, Taylor D Tapering of SSRI treatment to mitigate withdrawal symptoms. Lancet Psychiatry. 2019; 6: 538-546
Flenlepsin: withdrawal syndrome
Indications for the use of Flenlepsin are mental disorders, neurological disorders, alcohol withdrawal syndrome, and epilepsy. However, stopping use of the drug may cause withdrawal symptoms. Phenibut also contains psychoactive substances, so withdrawal syndrome is a common problem with which patients come to the Yusupov Hospital.
Psychiatrists at the Yusupov Hospital regularly study world experience in the field of addiction therapy, so they know how to treat withdrawal symptoms. At the Yusupov Hospital there is a comfortable hospital that allows patients to be kept away from an undesirable environment and to regularly monitor their condition and symptoms of withdrawal.
Clonazepam: withdrawal syndrome
Clonazepam is a drug that has a sedative effect, so it is used in the treatment of panic attacks, headaches, phobias, and anxiety. The duration of taking the drug should not exceed 2 weeks; most often, clonazepam is used once to improve mental state.
Patients who have been taking the drug for more than 2 months need professional help, as they may develop physical and psychological signs of addiction. Psychiatrists at the Yusupov Hospital collaborate with experienced narcologists and select methods for treating clonazepam withdrawal syndrome, taking into account the fact that its removal from the body takes a long period of time.
Diagnostics
To make an accurate diagnosis and identify the stage of the condition, consultation with a therapist, psychiatrist, narcologist and other specialized specialists is recommended. Diagnostic measures include:
- Anamnesis collection. For an accurate diagnosis, the doctor must find out the duration of alcohol intake, the main symptoms and complaints of the patient.
- Inspection. The neurologist must determine the integrity of reflexes and coordination of movements. The doctor assesses the condition of the skin, mucous membranes, sclera, and measures pulse and blood pressure.
- Laboratory research. The functioning of the body can be determined by general and biochemical analysis of blood and urine. To assess the condition of internal organs, liver and kidney tests, hormone tests, as well as ultrasound of the abdominal organs, thyroid gland and heart can be additionally prescribed.
Based on research data, alcohol withdrawal syndrome is diagnosed, the treatment of which depends on the stage and concomitant diseases.
Hashish withdrawal syndrome
Withdrawal syndrome after using hashish develops with its regular use and combination with alcohol. In the initial stages, a person experiences the following symptoms:
- depressive moods;
- aggression;
- lethargy and apathy;
- drowsiness and increased fatigue.
Morphine withdrawal syndrome has symptoms similar to those of hashish withdrawal. Patients who are in a state of depression or agitation cannot independently overcome the manifestations of withdrawal symptoms. Psychiatrists at the Yusupov Hospital help patients with these addictions overcome psychological dependence; professional narcologists carry out activities aimed at removing narcotic substances from the body.
Lyrics: withdrawal syndrome
Lyrica tablets are a severe psychotropic drug that are used to treat depression, anxiety and other conditions. When this drug enters the body, it causes mental and physical agitation. The development of drug dependence is one of the side effects of prolonged use of Lyrica.
Psychiatrists at the Yusupov Hospital are studying world experience in treating drug addiction, in particular the subject of research is beta blocker withdrawal syndrome. Specialists with academic degrees use exclusively world-class methods that are scientifically proven and have undergone clinical trials.
Prevention
A cup of strong coffee in the morning or a glass of good wine at dinner gives us a good mood, and without painkillers it is difficult to endure a serious illness. But if any meeting with friends becomes a reason for large-scale drinking, and taking medications becomes a habit, you need to seriously think about it.
The permissible amount of alcohol without harm to health is individual for each person. There is no consensus among doctors on this matter. Some believe that it is quite acceptable to drink a glass of vodka or a glass of wine several times a week, while others are convinced that even this amount of alcohol is the path to alcoholism.
Each person chooses his own path independently, and a conscious decision to completely give up alcohol and cigarettes evokes only respect. But if the question of the permissible amount of alcohol remains debatable, then there can be no dispute about drugs: there is only one preventive measure - never try.
Caffeine withdrawal syndrome
Caffeine and energy drinks can cause addiction, to get rid of which psychiatrists at the Yusupov Hospital carry out consistent work consisting of several stages:
- awareness of the problem and determination of the degree of dependence;
- assessment of the patient's physical condition;
- activities aimed at caffeine detoxification;
- developing a strategy for drinking drinks containing caffeine.
Programs developed individually for each patient at the Yusupov Hospital are aimed at restoring psychological and physical health. The tactics of interaction with a patient who has been diagnosed with amphetamine withdrawal syndrome will differ significantly from recovery from caffeine withdrawal. In addition, when treating patients with severe forms of addiction, work with the environment is carried out.
Smoking withdrawal syndrome
Prednisol withdrawal syndrome, the symptoms of which appear with long-term use of the drug, differs from the signs of nicotine withdrawal. This syndrome has various manifestations: allergic reactions, insomnia, headaches, constipation, increased blood pressure, increased appetite.
Some people cannot overcome the symptoms without the help of a specialist and use cigarettes to eliminate symptoms. Innovative techniques, in combination with traditional approaches to quitting smoking and relieving nicotine withdrawal syndrome, are used by psychiatrists at the Yusupov Hospital. The result of complex therapy is the patient’s complete cessation of smoking cigarettes.
Alcohol withdrawal
Abstinence from alcohol occurs in different ways. This depends largely on the stage of the disease. The second stage of alcoholism is characterized by excessive arousal in the psychological and physical areas. The patient's hands and eyelids often tremble; the skin of the face and neck takes on a red tint; perspiration appears; swelling appears; one feels weak.
The third stage of alcohol dependence has other withdrawal symptoms:
- pale skin with a bluish tint;
- the patient breaks out in a cold sweat;
- movements are difficult, sluggish, coordination is impaired.
In many cases, a person does not want to eat anything, he is tormented by vomiting and nausea, and a headache. Behavior becomes more aggressive.
Treatment of withdrawal syndrome in Moscow
The Yusupov Multidisciplinary Hospital is a modern medical institution that provides medical services to patients in accordance with international standards. Patients experiencing withdrawal symptoms from marijuana, medications, or alcohol may seek expert advice and treatment from mental health providers.
When treating patients, effective methods and drugs are used, when selecting which specialists take into account the characteristics of withdrawal symptoms. When visiting the Yusupov Hospital, patients receive professional advice and comprehensive therapy programs on the condition of anonymity.
Pre-registration for an appointment with a psychiatrist is carried out by employees of the Yusupov Hospital by telephone.
What causes these symptoms?
At first glance and by feeling, it seems that the body simply begins to act up, like an indignant teenager, and threatens to turn on a self-destruction program if it is not immediately given a cup of coffee, a cigarette or an antidepressant tablet (or maybe something more serious). But in fact, at the moment when you give up a substance or drug, many body systems experience enormous stress and learn to work again. They have to independently produce substances that they are accustomed to receiving from the outside.
Substances that cause physical addiction have analogues that the human body can produce itself: hormones and neurotransmitters.
Substances from the outside are called antagonists; they attach to the receptors used by hormones and mediators to transmit signals, and thus “deceive” the brain
Thus, nicotine is equivalent to acetylcholine (it is responsible for the contraction of muscle fibers), and euphoretics “ride” on the receptors of dopamine - responsible for the pleasure and reward system, and endorphin - which, in addition to pleasure, also increases the pain threshold.
Habituation and dependence arise at the moment when the brain evaluates and compares the energy costs of independently producing the desired mediator and receiving an antagonist from the outside. The body relies on constant supply of substances from the outside and, as a result, reduces its own production of mediators.