General information
The viral disease West Nile fever was first discovered in Uganda in 1937. Today it is widespread on many continents - many outbreaks are recorded in the USA, in the countries of the Mediterranean coast, and the modern form of the virus is also quite common in Indonesia, former CIS countries, in the south of Russia. The pathogen is most viable in tropical and subtropical climates. The disease is transmissible - transmitted by blood-sucking arthropods, in this case mosquitoes, ixodid and argasid ticks. It is seasonal: infection most often occurs from May to October - the period most favorable for the development of mosquitoes.
Virus distribution diagram
The disease is an acute zoonotic disease, also called West Nile encephalitis or duck fever . Distinctive signs are multiple inflammation of the lymph nodes ( polyadenitis ), serous inflammation of the meninges and skin rashes, and in rare cases, meningoencephalitis .
Treatment
Patients with neuroinvasive West Nile disease receive supportive care that often requires hospitalization, intravenous fluids, ventilatory support, and prevention of secondary infections. There is no vaccine for humans. Organizational measures are based on mandatory hospitalization of patients with suspected West Nile fever. The basis of therapy is pathogenetic measures, which are carried out syndromously. Intensive monitoring of parameters of cardiovascular activity (blood pressure, heart rate), external respiration (rhythm, respiratory rate, depth), renal function (hourly and daily diuresis), body temperature and other indicators. Also, pathogenetic therapy includes measures to eliminate cerebral edema, dysfunction of the cardiovascular system, and seizures; prevention and treatment of external respiration disorders.
Pathogenesis
The mechanism of infection after the virus enters the bloodstream occurs along the path of hematogenous dissemination. As a result of viremia, the pathogen is detected in brain tissue. A tropism was revealed not only for neurocytes and cardiomyocytes, but also for vascular endothelial cells.
In response to infection, a perivascular lymphoid infiltrate is formed in the body. Neurocytes undergo dystrophy and necrosis. As a result of vascular damage, edema and swelling of the brain, local and generalized manifestations of thrombohemorrhagic syndrome are aggravated.
The virus is capable of long-term persistence in the human body. After the disease, persistent post-infectious immunity and no repeated cases have been recorded.
Transmission of infection
Infection in humans most often occurs as a result of the bites of infected mosquitoes. Mosquitoes become infected by feeding on the blood of infected birds; the virus circulates in their blood for several days. The virus eventually enters the mosquito's salivary glands. During its subsequent feeding on blood (during mosquito bites), the virus can enter the body of people and animals, where it can multiply and lead to illness. The virus can also be transmitted through contact with other infected animals, their blood or other tissues. A very small proportion of human infections occur through organ transplants, blood transfusions and breastfeeding. One case of transplacental transmission of WNV (from mother to child) has been reported. To date, there are no documented cases of person-to-person transmission of WNV through non-hazardous contacts and no cases of transmission of WNV to healthcare workers when standard infection control precautions are followed.
Causes
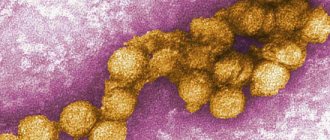
The cause of West Nile fever is the spread of an RNA-containing flavivirus, spherical in shape and only 20-30 nm in size.
West Nile virus model
The pathogen is able to survive in frosty and dry conditions; temperatures above 56 degrees Celsius are destructive; ether and deoxycholate are required for inactivation. The reservoir is birds and rodents.
Spreading
The first diagnosis of Nile fever was made in 1999 in Uganda. Until the early 70s, residents of equatorial Africa developed immunity and the virus spread to tropical regions. As a result of tourism, the disease spread to non-tropical regions and was introduced to the United States in 1999. Today, natural foci have been found in the Mediterranean countries, in Armenia, Azerbaijan, Moldova, in southern Ukraine, in the southern European part of Russia and other countries in this strip.
Map of the global spread of West Nile virus
In Russia, the first significant threat was in 1999, when West Nile fever in Volgograd affected more than 700 people, mainly affecting elderly people over 60 years of age, with 9 deaths.
By September 2021, more than 400 cases were registered, which is 2 times more than in previous years, and the disease occurred without symptoms of fever.
Natural foci most often form in suburban areas; they have been identified in the Astrakhan, Rostov, Voronezh, Lipetsk, Saratov and Volgograd regions, Krasnodar and Stavropol Territories, as well as in Tatarstan.
However, due to climate change, there is an increase in outbreaks of the disease. Thus, in Saratov, due to a decrease in the cold period, an increase in precipitation, and an increase in average temperatures, a favorable environment has been created for the development of foci and circulation of West Nile fever viruses. In the Saratov region, Rospotrebnadzor warns of danger and informs about preventive measures - the need to mow weeds, clean and drain basements, eliminate landfills, and install mosquito nets.
Vectors and host animals
The WNV virus is maintained in nature through a mosquito-bird-mosquito transmission cycle. The main carriers of WNV are mainly considered to be mosquitoes of the genus Culex, in particular Cx. Pipiens. WNV is maintained in mosquito populations through vertical transmission (from adults to eggs). Birds are reservoir hosts for WNV. Bird mortality associated with WNV infection is rare in Europe, Africa, the Middle East and Asia. Conversely, in America the virus is highly pathogenic for birds. The virus has been detected in dead and dying birds of more than 250 species, but birds from the crow family (Corvidae) are particularly susceptible. Birds can acquire infection in a variety of ways other than mosquito bites. Different bird species have different potential to maintain the transmission cycle. Horses, like people, are the “ultimate” owners. This means that when they acquire an infection, they do not spread it. Clinical infections in horses are also rare and are usually mild, but can lead to neurological disease, including fatal encephalomyelitis.
Virus circulation
West Nile virus has two main types of circulation:
• rural cycle (wild birds living in wetlands and ornithophilous mosquitoes, that is, feeding on the blood of birds); • urban cycle (synanthropic, ecologically associated with humans, bird species and mosquitoes that feed on the blood of birds and humans, mainly Culex pipiens/molestus). In Europe, there is a clear delineation of the disease with a predominance of a relatively small rural cycle (ornithophilous mosquitoes), since the majority of the population lives in cities and the urban lifestyle is clearly separated from the rural one, including in terms of living standards. And mosquitoes themselves are clearly differentiated in their preferences (either mammals or birds). In the United States, a significant part of the population actually lives in rural areas and most cities (especially one-story suburbs) have a pronounced “rural” character. At the same time, the differences in living standards between the city and the village are not so noticeable, and the subspecies of mosquitoes themselves are indiscriminate in their diet and choose both animals and birds. Therefore the disease is more common. Another factor is the more southern location of the main US territory compared to Europe. In North America, birds are also the main reservoir of the virus, especially the American crow and American robin, which are very common in suburban American gardens.
Symptoms of West Nile fever in humans
From the moment of infection to the appearance of the first symptoms, 3-21 days can pass - this is the duration of the incubation period. The disease in humans begins acutely with hyperthermia (body temperature remains 38-40°) and chills . The fever flares up and then subsides, and can last only 1-2 days, but more often 5-7. Its harbingers are often such short-term phenomena as:
- general weakness;
- lack of appetite;
- increased sweating ;
- myalgia (especially pain in the calf muscles);
- headache.
, serous meningitis occurs . As a result, patients develop a fragmentation of mild meningeal symptoms in the form of stiffness of the neck muscles, Kernig and Brudzinski symptoms, inflammatory changes in the cerebrospinal fluid - the development of pleocytosis , a slight increase in the amount of protein. Focal scattered microsymptoms from the nervous system develop, including horizontal nystagmus , palmomental symptom, diffuse decrease in muscle tone, deterioration of tendon and absence of abdominal reflexes.
Rare encephalitic manifestations are replaced by signs of mixed somato-cerebral asthenia ( sweating , insomnia , general weakness, mental depression, weakened memory are observed), which are caused by West Nile fever. Symptoms of intoxication are expressed as:
- severe painful headache, especially in the forehead and eyes, as well as pain in the neck and lower back;
- pain, discomfort and cardiac arrest;
- pain and swelling of the joints;
- hyperemia of the skin and in 5% of cases – maculopapular rash;
- repeated vomiting, lack of appetite, diarrhea and other dyspeptic disorders;
- hyperemia of the conjunctiva and uniform injection of the vessels of the eyeballs;
- hyperemia and granularity of the mucous membranes of the oral cavity;
- arterial hypotension;
- hepatolienal syndrome;
- polylymphadenitis – peripheral lymph nodes are enlarged, their sensitivity and slight pain;
- in rare cases, the nose becomes stuffy and a dry cough begins.
The clinic is accompanied by minor changes in laboratory parameters - an increase in ESR, slight leukocytosis .
Symptoms of West Nile fever in children often resemble tick-borne encephalitis . The disease is tolerated much more easily by children than by elderly people or people with weakened immune systems.
Publications in the media
Fever of unknown origin (FOU) is an increase in body temperature >38.3 °C for >3 weeks without identifying the cause after a 1-week intensive diagnostic search.
Etiology • Infectious diseases . Any infection can be accompanied by fever, but difficulties in diagnosis are often caused by sporadic, uncharacteristic or atypical diseases. Anamnesis, including epidemiological, is important.
•• Bacterial infections ••• Abdominal abscesses (subphrenic, retroperitoneal, pelvic), the likelihood of which increases with a history of trauma, surgery, gynecological or laparoscopic manipulations ••• Tuberculosis is one of the common causes of LNG. Diagnosis is difficult in cases of extrapulmonary tuberculosis with negative tuberculin tests. An important role in diagnosis is assigned to the search for lymph nodes and their biopsy ••• Infectious endocarditis is difficult to diagnose in cases of absence of heart murmurs or negative bacteriological blood cultures (usually due to previous antibiotic therapy) ••• Empyema of the gallbladder or cholangitis in elderly patients may occur without local symptoms of tension in the right upper quadrant of the abdomen ••• Osteomyelitis can be suspected in the presence of local tenderness in the bones, but radiographic changes may not be detected until several weeks later ••• Meningeal or, especially, gonococcal sepsis can be suspected by the presence of a characteristic rash; confirmed by bacteriological blood culture data ••• When identifying hospital-acquired LNG, the structure of hospital-acquired infections in a particular medical institution should be taken into account; the most common etiological agents are Pseudomonas aeruginosa and staphylococci.
•• Viral infections ••• Fever in AIDS is caused in 80% by concomitant infection, in 20% by lymphomas ••• Infection caused by the herpes virus, CMV, Epstein-Barr, is difficult to diagnose in the elderly (erased clinical manifestations); Serological confirmation of the presence of infection is important.
•• Fungal infections (candidiasis, fusarium, actinomycosis, histoplasmosis) are most likely in patients with AIDS and neutropenia.
•• Parasitic infections (malaria, toxoplasmosis, leishmaniasis) can be suspected in persons who have visited endemic areas.
• Neoplasms.
•• Hodgken and non-Hodgken lymphomas : diagnosis is difficult with retroperitoneal localization of lymph nodes •• Hemoblastoses •• Solid tumors (most typically with metastases to the liver or with tumor obstruction of the urinary tract).
• Systemic connective tissue diseases.
•• SLE: diagnosis is facilitated by the detection of ANAT •• Still's syndrome has no serological markers; is accompanied by the appearance of a salmon-colored rash at the height of fever (see Rheumatoid Arthritis) •• Among systemic vasculitis, the most common are polyarteritis nodosa and giant cell arteritis.
• Granulomatous diseases.
•• Sarcoidosis ( diagnosis is difficult with isolated liver damage or questionable changes in the lungs; liver biopsy or CT is important to clarify the condition of the bronchopulmonary lymph nodes) •• Crohn's disease is diagnostically difficult in the absence of diarrhea; endoscopy and biopsy data are important.
• Fever of medicinal origin (vaccines, antibiotics, various drugs): usually there are no skin manifestations of allergy or eosinophilia; drug withdrawal leads to normalization of body temperature within several days.
• Endocrine pathology.
•• Acute thyroiditis and thyrotoxicosis •• Adrenal insufficiency (rare) • Recurrent pulmonary embolism.
Pathogenesis. Exogenous pyrogens induce the production of cytokines (IL-1, IL-6, α-IFN, TNF-α). The effect of cytokines on the thermoregulatory centers of the hypothalamus leads to an increase in body temperature.
Classification • “Classical” variant of LNG (difficult to diagnose variants of diseases traditionally associated with fever) • Hospital LNG • LNG due to neutropenia • HIV-associated (mycobacteriosis, CMV infection, cryptococcosis, histoplasmosis).
Clinical picture • Increased body temperature • The type and nature of fever are usually not very informative • General symptoms accompanying increased body temperature are headache, general malaise, muscle pain. Diagnostic tactics • History •• In the history, not only current complaints are important, but also those that have already disappeared •• All previous diseases should be identified, including operations, injuries and mental disorders •• Details such as family history may also be significant , data on vaccination and medication, professional history, clarification of the travel route, information about the sexual partner, the presence of animals in the environment • Physical examination • At the very early stage of diagnosis, artificial causes of fever should be excluded (administration of pyrogens, manipulations with a thermometer) • Identification of the type of fever (intermittent, remitting, constant) allows one to suspect malaria by the characteristic periodicity of fever (on the 3rd or 4th day), but for other diseases it provides little information • Physical examination should be carried out carefully and regularly, focusing on the appearance or change in the nature of the rash , heart murmurs, lymph nodes, neurological manifestations, fundus symptoms.
Laboratory data • CBC •• Changes in leukocytes: leukocytosis (for purulent infections - shift of the leukocyte formula to the left, for viral infections - lymphocytosis), leukopenia and neutropenia (neutrophil content in peripheral blood <1.0109/l •• Anemia • • Thrombocytopenia or thrombocytosis •• Increased ESR. • OAM • It should be borne in mind that persistent leukocyturia with repeated negative results of bacteriological urine culture should alert you to renal tuberculosis. • Biochemical blood tests •• Increased concentration of CRP •• With an increase in the concentration of ALT, AST, it is necessary to conduct a targeted study for liver pathology •• Fibrinogen D-dimers - if PE is suspected. • Bacteriological blood culture. Several cultures of venous blood are carried out (no more than 6) for the presence of possible bacteremia or septicemia. • Bacteriological urine culture, if PE is suspected. renal tuberculosis - culture on media selective for mycobacteria • Bacteriological culture of sputum or stool - in the presence of appropriate clinical manifestations. • Bacterioscopy: examination of a “thick drop” of blood for Plasmodium malaria. • Immunological methods • Comprehensive examination of the patient for tuberculosis •• In anergic or acute infection, the tuberculin skin test is almost always negative (it should be repeated after 2 weeks). • Serological studies are carried out for infections caused by Epstein-Barr viruses, hepatitis, CMV, pathogens of syphilis, Lyme borreliosis, Q-fever, amoebiasis, coccidioidomycosis. Testing for HIV infection is mandatory! • Study of thyroid function in cases of suspected thyroiditis • Determination of RF and ANAT in cases of suspected systemic connective tissue diseases.
Instrumental data • X-ray of the chest, abdominal cavity, paranasal sinuses (according to clinical indications) • CT/MRI of the abdominal cavity and pelvis if an abscess or space-occupying lesion is suspected • Bone scanning with Tc99 in the early diagnosis of osteomyelitis has greater sensitivity than the x-ray method • Ultrasound of the abdominal cavity and pelvic organs (in combination with a biopsy if indicated) for suspected mass formation, obstructive kidney disease or pathology of the gallbladder and biliary tract • EchoCG for suspected heart valve damage, atrial myxoma, pericardial effusion • Colonoscopy for suspected disease Crohn's • ECG: possible signs of overload of the right heart with PE • Bone marrow puncture if hemoblastosis is suspected, to identify the causes of neutropenia • Liver biopsy if granulomatous hepatitis is suspected • Temporal artery biopsy if giant cell arteritis is suspected • Biopsy of lymph nodes, altered muscle areas and/or skin.
Features in children. The most common causes of LNG are infectious processes and systemic connective tissue diseases.
Features in the elderly. The most likely causes are cancer, infections (including tuberculosis), systemic connective tissue diseases (especially polymyalgia rheumatica and arteritis of the temporal artery). Signs and symptoms are less severe. Concomitant diseases and the use of various drugs can mask fever. The mortality rate is higher than in other age groups.
Features in pregnant women. An increase in body temperature increases the risk of developing neural tube defects in the fetus and causes premature birth.
TREATMENT General tactics • It is necessary to establish the cause of fever using all possible methods; until the cause is established, symptomatic treatment • Caution should be given against “empirical therapy” of GC, which can be harmful if the fever is infectious in nature. Mode. Hospitalization of the patient, limiting contacts until infectious pathology is excluded. Patients with neutropenia are placed in boxes. Diet • When body temperature rises, increase the amount of fluid consumed • Patients with neutropenia are prohibited from bringing flowers (source of Pseudomonas aeruginosa), bananas (source of Fusarium), lemons (source of Candida) into the ward.
Drug treatment Treatment is prescribed depending on the underlying disease. If the cause of fever is not established (in 20%), the following drugs can be prescribed. • Antipyretics: paracetamol or NSAIDs (indomethacin 150 mg/day or naproxen 0.4 g/day). • Tactics of empirical therapy for LNG due to neutropenia •• Stage I: start with penicillin, which has activity against Pseudomonas aeruginosa (azlocillin 2-4 g 3-4 times / day) in combination with gentamicin 1.5-2 mg/ kg every 8 hours or with ceftazidime 2 g IV every 8 or 12 hours •• Stage II: if fever persists, on the 3rd day an antibiotic acting on gram-positive flora is added (cefazolin 1 g IV every 6–8 h, if ceftazidime has not been previously prescribed) •• Stage III: if the fever persists for another 3 days, amphotericin B 0.7 mg/kg/day or flunicazole 200–400 mg/day IV should be added •• If the fever is eliminated, An effective antibiotic regimen is continued until the neutrophil count returns to normal.
Course and Prognosis • Depends on etiology and age • One-year survival rates are: 91% for those under 35 years of age, 82% for those aged 35–64 years and 67% for those over 64 years of age. Abbreviations. FNG is a fever of unknown origin.
ICD-10 • R50 Fever of unknown origin
Tests and diagnosis of West Nile fever
The reasons for suspecting West Nile fever are the characteristic clinical picture and epidemiological history.
Serological studies do not provide completely reliable results, since flaviviruses have a close antigenic relationship and the detection of antibodies in blood serum is due to the circulation of another type of virus.
Diagnosis is carried out by isolating MK-2 cells from cultures and intracerebral infection of mice. To identify West Nile virus, fluorescent antibodies and species-specific luminescent immunoglobulins are used.
Laboratory tests of cerebrospinal fluid reveal:
- lymphocytic pleocytosis 100-2000×106/l;
- slight increase in the amount of proteins.
Prevention
No specific vaccine has been developed for West Nile fevers. Nonspecific preventive measures boil down to preventing mosquito bites and ticks, as well as their early removal.
Health education should focus on reducing the risk of mosquito transmission. Efforts to prevent transmission should primarily focus on personal and community protection from mosquito bites through the use of mosquito nets and personal repellents, wearing light-colored clothing (long-sleeved shirts and trousers), and avoiding exposure to outdoors during peak mosquito bite times. In addition, programs should be implemented to encourage communities to eliminate mosquito breeding sites in residential areas.
Viral Roulette
The genetic stability of WNV, unprecedented for flaviviruses, allowed us to say that the entire modern world “population” of this virus is actually the offspring of a single clone that originated in the Mediterranean Sea region.
It is obvious that it was changes in the nucleotide sequence of the virus genome that determined its unusual ability to infect a large number of species of mosquitoes, birds and mammals. But since the total genetic differences of the new strain from the previous ones are too small (no more than 5%), it has not yet been possible to identify those critical mutations that predetermined the current distribution of the virus in the natural ecosystems of various continents.
The deaths of polar bears from WNV reported in Canada show that the virus's potential to expand into new ecosystems is far from exhausted. It is possible that it can even reach Antarctica with migratory birds.
As mentioned above, a person is sensitive to a new genovariant of the virus. Most of the human diseases are registered in the second half of summer and autumn. The incubation period after being bitten by an infected mosquito is 4-8 days. An illness that begins with an increase in temperature most often develops into fever of varying degrees of severity and duration. This form of the disease is very similar to the common flu and is often misdiagnosed.
Some patients develop viral encephalitis and meningoencephalitis - severe forms of the disease requiring hospitalization. The clinical picture in these cases is very similar to that of tick-borne encephalitis. The prognosis is also similar: mortality up to 10% or more. At the same time, children get sick much more easily, unlike older and elderly people.
There is an assumption that low sensitivity to West Nile virus and other flaviviruses, such as tick-borne encephalitis virus, is genetically determined in humans. However, genes that provide such resistance have not yet been discovered
But infection does not necessarily end in disease: as a rule, out of ten infected people, 8-9 people do not develop the disease or are asymptomatic. Although these people are not at risk to their health, they may pose a danger to others if they donate blood or if their organs are used for transplantation. Fatalities following blood transfusions or organ transplants have prompted the US government to mandate WNV testing for blood products and organ donations.