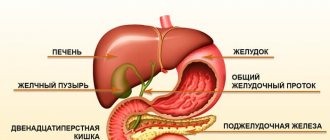
How does a lack of potassium manifest itself in the body?
Potassium is one of the elements necessary for the body. Its main carrier is water, and since the body is composed primarily of water, it is obvious that potassium must be everywhere. It performs many functions in the body. Stimulates insulin secretion, promotes the burning of proteins and carbohydrates. He is very needed. Its deficiency can be very unfavorable for the body, so it is worth knowing how to recognize this condition and, of course, how to counteract it. Be sure to read the helpful tips in this article.
Symptoms
Symptoms of potassium deficiency can vary. Pay special attention to your stomach. If it fails and flattens, then this is the effect of the so-called “frog belly”. This may be due to weakness of the abdominal muscles, as well as the stomach and intestines. This disease is also accompanied by problems with metabolism and constipation. You should be aware that high blood pressure can also be a sign of hypokalemia, but not only that. If you are suffering from swollen legs and arms, you need to get tested and take some action to replenish the potassium deficiency, if any. If you find that your heart is beating irregularly, it's time to see a doctor and have your blood potassium levels checked. I'm not kidding.
Hypokalemia
Hypokalemia develops due to
- reducing potassium intake from food,
- its movement into cells or
- enhanced excretion.
A decrease in potassium intake is rarely the only cause of hypokalemia, since due to reabsorption in the distal nephron, urinary potassium excretion can decrease to 15 mmol/day; the amount of potassium entering the body with food in most cases exceeds this value. The exceptions are citizens with a low standard of living and people on special diets.
However, insufficient potassium intake may aggravate hypokalemia caused by potassium losses through the gastrointestinal tract or kidneys.
One of the rare causes of hypokalemia is eating clay (geophagy), since it binds potassium and iron ions. Geophagy was formerly widespread among blacks in the southern United States.
The movement of potassium into cells reduces plasma potassium concentrations temporarily without affecting total body potassium levels. Regardless of the reason for the movement of potassium into cells, the change in its concentration is normally relatively small - no more than 1 mmol/l. However, like insufficient dietary potassium intake, potassium translocation into cells may exacerbate hypokalemia due to potassium wasting.
Hypokalemia is caused by metabolic alkalosis (due to potassium redistribution and losses through the kidneys and gastrointestinal tract), hyperglycemia (due to osmotic diuresis), administration of large doses of insulin during diabetic ketoacidosis (as a result of stimulation of Na+/H+ countertransport and mediated activation of Na+,K±ATPase), increased levels of catecholamines, the appointment of beta2-agonists (due to the movement of potassium into the cells and increased insulin secretion), the growth of new cells (for example, when prescribing vitamin B12 for Addison-Beermer disease or GM-CSF for neutropenia), transfusion of thawed and washed red blood cells (since frozen red blood cells lose up to half of their potassium during storage).
Hypokalemia is also seen in familial hypokalemic periodic paralysis, a rare condition that causes attacks of muscle weakness or paralysis.
Sweating leads to hypokalemia, both directly and through hypovolemia-induced increases in aldosterone and potassium excretion.
Normally, with a stool volume of 100-200 ml, potassium loss with it is 5-10 mmol/day.
Hypokalemia due to potassium loss through the gastrointestinal tract occurs with villous polyp, VIPoma, diarrhea (usually secretory) and laxative abuse. Loss of gastric contents during vomiting and aspiration through a nasogastric tube are not in themselves the causes of hypokalemia (the potassium concentration in gastric juice is 5-10 mmol/l, and for a deficiency of 300-400 mmol, which is usually observed in such patients, it would be required volume losses of 30-80 l). In such cases, hypovolemia and metabolic alkalosis lead to hypokalemia. Hypovolemia stimulates aldosterone secretion, and metabolic alkalosis leads to bicarbonaturia and increased negative fluid charge in the collecting ducts (filtered bicarbonate cannot be completely reabsorbed in the proximal tubules). Both of these mechanisms increase urinary potassium excretion.
How to find out which microelements are missing in the body? / "www.inthecity.ru"
Return to list
When choosing a vitamin-mineral complex at the pharmacy, we first of all pay attention to how much vitamins C, B and E it contains as a percentage of the daily value. We usually ignore the inscription informing about the content of zinc, magnesium, selenium and phosphorus in the preparation. Yes, we know that it is good for the body. But who wants to remember school chemistry?
Meanwhile, there are 86 microelements in the human body. Some of them are called structural, since they make up 99% of the elemental composition of the human body. These include: carbon, oxygen, hydrogen, nitrogen, calcium, magnesium, sodium, potassium, chlorine, phosphorus, sulfur, iron. The growth, development and health of the body directly depend on the amount of minerals: they affect hematopoiesis, bone formation, absorption processes in the intestines, are responsible for the acid-base balance, perform the function of nerve conduction, intracellular respiration and much more.
Unfortunately, living in the city, we receive not only useful microelements. Our health is at risk from the accumulation of heavy metals that cause intoxication, or, more simply, poisoning. Symptoms of the accumulation of mercury, lead, arsenic, cadmium, nickel are weakness, sleep and appetite disturbances, irritability, dull skin and hair, broken nails and, of course, memory deterioration, concentration decreases, and vision deteriorates. Tatyana Semenchenya, a doctor at the independent INVITRO laboratory, talks about the role of each element in the human body.
Copper
The largest amounts of copper are found in the liver, kidneys, heart and brain. And this microelement is excreted mainly with bile. Copper poisoning when it is contained in excess in water or food products and enters the body in large quantities is accompanied by nausea, vomiting, diarrhea, which can lead to the development of hemolytic anemia, renal and liver failure, and neurological disorders. Copper deficiency can lead to anemia and, in premature babies, to delayed psychomotor development.
Selenium
The role of selenium is not yet fully understood, however, it is believed that selenium has an antioxidant effect on the body, slowing down aging. Stimulates the production of collagen in the skin to maintain elasticity and helps eliminate dandruff.
In combination with vitamin E, selenium participates in the processes of reproduction, development of a young body and in a certain way affects life expectancy. When it is deficient, arsenic and cadmium accumulate in the body and calcium levels decrease. Selenium supports the functioning of the immune system. It can also reduce the likelihood of developing cancer.
Zinc
Foods that contain zinc are cereal grains, legumes, cocoa, seafood, mushrooms, onions, potatoes, and cow's milk. Zinc affects the hormonal levels of the body, is responsible for puberty, and affects fat, protein and carbohydrate metabolism. It is believed that zinc has a lipotropic effect, that is, it is able to break down fat cells.
It is also necessary to remember about a possible excess of this substance in the body, which can lead to growth retardation. A lack of zinc contributes to overexcitation of the nervous system, rapid fatigue, hair loss, and threatens infertility.
Iodine
A unique substance that is part of all plants. Iodine deficiency can lead to serious diseases - and this is not only thyroid disease, as is commonly believed, but also the development of mental retardation - cretinism - precisely in childhood! If there is a lack of iodine, the child stops growing and the entire structure of the body changes.
Excess iodine is characterized by sweating, irritability, tachycardia (rapid heartbeat), a person loses weight, a tendency to diarrhea, and exophthalmos (bulging eyes). This trace element is found in kelp (brown seaweed), onions, all seafood, as well as in vegetables grown in soil rich in iodine.
Potassium
Potassium is necessary for the human body for mental clarity, concentration, and also for getting rid of toxins. The main symptoms of potassium deficiency are delayed puberty, slow growth; with severe potassium deficiency, convulsions and cardiac dysfunction are possible. Potassium is found in tomatoes, bananas, potatoes, sunflower seeds, and citrus fruits.
Calcium
With a lack of calcium, tachycardia, arrhythmia (heart rhythm disturbance), muscle pain, constipation, whitening of fingers and toes, increased irritability, dullness, memory loss, decreased vision, broken nails, and hair loss are observed. Excess calcium is accompanied by muscle weakness, difficulty coordinating movements, bone deformation, nausea, vomiting, and frequent urination. Also, excess calcium can lead to a deficiency of zinc and phosphorus.
Calcium is contained in both plant and animal foods in the form of insoluble salts; their absorption into the intestines practically does not occur. Calcium metabolism is regulated by the parathyroid glands.
Magnesium
Magnesium is an essential component of all cells and tissues, including brain tissue. Participates in the process of neuromuscular excitability and is part of enzymes. Enters the body with water, food and salt. Found in large quantities in plant foods - almonds, dark green vegetables, bananas, nuts, figs.
With magnesium deficiency, symptoms of nervous system excitation, including seizures, are observed. A decrease in magnesium concentration leads to excess calcium and phosphorus deficiency. Phosphorus
Phosphorus plays an important role in all processes of our body and is involved in the construction of numerous enzymes responsible for cell life. And its salts make up the tissue of our skeleton.
With phosphorus deficiency, changes in bone and muscle tissue, memory loss, fatigue, and irritability are noted. With an excess of phosphorus, acute poisoning occurs, abdominal pain, vomiting are observed; an excess of this element can lead to death.
What to do?
If a person does not suffer from chronic diseases, monitors his diet, plays sports, spends enough time outside the city, in the fresh air, the likelihood of an acute shortage of any vitamins and minerals is small.
If any problems arise (even if it is “just” increased fatigue, irritability, sleep disturbances) or when planning large loads on the body (for example, pregnancy), it would be useful to undergo an analysis to determine microelements in the blood. Using this analysis, you can assess the state of the body in terms of resistance to chronic, endocrinological diseases, stress, and determine the deficiency of certain substances in the body.
It is recommended to do this analysis:
- children and rapidly growing teenagers
- To old people
- those planning pregnancy, pregnant women and nursing mothers
- people with chronic diseases, diseases of the endocrine system, suffering from intestinal dysbiosis, and those who often catch colds
- girls who are passionate about diets
- workaholics who work 24 hours a day
- living in unfavorable ecological zones
Where to get tested
Network of laboratories "INVITRO"
Analysis can be done on blood, hair and nails.
Examination “ME Profile 1” (main vital microelements: selenium, copper, zinc) - 990 rub. Adding other microelements - 200 rub. for every.
The analysis period is up to 6 working days.
Magnesium deficiency and heart rhythm disturbances
Magnesium controls the spontaneous electrical activity of the cardiac conduction system, ensuring normal functioning of the cardiomyocyte at the subcellular level. That is why the microelement plays a universal role in cardioprotection. Magnesium also takes part in the synthesis of lipids, proteins, nucleic acids, and ATP. The trace element is necessary for many energy and reparative processes, as well as normal electrolyte metabolism. Magnesium promotes relaxation of muscle fibers, maintains the necessary transmembrane potential in electrically excitable tissues, and reduces the aggregation ability of platelets. In autonomic cardiopathy, microelement deficiency may be indicated by long QT interval syndrome, paroxysms of ventricular tachycardia (torsades de pointes type), episodes of syncope, and acute cardiac arrest. The following signs can be seen on the ECG:
- prolongation of the QT interval;
- widening of the QRS complex;
- nonspecific decrease in the ST segment;
- slowing of AV conduction;
- pronounced U wave.
Risk factors for drug-induced hypokalemia
According to a study by E. Ramírez et al. [16], the only statistically significant (p<0.0001) predictor of the development of drug-induced hypokalemia is the simultaneous use of more than 5 drugs (polypharmacy), while the trigger for its development is hypoalbuminemia. Long-term use of certain drugs and their use in high doses is also associated with an increased risk of developing drug-induced hypokalemia [9, 20]. It can also be assumed that the risk of developing this pathological condition increases if the patient has diseases/conditions accompanied by hypokalemia (for example, Cushing's syndrome, gastrointestinal infections or tumors, malabsorption, hyperaldosteronism, hyperthyroidism, hypomagnesemia, renal tubular acidosis, etc.) [23] .
Treatment
To identify a lack of potassium and magnesium, you should not take into account only external signs. Doctors recommend blood and urine tests, an electrocardiogram, and a study of the mineral composition of hair and nails. After the deficiency of elements is confirmed, the doctor prescribes therapy to replenish them: vitamin preparations, IVs, injections or a special diet.
If there is a slight lack of minerals, drinking freshly squeezed juices will help replenish their amount. Substances in drinks are considered good catalysts and allow better absorption of food. Also, the diet should contain a lot of greens, vegetables, and fruits.
To replenish magnesium, eat nuts (hazelnuts, almonds, cashews and peanuts), wheat bran, buckwheat porridge, millet and wheat. Dried fruits are especially rich in minerals. For good health and replenishment of elements, regularly include dates, dried apricots, raisins, prunes, and dried coconuts in your menu.
All varieties of cabbage, fruits (apples, avocados, peaches, cherries and gooseberries), mint, sunflower seeds and various types of nuts are good for eliminating potassium deficiency. Do not neglect dairy and fermented milk products. There is especially a lot of potassium in fatty cheeses, sour cream, and fermented baked milk.
During heat treatment, products lose most of their nutrients. Therefore, try to include as much fresh food in your diet as possible. It is not recommended to soak potatoes and other vegetables in water before cooking. They need to be cut immediately before use: storing them in chopped form significantly reduces the number of useful elements.
To replenish minerals using pharmacological agents, you should not purchase them without consulting your doctor. An experienced medical specialist will recommend a suitable remedy, prescribe a dose and course duration. If there is a lack of magnesium, Magnesium Diasporal, Magne B6 Forte, Magnelis B6 and others are usually prescribed. Popular drugs containing potassium are Asparkam, Panangin, Potassium orotate and others.
Causes of deficiency
Most often, the lack of elements is caused by the reasons presented below.
- Improper and unbalanced nutrition.
- Long-term gastrointestinal disorders accompanied by vomiting and diarrhea.
- Abuse of laxatives or diuretics.
- Long-term use of glucocorticosteroid hormonal drugs, for example, Dexamethasone, Methylprednisolone or Hydrocortisone.
- High activity of the adrenal cortex and increased sweating.
- Staying under stress for a long time.
Mineral leaching occurs due to consumption of large amounts of coffee, alcohol or sweets.
Magnesium and potassium deficiency in the body: symptoms and signs
Home first aid kit MIRRA
In recent years, the Company has actively conducted research on the possibility of using health and cosmetic products to solve general and cosmetic problems. Almost all the leading employees of the Company worked in this direction - I. Rudakov (Dr. Sc.), S. Chubatova (Dr. Sc.), E. Aitova (Ph.D.), L. Conde ( Ph.D.), A. Golubkov (Ph.D.), Production Director V. Tulsky, Chief Technologist B. Gorodnichev. Also, consultants and distributors of some DCs began to take part in scientific developments. Since 2010, numerous scientific articles, how-to guides and product references have been published, addressing a range of modern cosmetology (cosmeceutical) concepts and the need for new product development, as well as the idea that beauty and health products need to be used in combination. The result of the scientific and practical work was the development of an information testing method for assessing the micronutrient supply (MS) of the body. This information was published in the issues of our monthly under the heading “Home First Aid Kit MIRRA”.
This publication is about potassium and magnesium deficiency.
POTASSIUM
(K)
Potassium is found in many foods and is 90-95% absorbable. On average, it enters the body with food in an amount of 1−3 g per day. A total of 160−180 g of potassium is present in the human body. Below is a questionnaire containing a list of negative states (NS). Their cause may be potassium deficiency, or rather, insufficient micronutrient supply. To understand whether there is a deficiency of potassium in the body, you need to identify the NS characteristic of your health condition and, depending on their quantity, estimate the potassium MO.
- Apathy, indifference to what is happening around.
- Tendency to depression.
- Decreased performance.
- Fatigue, frequent weakness.
- Decreased resistance to stress.
- Allergic reactions and diseases.
- Muscle weakness.
- Skin itching.
- The skin slowly recovers from cuts and wounds.
- Excessive dry skin.
- Excessive peeling and roughness of the skin.
- Severe hair loss.
- Loss of hair flexibility.
- Hair has become thinner.
- Hair dulling.
- The mucous membranes of the mouth and tongue are inflamed.
- Tendency to diarrhea.
- Heart rhythm disturbances, heart pain.
- Change in blood pressure.
- Tendency to inflammatory processes with the formation of erosion (gastritis, cervical erosion).
The results obtained allow us to judge the degree of potassium supply in the body. If NS is 6 or less, this indicates a normal level of MO. When choosing 7−12 NS, we can talk about a slight or moderate decrease in MO. Potassium deficiency in the body may be indicated by NS levels of 13 or more.
The reason for the decrease in the body's supply of potassium may be its insufficient intake from food. However, this is not the only explanation. Thus, the body intensively consumes potassium during nervous, mental overload, excessive or chronic stress.
Another important reason for the decrease in potassium MO is its displacement by excess sodium entering the body, taking hormonal drugs, diuretics, and laxatives. Potassium is consumed faster when the excretory systems (skin, intestines, lungs, kidneys) are disrupted.
Thus, if a potassium deficiency is detected, i.e., a decrease in MO, it is necessary to reconsider the diet. By adding potassium-rich foods to it, MO can be restored. The rapid restoration of potassium levels can be facilitated by over-the-counter drugs containing this micronutrient in the form of aspartate, which is well absorbed by the body (Panangin, Asparkam). They also contain magnesium aspartate. If the body is exposed to various stress factors for a long time, MO may be disrupted not only by potassium, but also by other substances, which requires the selection of a group of means to restore it.
If there is a pathology of the excretory systems, drug treatment is often prescribed. If potassium metabolism processes are disrupted at the organismal level, regulatory therapy with homeopathic remedies may be recommended. If potassium MO is normal, no interventions should be performed. If MO is reduced, its normalization becomes extremely important, and sometimes even vital for the body.
MAGNESIUM
(Mg)
On average, 200−400 mg of magnesium enters the body with food and water per day, and about half of this dose is absorbed in the gastrointestinal tract. This microelement is an important component of every cell, where, together with calcium and sodium, it participates in ensuring the most important intracellular processes.
Below is a list of negative conditions (discomfort, symptoms, diseases) that often indicate magnesium deficiency, or its insufficient MO. This condition may require correction by normalizing the diet and taking dietary supplements. Count the number of NS characteristic of your health condition.
- Increased nervous excitability.
- Dizziness.
- Anxiety, restlessness.
- Sleep disorders, insomnia.
- Tendency to depression.
- Increased fatigue, weakness.
- Decreased performance.
- Deterioration in concentration.
- Decreased resistance to stress.
- Hearing loss.
- Immunodeficiency states.
- Hair loss.
- Thin and brittle nails.
- Tingling and numbness in fingers and toes.
- Twitching of eyelids.
- Cramps and muscle pain.
- Fluctuations in blood pressure.
- Heart rhythm disturbances.
- Heartache.
- Tendency to diarrhea or constipation.
If the number of selected NS does not exceed 6, we can talk about a conditionally normal level of MO. The likelihood of a slight or moderate decrease in MO is indicated by the choice of 7−12 NS. A sign of magnesium deficiency may be the release of 13 NS or more.
In addition to those indicated in the list of NS, symptoms of magnesium deficiency (i.e., insufficient MO) may include unexplained headaches, increased irritability and tearfulness, and the appearance of absurd character. Of the entire complex of NS, restlessness, anxiety, and decreased perseverance are very often observed. The state of magnesium deficiency in the body and the disruption of its metabolism are greatly influenced by chronic stress.
These factors are not the only ones that can influence magnesium deficiency. To their number you can also add inflammatory processes or dysbiosis of the gastrointestinal tract, due to which the absorption of nutrients is impaired. Impaired magnesium metabolism can result from taking certain medications. An increased need for magnesium is observed during pregnancy or recovery after a long illness. At the same time, it is necessary to exclude the possibility of magnesium deficiency due to a monotonous diet, in which foods poor in this microelement predominate.
To eliminate the nervous system associated with magnesium deficiency, it is often enough to normalize the diet. MO can also restore the intake of magnesium-containing over-the-counter medications and dietary supplements. They may contain magnesium and potassium in the form of aspartates (Asparkam, Panangin), or magnesium and vitamin B6, as well as other mineral and vitamin complexes. Normal supply of the body with magnesium does not require taking any measures, but if it is insufficient, normalization of this condition is not only desirable, but often necessary.
I. Rudakov, Doctor of Medical Sciences, Director of Science
*When using article materials, a hyperlink to the source is required.
The role of minerals
Magnesium is a mineral responsible for the delivery of calcium and sodium ions to cells. It controls the condition of the cell membrane. Participates in strengthening and expanding the walls of blood vessels, normalizes the functioning of the heart. Thanks to magnesium, the functioning of the nervous system is normalized, tension goes away, and resistance to stress increases. The mineral takes an active part in hydrolysis, improves intestinal motility, and promotes the removal of waste and toxins from the body.
A lack of magnesium increases the risk of developing kidney and bladder stones. Deficiency of the element leads to rapid destruction of joints and bones. They become soft and porous. Often, magnesium deficiency causes a heart attack.
The main role of potassium is participation in water-salt balance. It delivers water to cells and removes excess water. Affects muscle function and increases resistance to physical stress. Potassium normalizes heart rhythm and has a beneficial effect on the condition of the myocardium. It provides oxygen to the brain and increases mental activity.
Lack of potassium leads to pathologies of the kidneys, liver, and disrupts the activity of the endocrine glands. Lack of the mineral causes the development of sclerosis and the accumulation of sodium in the vessels. This in turn provokes allergic reactions.
The daily intake of magnesium for an adult is 280–320 mg, potassium – from 200 to 500 mg. For pregnant women and athletes, the mineral content should be increased by 50–100 mg.
Potassium deficiency and heart rhythm disturbances
Potassium is required for the proper functioning of a wide range of intracellular enzymes. The trace element helps maintain normal acid-base and osmotic homeostasis, participates in the synthesis of glycogen, protein, central nervous system mediators, etc. With potassium deficiency, the cardiovascular system most often suffers. Against the background of microelement deficiency, autonomic cardioneuropathy may develop. The pathology is accompanied by complex rhythm disturbances, including atrial fibrillation. In some cases, it leads to death - sudden cardiac death. A lack of potassium can also aggravate the course of hypertension and increase the risk of developing a cerebral stroke. With a deficiency of this microelement, a pathological U wave, a smoothed T scar, and multifocal extrasystoles are usually recorded on the patient’s electrocardiogram.
Electrolyte imbalance and its role in the development of cardiovascular diseases
The article discusses the role of magnesium and potassium deficiency in the development of cardiovascular diseases and their complications. Risk factors for the development and symptoms of potassium and magnesium deficiency are described. The results of studies on the effectiveness of magnesium and potassium preparations used in cardiological practice are presented. The importance of potassium and magnesium preparations in preventing the progression of atherosclerosis, arterial hypertension, endothelial dysfunction, and disorders of carbohydrate and lipid metabolism has been shown. The advantages of magnesium and potassium aspartate preparations in order to eliminate the deficiency of these cations have been demonstrated.
Table 1. Foods high in magnesium and potassium
Table 2. Symptoms of potassium and magnesium deficiency
SHEP study: relative risk of cardiovascular events during treatment with chlorthalidone depending on plasma potassium levels (relative risk of cardiovascular events in the placebo group is set to 1)
Table 3. Positive effect on the prognosis of additional daily magnesium intake in patients at high cardiovascular risk in the PREDIMED study
Introduction
In recent years, a special role in the development and progression of cardiovascular diseases (CVD) has been assigned to electrolyte imbalances, in particular the balance of magnesium and potassium [1, 2]. Potassium is the main intracellular cation. Normally, the cell contains 150–160 mmol/l of potassium, and the blood plasma contains 3.5–5.5 mmol/l. Potassium is involved in the bioelectrical activity of cells, the formation of cellular action potentials and the maintenance of neuromuscular excitability and conductivity. The second most important intracellular cation is magnesium. Magnesium is a universal regulator of biochemical and physiological processes in the body, a cofactor for over 300 enzymes involved in biochemical reactions. Magnesium ensures the hydrolysis of adenosine triphosphate (ATP), reduces the separation of oxidation and phosphorylation, regulates the polarization of cell membranes, controls the spontaneous electrical activity of nervous tissue and the conduction system of the heart, the normal functioning of the cardiomyocyte, and is involved in the metabolism of carbohydrates, lipids, nucleic acids and proteins. Magnesium is a natural physiological calcium antagonist. It reduces the release of calcium from the sarcoplasmic reticulum and protects cells from calcium overload under ischemic conditions, reduces platelet aggregation ability, and maintains normal transmembrane potential in electrically excitable tissues [3, 4]. Mg2+ deficiency is associated with increased levels of total cholesterol, low-density lipoproteins, triglycerides, decreased activity of lecithin-cholesterol aminotransferase and lipoprotein lipase, and increased activity of HMG-CoA reductase. Magnesium has an antiatherogenic effect [5, 6]. Data have emerged on the decisive role of magnesium in the synthesis and metabolism of vitamin D, the deficiency of which is considered an independent risk factor for the development of CVD [7].
Potassium enters the body with food, magnesium - with food and water, excess potassium and magnesium is excreted in the urine. The daily requirement for potassium is 2500 mg. The magnesium requirement of an adult is 300–400 mg/day (increases during the period of growth, as well as in persons engaged in physical labor, athletes, and pregnant women). Potassium is found in bananas, potatoes, dried fruits, apricots, spinach, broccoli, and legumes. Dried apricots, prunes, nuts, dark chocolate, and seaweed are characterized by a high content of potassium and magnesium (Table 1). However, digestibility from food products does not exceed 30–35%.
Hypokalemia is a persistent decrease in serum potassium concentration less than 3.5 mmol/l, hypomagnesemia is a decrease in serum magnesium concentration less than 0.8 mmol/l. The normal intracellular potassium content is 150–160 mmol/l, magnesium – 1.65–2.55 mmol/l. It should be taken into account that with normal levels of potassium and magnesium in the blood serum, an intracellular deficiency of these cations may occur.
In many regions, the concentration of magnesium in drinking water and soil, as well as in plant foods grown in these regions, is low. Daily magnesium intake is significantly lower than recommended.
In industrialized countries, the number of people with magnesium deficiency is increasing [7, 8]. In the United States, almost 75% of the population has a magnesium deficiency or its level corresponds to the lower limit of normal [9].
Causes of potassium and magnesium deficiency
The most common causes of potassium and magnesium deficiency include:
- insufficient intake of potassium and magnesium into the body from food (with poor nutrition, deficiency in the diet of foods containing potassium and magnesium) or malabsorption (malabsorption syndrome, chronic gastroduodenitis, condition after intestinal resection);
- loss of potassium and magnesium due to vomiting and chronic diarrhea (intestinal secretions contain a large amount of potassium), sauna abuse, alcohol abuse, endocrine pathology (diabetes mellitus, hyperthyroidism, hyperparathyroidism, hyperaldosteronism);
- increased excretion of potassium and magnesium due to improper use of diuretics, primary and secondary hyperaldosteronism, renal tubular defects (Barter syndrome, Gitelman syndrome).
Manifestations of potassium and magnesium deficiency
The variety of manifestations of potassium and magnesium deficiency is due to the numerous functions of these cations in the body (Table 2). One of the most common manifestations of potassium deficiency is a disorder of neuromuscular transmission (muscle weakness, leg muscle spasms, paresthesia, extinction of tendon reflexes) [10]. Hypokalemia is also manifested by disorders of the cardiovascular system (decreased myocardial contractile function, dilatation of the heart cavities, decreased blood pressure) [11]. Damage to smooth muscles leads to intestinal paresis, vomiting, flatulence, constipation, and bladder atony [12].
Chronic hypokalemia can manifest itself as dysfunction of the central and peripheral nervous system (mild paresthesia of the face and extremities, decreased pain and tactile sensitivity, muscle weakness, tremor, hyperhidrosis).
Hypomagnesemia is characterized by increased fatigue, irritability, chronic fatigue, depression, apathy, dizziness, decreased memory and the ability to concentrate and maintain attention. The initial signs of magnesium deficiency include hair loss, brittle nails, caries, weather sensitivity, sleep disturbances (insomnia, nightmares, difficulty waking up even after a normal amount of sleep).
Both hypokalemia and hypomagnesemia are characterized by fluctuations in blood pressure (BP), the appearance of heart rhythm disturbances, and certain changes in the electrocardiogram (widening of the QRS complex, decreased ST segment, depression or inversion of the T wave, pronounced U wave) [13, 14].
Studies on the effectiveness of potassium and magnesium preparations
The SHEP study established an inverse statistically significant relationship between the level of potassium in the blood plasma and the incidence of cardiovascular complications: when the potassium level decreased to less than 3.5 mmol/l during chlorthalidone therapy, the risk of myocardial infarction, stroke, and cardiovascular events increased (Figure) [15]. In other words, when the potassium level decreases to less than 3.5 mmol/l during long-term therapy with thiazide diuretics, their positive effect on the prognosis is neutralized. It should be noted that in the first year of chlorthalidone therapy, hypokalemia was detected in 7.2% of patients.
Numerous data indicate that increasing the intake of both potassium and magnesium is accompanied by a decrease in the incidence of cardiovascular complications, improvement in the course of heart failure, and a decrease in the severity of left ventricular hypertrophy, arrhythmias, and new cases of diabetes mellitus.
A meta-analysis of a number of prospective studies showed that supplementation with 42 mmol potassium per day significantly reduced the relative risk of stroke (by 21%; p = 0.0007) with a trend towards a lower risk of coronary events (by 7%; p = 0.03) and CVD in general (by 26%; p = 0.0037) [16].
The randomized clinical trial PREDIMED [17] included 7216 patients with high and very high cardiovascular risk (mean age 67 years). At the time of inclusion in the study, patients did not have a diagnosed CVD, but were at high risk of developing it (type 2 diabetes mellitus, family history of CVD, overweight or obesity, smoking, arterial hypertension, hypercholesterolemia, low high-density lipoprotein cholesterol) . All patients were on a Mediterranean diet. Study participants were divided into three groups—three tertiles—depending on the amount of magnesium consumed daily (patients with the highest magnesium intake (tertile 3) also had higher plasma magnesium concentrations). The study lasted about five years. An inverse relationship was found between magnesium intake and the incidence of cardiovascular events, cardiovascular mortality, cancer mortality and total mortality (Table 3). According to the researchers, the distinct hypotensive, hypolipidemic and antiplatelet effects of magnesium, its ability to improve endothelial function and modulate inflammation, and reduce insulin resistance could have a positive effect on outcomes.
According to a meta-analysis of 19 studies, when using potassium supplements, blood pressure decreased by an average of 5.9/3.4 mm Hg. Art. [18]. The Canadian Guidelines for the Diagnosis, Risk Assessment, Prevention and Treatment of Hypertension (2021 Revision) emphasize the need to increase potassium intake to lower BP (in patients not at high risk for hyperkalemia) [19]. The hypotensive effect of potassium is provided by:
- increased natriuresis;
- changes in baroreceptor sensitivity;
- decreased sensitivity to catecholamines and angiotensin II;
- increase in Na+-K+-ATPase in vascular smooth muscle cells;
- improving the function of the sympathetic nervous system;
- increased sensitivity to insulin;
- decrease in intracellular Na+ and decrease in the formation of transforming growth factor beta [20].
Magnesium, being a natural physiological calcium antagonist, reduces systemic and pulmonary vascular resistance with a subsequent decrease in systemic blood pressure and a slight increase in cardiac index [4]. Reliable data have also been obtained (meta-analysis of 22 clinical studies) on the clinically significant antihypertensive effect of magnesium preparations.
Magnesium has been shown to suppress platelet activation by inhibiting thromboxane A2 or potentiating the synthesis of antiplatelet factors such as prostacyclin (prostaglandin I2). An increase in serum magnesium levels may interfere with the binding of fibrinogen to glycoprotein IIb–IIIa receptors by changing the structure of the receptors [8]. Intravenous administration of magnesium sulfate to healthy volunteers suppressed adenosine diphosphate-induced platelet aggregation by 40% [21].
A double-blind, placebo-controlled clinical study in patients with coronary heart disease (CHD) revealed a significant improvement in endothelial function and increased exercise tolerance with the use of magnesium supplements at a dose of 30 mmol/day [22]. According to a meta-analysis of 16 prospective studies (included over 310,000 patients), plasma magnesium levels are inversely proportional to the risk of developing cardiac arrhythmias and complications of coronary artery disease, including fatal myocardial infarction [23].
Magnesium deficiency is associated with impaired glucose tolerance [24]. With magnesium deficiency, insulin resistance can develop, which interferes with both the uptake of glucose into the cell and the transport of magnesium into the cell. It has been shown that the administration of magnesium as a dietary supplement to persons with arterial hypertension and/or type 2 diabetes mellitus helps reduce insulin resistance, the severity of dyslipidemia, and lower blood pressure levels [25–27]. Hypomagnesemia increases with decompensation of diabetes mellitus (additional losses of magnesium during polyuria).
Treatment and prevention of hypokalemia and hypomagnesemia
Even severe hypokalemia and hypomagnesemia often remain unrecognized in clinical practice. A doctor of any specialty must remember the clinical manifestations of potassium and magnesium deficiency in the body in order to promptly eliminate or prevent their development in risk groups with the help of adequate therapy. It must also be remembered that magnesium promotes the fixation of potassium in the cell. Without eliminating magnesium deficiency, it is impossible to solve the problem of intracellular potassium deficiency.
In many characteristics, potassium and magnesium complement each other and represent a kind of metabolic tandem [28]. The fairly high frequency and severity of combined deficiency of these macroelements justifies the advisability of using combined K+ and Mg2+ preparations for a number of conditions associated with a high risk of developing hypokalemia and hypomagnesemia.
Taking into account the role of potassium and magnesium ions in the development of pathology in the body, the need to correct the deficiency of these cations is obvious. Methods for correcting potassium and magnesium deficiency include dietary measures and pharmacotherapy. Typically, the intake of the required amount of potassium and magnesium into the body is ensured by a balanced diet. If there are clear clinical or subclinical signs of potassium and magnesium deficiency, replacement therapy is carried out, and subsequently in risk groups - preventive therapy. As already noted, a combination of potassium and magnesium ions in one preparation is preferable, since due to the common risk factors for development, potassium deficiency is often accompanied by magnesium deficiency, which requires simultaneous correction of the level of both ions [29–30]. The role of magnesium in maintaining intracellular potassium concentrations is especially important in cardiomyocytes, since magnesium reduces their sensitivity to the arrhythmogenic effects of cardiac glycosides [31].
The results of the randomized, multicenter, placebo-controlled, double-blind study MAGICA allowed us to consider magnesium and potassium preparations as the generally accepted European standard for the treatment of patients with arrhythmia while taking cardiac glycosides, diuretics, and antiarrhythmic drugs [32].
As an antiarrhythmic agent, magnesium salts are often used for ventricular tachycardia of the torsades de pointes type due to their ability to inhibit the development of trace depolarizations and thereby reduce the duration of the QT interval [33].
National guidelines for determining the risk and prevention of sudden cardiac death [34] consider electrolyte disturbances as a possible cause of sudden death in patients with a structurally normal heart. It is recommended to use potassium and magnesium salts for the treatment and prevention of ventricular arrhythmias when using thiazide diuretics, intoxication with cardiac glycosides, acute and chronic alcohol and drug intoxication, and anorexia. Moreover, in patients with verified life-threatening ventricular arrhythmias, it is advisable to maintain the serum potassium level in the range of 4.5–5.5 mmol/l, although a potassium level from 3.5 to 5.5 mmol/l is considered normal.
High clinical effectiveness is observed when potassium and magnesium are combined with aspartic acid. It has been established that aspartic acid, when included in the Krebs cycle, actively participates in the synthesis of ATP, promotes the entry of K+ and Mg2+ ions into the cell, restores the adequate functioning of ion pumps under hypoxic conditions, normalizes the processes of excitation and inhibition in nerve cells, and stimulates the immune system. In addition, aspartic acid promotes the conversion of carbohydrates into glucose and supplies myocytes with an energy substrate for oxidative phosphorylation [35]. Salts of aspartic acid have an adaptogenic effect, increasing the body's endurance and resistance to various stress factors.
Since 1960, K-Mg aspartate has been actively used in clinical practice. One of the most well-known preparations of K-Mg-aspartate is the drug Panangin, containing potassium and magnesium in an easily digestible form, produced in film-coated tablets containing 158 mg of potassium aspartate (36.2 mg of potassium) and 140 mg of magnesium aspartate ( 11.8 mg magnesium), as well as in the form of an injection solution in 10 ml ampoules containing 452 mg of potassium aspartate (103.3 mg of potassium) and 0.40 mg of magnesium aspartate (33.7 mg of magnesium). Recently, the drug Panangin Forte appeared on the pharmaceutical market, containing 316 mg of potassium aspartate (72.4 mg of potassium) and 280 mg of magnesium aspartate (23.6 mg of magnesium).
Panangin is the drug of choice for the complex treatment and prevention of hypokalemia and hypomagnesemia. The presence of a cardioprotective effect, a positive effect on liver function and blood pressure levels, and a reduced risk of arrhythmias significantly expand the range of clinical applications of Panangin [30, 36].
To eliminate severe deficiency of potassium and magnesium, Panangin Forte is prescribed (one tablet three times a day), to prevent the development of hypokalemia and hypomagnesemia - Panangin (one tablet three times a day after meals). The duration of treatment is determined individually and is usually three to four weeks, due to the gradual saturation of tissue depots.
The drug is indicated as an adjuvant therapy in patients with chronic heart disease (heart failure, post-myocardial infarction), cardiac arrhythmia (primarily ventricular arrhythmia), and during therapy with cardiac glycosides. The usual daily dose for adults is one or two tablets three times a day.
The use of the drug Panangin is pathogenetically justified for a number of conditions and diseases associated with the risk of developing hypokalemia and hypomagnesemia. The experience of clinical use of the drug Panangin confirms its high effectiveness in the correction and prevention of potassium-magnesium deficiency.
According to a number of randomized controlled trials [37–39], the addition of Panangin to standard therapy for coronary artery disease and chronic heart failure can reduce the number of angina attacks by 20% (p
The clinical effectiveness of the drug Panangin is due to the following pharmacological properties: improvement of vascular endothelial function and anti-atherosclerotic effect, antihypertensive effect and reduction of blood viscosity and thrombus formation [40].
Sometimes doctors are afraid to prescribe potassium and magnesium supplements because of the possible development of hyperkalemia and hypermagnesemia, but the risk of developing these conditions increases mainly in chronic kidney disease, in the case of severe (
A meta-analysis of 20 randomized clinical trials demonstrated the effect of oral potassium supplementation on serum potassium concentrations. Consumption of potassium supplements in doses up to 5460 mg/day for six months leads to a small but significant increase in circulating potassium concentration by 0.14 mmol/l, but does not contribute to the development of hyperkalemia or deterioration of renal function. Thus, the use of potassium supplements is safe for patients receiving blockers of the renin-angiotensin-aldosterone system (RAAS) [41]. Since RAAS inhibition is currently a key strategy in the treatment of hypertension and cardiovascular disease [42], the simultaneous administration of potassium and magnesium supplements and RAAS blockers is being considered in some situations. According to a meta-analysis of 39 studies, when RAAS blockers were prescribed to patients without chronic kidney disease, the incidence of hyperkalemia did not exceed 2% [43].
Panangin can be called the drug of first choice for relieving identified potassium deficiency (decreased K+ concentration in serum
Conclusion
An important component of modern clinical practice should be monitoring of electrolyte, primarily potassium-magnesium balance. If there is a high risk of developing hypokalemia and hypomagnesemia, both correction (if detected) and prevention of the development of potassium and magnesium deficiency should be carried out. Maintaining the potassium-magnesium balance provides an additional therapeutic effect in patients with arterial hypertension, diabetes mellitus, congestive heart failure, as well as in patients with a high risk of developing cerebral stroke and heart rhythm disturbances. The optimal option in the pharmacological correction and prevention of hypokalemia and hypomagnesemia is the use of K-Mg aspartate (Panangin and Panangina Forte), many years of clinical experience of which have confirmed its high therapeutic efficacy and safety.