General urine analysis
What is a general urine test?
A general urinalysis includes assessment of the physicochemical characteristics of urine and microscopy of sediment. This study allows you to evaluate the function of the kidneys and other internal organs, as well as identify the inflammatory process in the urinary tract. Together with a general clinical blood test, the results of this study can tell quite a lot about the processes occurring in the human body and, most importantly, indicate the direction of further diagnostic search.
Physico-chemical characteristics of urine:
- color;
- transparency;
- specific gravity (relative density);
- pH (acidity);
- protein;
- glucose;
- bilirubin;
- urobilinogen;
- ketone bodies;
- nitrites;
Microscopy of urinary sediment (the study is done in case of pathology in a general urine analysis or at the request of the customer):
Organized urine sediment:
- red blood cells;
- leukocytes;
- epithelial cells;
- cylinders;
- bacteria;
- yeast fungi;
- slime.
- Unorganized urine sediment (crystals).
Indications for the purpose of analysis:
- diseases of the urinary system;
- suspected diabetes mellitus;
- assessment of the toxic state of the body;
- assessment of the course of the disease;
- monitoring the development of complications and the effectiveness of treatment;
- Persons who have had a streptococcal infection (tonsillitis, scarlet fever) are recommended to take a urine test 1-2 weeks after recovery.
Preparing for the study:
On the eve of the study, it is not recommended to eat vegetables and fruits that can change the color of urine (beets, carrots, etc.), as well as diuretics. Before collecting urine, perform a thorough hygienic toilet of the genitourinary organs. Women are not recommended to take the test during menstruation. The container for collecting urine must be clean and dry. To properly collect urine, you need to: during the first morning urination, release a small amount of urine into the toilet, and then, without interrupting urination, place a container for collecting urine, into which to collect about 100-150 ml of urine.
Execution time: 1 working day.
Physico-chemical characteristics.
Color. Normal urine has a straw-yellow color of varying intensities. The color of urine in healthy people is determined by the presence of substances formed from blood pigments (urobilin, urochromes, hematoporphyrin, etc.). The color of urine changes depending on its relative density, daily volume and the presence of various coloring components entering the human body with food, medications, and vitamins.
For example:
- the red color may be due to amidopyrine;
- pink - acetylsalicylic acid, carrots, beets;
- greenish blue - methylene blue;
- brown - bear ears, sulfonamides, activated carbon;
- greenish-yellow - rhubarb, Alexandria leaf;
- deep yellow - riboflavin, 5-NOK, furagin.
Normally, the more intense the yellow color of the urine, the higher its relative density and vice versa. Concentrated urine has a brighter color. However, the normal color of urine does not indicate that it is the urine of a healthy person.
Transparency. Normal freshly passed urine is clear. A small cloud of turbidity may also appear in normal urine due to epithelial cells and mucus. Severe cloudiness of urine can be caused by the presence in it of red blood cells, leukocytes, fat, epithelium, bacteria, and significant amounts of various salts (urates, phosphates, oxalates). The causes of cloudy urine are determined by microscopy of sediment and chemical analysis. Using a three-glass sample, you can roughly answer the question - from which part of the urinary system are leukocytes and mucus released (from the urethra, bladder or renal pelvis). Slightly cloudy urine is often observed in older people (mainly from the urethra). The clouding of urine that occurs when standing in the cold usually depends on the deposition of urates, and in the heat - phosphates. However, clear urine does not yet indicate the absence of diseases of the genitourinary system.
Specific gravity (relative density). Measuring urine specific gravity is a simple test that measures the ability of the kidneys to concentrate urine and dilute urine. A decrease in the concentrating ability of the kidneys occurs simultaneously with a decrease in other renal functions. Normally functioning kidneys are characterized by wide fluctuations in the specific gravity of urine during the day, which is associated with periodic intake of food, water and fluid loss from the body (sweating, breathing). The kidneys under different conditions can excrete urine with a relative density of 1.001 to 1.040.
pH (acidity). The kidneys excrete “unnecessary” substances from the body and retain necessary substances to ensure the exchange of water, electrolytes, glucose, amino acids and maintain acid-base balance. The reaction of urine - pH - largely determines the effectiveness and characteristics of these mechanisms. Normally, most often the urine reaction is slightly acidic (pH 5.0 - 7.0). It depends on many factors: age, diet, body temperature, physical activity, kidney condition, etc. The lowest pH values are in the morning on an empty stomach and the highest after meals. When consuming predominantly meat foods, the reaction is more acidic; when consuming plant foods, the reaction is alkaline. When urine stands, the pH value tends to increase due to the formation of ammonium by microorganisms (pH 9 indicates improper preservation of the sample). Constant pH values (7-8) suggest the presence of a urinary tract infection. Changes in urine pH depend on blood pH: with acidosis, urine has an acidic reaction; for alkalosis - alkaline. A discrepancy between these indicators occurs with chronic damage to the kidney tubules: hyperchloric acidosis is observed in the blood, and the urine reaction is alkaline.
Protein. Protein is normally absent in urine or there are small traces of it, since protein molecules are large molecules that are not able to pass through the membrane of the glomeruli.
Glucose. Normally, there is no sugar in the urine, since all glucose, after being filtered through the glomerular membrane of the kidneys, is completely absorbed back into the proximal tubules. The appearance of glucose in the blood, glucosuria, can be:
- physiological (under stress, taking increased amounts of carbohydrates in older people);
- extrarenal (diabetes mellitus, pancreatitis, diffuse liver damage, pancreatic cancer, hyperthyroidism, Cushing's disease, pheochromocytoma, hyperthyroidism, acromegaly, traumatic brain injury, stroke, poisoning with carbon monoxide, morphine, chloroform);
- renal (renal diabetes, chronic nephritis, acute renal failure, pregnancy, phosphorus poisoning, certain medications).
Glucose is a substance with a high renal excretion threshold. The renal excretion threshold is the concentration of a substance in the blood, exceeding which leads to the cessation of its reabsorption in the tubules. When the blood glucose concentration is more than 8.8-9.9 mmol/l, sugar appears in the urine.
Bilirubin. Normally, bilirubin is practically absent in urine. Formed during the destruction of hemoglobin in the cells of the reticuloendothelial system, about 250-350 mg/day. When the concentration of conjugated bilirubin in the blood increases, it begins to be excreted by the kidneys and is found in the urine. Bilirubinuria is detected in parenchymal liver lesions (viral hepatitis), mechanical (subhepatic) jaundice, cirrhosis, cholestasis. In hemolytic jaundice, the urine usually does not contain bilirubin. It should be noted that only direct (bound) bilirubin is excreted in the urine.
Urobilinogen. Urobilinogen bodies (I-urobilinogen, d-urobilinogen, third urobilinogen, stercobilinogen) are derivatives of bilirubin and are normal products of catabolism, which under physiological conditions are formed at a certain rate, constantly excreted in feces and in small quantities in urine. Normal urine contains traces of urobilinogen. Its level increases sharply with hemolytic jaundice (intravascular destruction of red blood cells), as well as with toxic and inflammatory lesions of the liver, intestinal diseases (enteritis, constipation). With subhepatic (obstructive) jaundice, when there is complete blockage of the bile duct, there is no urobilinogen in the urine.
Ketone bodies. Ketone bodies include acetone, acetoacetic and beta-hydroxybutyric acids. A healthy person excretes 20-30 mg of ketones per day in urine. An increase in the excretion of ketones in the urine, ketonuria appears when there is a violation of carbohydrate, fat or protein metabolism.
Nitrites. There are no nitrites in normal urine. In urine, they are formed from nitrates of food origin (when eating plant foods) under the influence of bacteria, if the urine was in the bladder for at least 4 hours. Detection of nitrites in the urine (positive test result) indicates infection of the urinary tract. However, a negative result does not always exclude bacteriuria. Urinary tract infection varies among different populations and is dependent on age and gender. The following categories of people are more susceptible to an increased risk of asymptomatic urinary tract infections and chronic pyelonephritis, other things being equal:
- girls and women;
- elderly people (over 70 years old);
- men with prostate adenoma;
- diabetic patients;
- patients with gout;
- patients after urological operations or instrumental procedures on the urinary tract.
Microscopy of urinary sediment. In urinary sediment, organized sediment is distinguished (cellular elements, cylinders, mucus, bacteria, yeast fungi) and unorganized (crystalline elements).
Red blood cells. 2 million red blood cells are excreted in the urine per day, which, when examining urine sediment, is normally less than 3 red blood cells per field of view for women, and 1 red blood cell per field of view for men. Anything higher is hematuria. Highlight:
- gross hematuria (when the color of urine is changed);
- microhematuria (when the color of urine is not changed, and red blood cells are detected only under a microscope).
In urinary sediment, red blood cells can be unchanged (containing hemoglobin) and changed (deprived of hemoglobin, leached). The appearance of leached red blood cells in the urine is of great diagnostic importance, because they most often have a renal origin and are found in glomerulonephritis, tuberculosis and other kidney diseases. Fresh, unchanged red blood cells are more likely to cause damage to the urinary tract (urolithiasis, cystitis, urethritis). To determine the source of hematuria, a “three-vessel” test is used: the patient collects urine sequentially into three vessels. When bleeding from the urethra, hematuria is greatest in the first portion (unchanged red blood cells), from the bladder - in the last portion (unchanged red blood cells), with other sources of bleeding, red blood cells are distributed evenly over all three portions.
Leukocytes. Leukocytes in the urine of a healthy person are contained in small quantities (in men 0–3, in women and children 0–6 leukocytes per field of view). An increase in the number of leukocytes in the urine (leukocyturia) indicates inflammatory processes in the kidneys (pyelonephritis) or urinary tract (cystitis, urethritis). To establish the source of leukocyturia, a three-glass test is used: the predominance of leukocytes in the first portion indicates urethritis or prostatitis, in the third - cystitis, an even distribution of leukocytes in all portions can most likely indicate kidney damage. So-called sterile leukocyturia is possible. This is the presence of leukocyturia in the absence of bacteriuria and dysuria (with exacerbation of chronic glomerulonephritis, contamination during urine collection, condition after treatment with antibiotics, bladder tumors, renal tuberculosis, interstitial analgesic nephritis). Urethral syndrome. This is frequent, painful urination and leukocyturia in the absence of bacteriuria. Occurs predominantly in women. In 30-40% of cases in women with symptoms of urinary tract infection, bacteriuria cannot be detected. The reasons for the negative result are that the true causative agent of this condition, as a rule, is anaerobic bacteria, ureaplasma, chlamydia, gonococcus, and viruses. And they all require sowing on special media.
Epithelial cells. Epithelial cells are almost always found in urinary sediment. Normally there are no more than 10 of them in the field of view. Epithelial cells have different origins:
- cells of stratified squamous keratinizing epithelium (washed off with night urine from the external genitalia);
- cells of stratified squamous non-keratinizing epithelium (from the distal parts of the male and female urethra and vagina, of little diagnostic value);
- transitional epithelial cells (lining the mucous membrane of the bladder, ureters, pelvis, large ducts of the prostate gland);
- cells of the renal (tubular) epithelium (lining the renal tubules).
Cylinders. The cylinder is a protein that is coagulated in the lumen of the renal tubules and includes in its matrix any contents of the lumen of the tubules. The cylinders take the shape of the tubules themselves (cylindrical cast). In the urine of a healthy person, single cylinders can be detected in the field of view of a microscope per day. Normally, there are no casts in a general urine analysis. The appearance of casts (cylindruria) is a symptom of kidney damage. The type of cylinders has no special diagnostic significance. Cylinders are distinguished:
- hyaline (with overlay of erythrocytes, leukocytes, renal epithelial cells, amorphous granular masses);
- granular;
- waxy;
- pigmented;
- epithelial;
- erythrocyte;
- leukocyte;
- fatty.
Bacteria. Normally, urine in the bladder is sterile. When urinating, microbes from the lower part of the urethra enter it, but their number is not > 10,000 in 1 ml. Bacteriuria is defined as the detection of more than one bacterium in the field of view (qualitative method), which implies the growth of colonies in culture exceeding 100,000 bacteria per 1 ml (quantitative method).
It is clear that urine culture is the gold standard for diagnosing urinary tract infections. The presence of bacteria in the urine in the absence of complaints is regarded as asymptomatic bacteriuria. A similar condition often occurs with organic changes in the urinary tract; in women who are promiscuous and in older people. Asymptomatic bacteriuria increases the risk of urinary tract infection, especially during pregnancy (infection develops in 40% of cases). The detection of bacteria in a urine test indicates an infectious lesion of the urinary system (pyelonephritis, urethritis, cystitis, etc.). The type of bacteria can only be determined through bacteriological examination.
Yeast fungi. The detection of yeast of the genus Candida indicates candidiasis, which most often occurs as a result of irrational antibiotic therapy, the use of immunosuppressants, and cytostatics. Determining the type of fungus is possible only through bacteriological examination.
Slime. Mucus is secreted by the epithelium of the mucous membranes. Normally absent or present in urine in small quantities. During inflammatory processes in the lower parts of the urinary tract, the mucus content in the urine increases. An increased amount of mucus in the urine may indicate a violation of the rules of proper preparation for taking a urine sample.
Crystals (disorganized sediment). Urine is a solution of various salts, which can precipitate (form crystals) when the urine stands. Low temperature promotes the formation of crystals. The presence of certain salt crystals in the urinary sediment indicates a change in the reaction towards the acidic or alkaline side. Excessive salt content in urine contributes to the formation of stones and the development of urolithiasis. At the same time, the diagnostic value of the presence of salt crystals in urine is usually small.
Cost of seeing a doctor
| Name of service | Price, rub.) |
| Primary appointment with a general practitioner | 2000 rub. |
| Repeated appointment with a general practitioner | 1500 rub. |
Urinalysis
| Code | Name of the study | Biological material | Result | ****Execution period | Price | ***CIT | Note |
| 110101 | General urine analysis | urine (morning portion) | count | 1 k.d. | 345 rub. | 690 rub. | 0 |
| 110102 | 2 glass sample | urine | count | 1 k.d. | 575 rub. | 1150 rub. | 0 |
| 110103 | 3 glass sample | urine | count | 1 k.d. | 690 rub. | 1380 rub. | 0 |
| 110104 | Rehberg's test | urine + blood (serum) | count | 1 k.d. | 403 rub. | 805 rub. | 0 |
| 110105 | Urine analysis according to Zimnitsky | urine | count | 1 k.d. | 920 rub. | 1840.00 | 0 |
| 110106 | Urinalysis according to Nechiporenko | urine | count | 1 k.d. | 345 rub. | 690 rub. | 0 |
Advanced urine analysis study
| Code | Name of the study | Biological material | Result | ****Execution period | Price | ***CIT | Note |
| 090101 | Creatinine | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090102 | Urea | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090103 | Uric acid | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
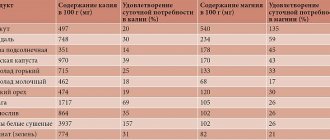
| 090104 | Phosphorus | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090105 | Magnesium | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090106 | Glucose | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090107 | Calcium | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090108 | Alpha amylase | urine | count | 1 k.d. | 345.00 rub. | 690.00 rub. | 0 |
| 090109 | Total protein | urine | count | 1 k.d. | 230.00 rub. | 460.00 rub. | 0 |
| 090110 | Na+/K+/Cl- | urine | count | 1 k.d. | 460.00 rub. | 920.00 rub. | 0 |
| 090112 | Microalbumin | urine | count | 1 k.d. | 575.00 rub. | 1150.00rub | 0 |
| 090121 | Deoxypyridinoline (DPID) | urine | count | 3-5 k.d. | 2300.00 rub. | 0 ₽ | 0 |
All our services and prices
Preparing for the OAM test for cystitis
On the day before taking biomaterial, it is advisable to refrain from physical activity, drinking alcohol, and not eat vegetables and fruits (beets, carrots, citrus fruits, watermelons), red wine, and multivitamins, which can change the color of urine.
Avoid taking diuretics for 48 hours before urine collection (in consultation with your doctor).
Urine should be collected before starting antibiotic therapy.
Carry out a thorough toileting of the external genitalia under the shower with soap (it is prohibited to use hygiene products with antiseptics). For men, pull back the foreskin of the penis, wash the head well with warm water, and dry with a paper towel.
Women during menstruation should place a tampon in the vagina before collecting urine and inform the attending physician that the test was performed during menstruation.
How to treat?
After discovering the true cause of the disease and making an accurate diagnosis, the doctor advises the patient in detail about the upcoming treatment.
- Drinking plenty of fluids is recommended. Collections of anti-inflammatory herbs, juices, mineral water without gases, etc. are best suited for these purposes.
- Treatment must be comprehensive. Painkillers are used to relieve pain. Antibiotics and anti-inflammatory drugs will eliminate inflammation. Medicines are prescribed depending on the disease that caused the increased secretion of mucus.
- It is better to forget about bad habits forever. You need to eat properly: fractionally and in small portions. Salty, spicy, smoked foods, sweets, milk, white bread and baked goods are excluded from the menu.
Mucus mixed with pus and blood, which has an unpleasant odor, is not a disease in itself, but it signals a serious illness.
Symptoms
Mucus in a urine test is a symptom that you definitely need to pay attention to. Although its very appearance may go unnoticed by a person, the disease developing against this background will certainly be accompanied by characteristic pain when urinating, pain in the lower abdomen, increased body temperature and other signs.
In men, problems with the genitourinary tract cause discomfort in the lumbar region. The pain radiates to the groin, genitals and scrotum. When emptying the bladder, a burning sensation and pain are felt. In women, vaginal discharge increases, pain is concentrated in the lower back and in the area of the appendages. The urine becomes cloudy and smells unpleasant.
Problems of the genitourinary system, for which mucus in a urine test is a characteristic sign, can also give rise to other symptoms: headaches, sleep disorders, high blood pressure, nausea, vomiting, loss of appetite, weakness, swelling of the arms and legs, chills, dry skin, seizures, etc. However, only a specialist should give a final conclusion about the causes of the disease and select treatment!
Normal indicators
The human body constantly stimulates the process of rejection of epithelial cells, which can form a small amount of impurities released during urination. Diagnostic laboratories evaluate mucus in a urine test using a special plus system (from 1 to 4).
Normal indicators of its presence are usually designated by 1 plus, and maximum indicators, at which the consistency of the impurity resembles thick jelly, by four. The results are deciphered by the attending physician.
Appearance
Color. Normal urine color is yellow: from straw yellow to dark amber. The shade depends on the concentration of urochrome, a coloring pigment in urine. Concentrated urine that has been sitting in the bladder overnight has more urochrome, so the urine will be more amber. And if a person has recently drunk water, the color will be more like straw.
In this case, urine can be colored in almost all the colors of the rainbow. Moreover, an unusual shade can either be a variant of the norm or indicate a disease. Moreover, urinary tract infections can produce different shades of urine - the color depends on the specific type of pathogenic microorganisms.
“Sometimes a patient’s urine turns red,” says Svetlana Artemova, candidate of medical sciences, nutritionist and nephrologist at GMS Clinic. Without analysis it is impossible to understand why this happens. This may be due, for example, to eating beets, to treatment with sulfonamides, or to rhabdomyolysis, a condition in which muscle tissue is destroyed.”