General information
In the structure of the incidence of acute respiratory viral infections, which account for about 90% of all infectious diseases, influenza . One of the pressing problems today is influenza, once called “swine flu,” which is caused by the A/H1N1 virus. Refers to an emergent infection (that is, occurring suddenly) with the possibility of rapid transmission of the virus to a new host. Its distinctive feature from seasonal influenza is its high contagiousness, which contributes to the development of epidemics and pandemics, as well as the high risk of developing complicated forms in the form of community-acquired severe pneumonia and acute respiratory failure . Virologists call the influenza A(H1N1) pdm09 strain a four-time reassortant (mixed) virus because it contains:
- Genes of swine influenza circulating among North American pigs.
- Genes of swine influenza circulating among pig populations in Asia/Europe.
- Genes for seasonal influenza circulating among humans.
- Avian influenza genes .
Today, influenza A viruses are characterized by extremely high ecological plasticity, significantly exceeding all known orthomyxoviruses . The natural reservoir of influenza A is birds of the aquatic/semi-aquatic complex. A characteristic feature of influenza A viruses is the ability to overcome interspecies barriers and infect populations of potentially new hosts with rapid adaptation to them and circulation among them over a long period of time, which is the cause of epizootics, epidemics and even pandemics. Mortality from swine flu varies significantly from year to year. Thus, in 2009–2010, 622 deaths from influenza A (H1N1) pdm09 were recorded in the Russian Federation. In subsequent years, the intensity of the epidemic was significantly lower. How many people have died from swine flu in 2021? Mortality in the 2015–2016 season amounted to 309 cases, while in 2015 significantly fewer people died - 44 people. For the 2015–2016 season, the circulation of influenza pathogens throughout the epidemic rise is characterized by the dominance of one virus - swine influenza A (H1N1) pdm09, which did not actively circulate and did not undergo mutations over the previous 3 years. It is obvious that the formation of pandemic variants of the influenza virus is based on 2 mechanisms:
- adaptation of an animal/avian virus directly to humans;
- reassortment (mixing) between avian/animal and human influenza viruses.
Since the influenza A virus (НШ1/2009) differs in its antigenic properties from traditional seasonal influenza, the disease occurs predominantly in the relatively young non-immune part of the human population, in particular, children and people aged 20 to 40 years.
Megafarms
At the end of March 2009, a five-year-old boy in the small village of La Gloria, Veracruz, municipality of Pirot, Mexico, fell ill with the flu. This ordinary, seemingly unremarkable event was, in fact, comparable in significance to the beginning of a new world war. The boy was ill for 3 days before he felt an improvement in his condition and completely recovered. But after just two weeks, there were already more than 800 sick people in Perot, and the boy was called “zero.” A month later, the disease had already captured 60% of the population of Veracruz.
Edgar Hernandez's mother, besieged by journalists, sobbed and insisted that her son could not be the cause of this disaster. She and her neighbors tended to blame the pig farms of Perota, the capital of Veracruz state. Situated 120 miles from Mexico City, surrounded by mountains on all sides, it was home to only 35,000 bipedal inhabitants and up to a million artiodactyls. Yes, yes, the pig population was tens of times larger than the human population. Residents have complained for years about the consequences of pig farming. The smells from the grotesquely massive manure cesspools, blazing in the sun, permeated not only the air, but the houses themselves, clothes and even things. Dust clouds of dried manure travel from these parts for many miles, picked up by hot winds and stopping the breath upon arrival.
And SV doesn’t exaggerate anything. The thing is that we are not talking about traditional pig farms, or even about Chinese pig plants - we are talking about Grangie Carroll de Mexico (“GCM”) or pig-breeding mega-plants.
These are the colossi of animal agriculture, representing overpopulation, global warming and the endless hunger of all 7 billion human throats.
Over the past twenty years, the Mexican livestock industry has undergone a number of radical changes, with production volumes increasing and the number of farmers decreasing. In many ways, this transformation mirrored the industrialization of agriculture in the United States itself in the late 1980s and 1990s. The irony is that in both cases, the catalysts for change were American megacorporations. But, if at home, in the States, their goal was safe and legally correct production while maximizing profits, then, thanks to the trade in liberalism in Mexico itself, NAFTA and the American lobby, what happened in Veracruz happened. Cities of pigs... and pigs, as you remember, without vaccination and in such a pig pile are an incubator for the production of new strains of influenza.
So who was more to blame? A million pig-nosed incubators that are unvaccinated reservoirs? Farm workers? Mass consumption? Mexico's gluttonous neighbor who needs thousands of tons of bacon? Or 5-year-old Edgar?
Pathogenesis
After infection, virus A enters the mucous membranes of the larynx, trachea and bronchi, where it begins the process of reproduction in columnar epithelial cells. Against the background of virus reproduction, degenerative changes in the epithelium increase and with a massive release of mature virions, massive cell death is observed, manifested by inflammatory phenomena in the upper respiratory tract (mainly in the trachea/bronchi). This process is pathogenetically manifested by disturbances in the function of external respiration, a decrease in blood oxygenation and the supply of oxygen to organs and tissues. Clinical signs at this stage are manifested by intoxication syndrome, which is caused by the action of viral toxins and various decay products of epithelial cells, which have a toxic effect on the cardiovascular and central/autonomic nervous system.
Circulatory disorders play a leading role in the damage to systems/organs during influenza. The toxic effect of the virus on the vascular system is manifested by fragility of the vascular walls and an increase in their permeability, disturbances in the capillary circulatory system and the frequent development of hemorrhagic syndrome and the formation of small blood clots. The formation of neurotoxic syndrome is caused by a violation of cerebral hemodynamics. The pronounced immunosuppressive and vasospastic effect of the influenza virus creates a high risk of secondary infection, especially in the respiratory system, which is greatly facilitated by the accumulation of fluid in the lumen of the alveoli and interstitial tissue, disruption of the drainage function of the bronchi and microcirculation, as well as increased pressure in the pulmonary circulation.
Classification
The classification of swine flu is based on several factors. According to the degree (form) of severity of the disease, mild, moderate and severe forms are distinguished.
According to the nature of the flow:
- Uncomplicated - occurs with typical symptoms ( runny nose , cough , nasal congestion, headache , myalgia , weakness , arthralgia , less often with gastrointestinal disorders).
- Complicated (with the development of virus-associated/bacterial complications with damage to the lower respiratory tract (acute tracheitis , bronchitis , pneumonia ) and chronic diseases).
- According to topical signs (localization of the lesion): acute rhinitis , pharyngitis , tracheitis , laryngitis , bronchitis , pneumonia .
Causes
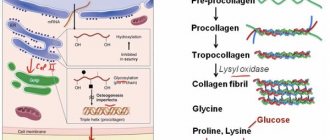
Swine flu (h1n1) is caused by an RNA virus of the Orthomyxoviridae family, genus Influenza type A. The genome structure of the A virus is shown below.
Virus A has a spherical structure with a diameter of 80 to 120 nm and contains a lipoprotein envelope with a segmented genome, which includes 8 single-stranded RNA segments, the length of which varies from 890 to 2341 nucleotides. Influenza A viruses contain hemagglutinin (HA) and neuraminidase (NA), which have pronounced neuraminidase/hemagglutinating activity, as their main structural and antigenic components. The main antigen is neuraminidases, which neutralize antibodies and take part in the binding of virus A to host cell receptors. Influenza A viruses have a pronounced ability to change the NA/NA structure. There are 2 mechanisms of variability characteristic of influenza A:
- antigenic drift - represents point mutations directly in the viral genome with changes in HA and NA;
- antigenic shift - which is based on the process of complete replacement of one/both surface glycoproteins of the virus (HA and NA) through reassortment/recombination, which leads to the emergence of a fundamentally new variant of the virus with high virulence.
Both of these processes can affect only hemagglutinin (HA) or both hemagglutinin and neuraminidase (NA). This allows the newly formed antigenic variant of the A virus not to fall under the influence of population immunity, causing sporadic/epidemic increases in incidence every year. The ability of influenza A viruses to exhibit high antigenic variability essentially determines their specificity, epidemiological features, and high susceptibility of the population.
Why doesn't the vaccine protect 100%?
Previously, we have already examined cases when vaccinated people can also get sick. Once again, we note that any vaccines do not provide a 100% guarantee. In the instructions for the drugs you will see efficiency indicators that are always above 80%, close to 95-99%.
Efficacy is influenced by the initial characteristics of the vaccine and the immune status of the individual. In the case of influenza, we described the additional risks and complexities associated with yearly forecasting and updating of strains.
Scientists have extensive experience in combating this elusive enemy; more than 2,000 serotypes of influenza viruses are known in the world. However, the risk of a completely new mutation always exists, and scientists cannot yet control this. Just like they cannot create a vaccine that would protect against influenza for life and 100%.
Whether you should get vaccinated when you are unsure of the Global Influenza Surveillance System forecasts is up to you. Perhaps the numbers will help you make a difficult choice: in Russia, among those sick with influenza A, 91.8% were unvaccinated, and among those who died, 100%.
Epidemiology
The lack of specific immunity in the human population to shift (new) variants of the influenza A virus leads to an extremely rapid spread of influenza over a wide area. The rate of H1N1 infection among contacts of sick people varies between 22-33%.
The source of infection is a sick person who is in the acute period of the disease, including those with an asymptomatic course, or less often a convalescent person who releases the pathogen within 2 weeks from the onset of the disease. The leading mechanism of transmission of the influenza virus is airborne droplets. The virus is released from the body when coughing, sneezing, talking, breathing, crying and poses a danger to a person located within a radius of 2-2.5 meters from the patient.
Much less frequently, the virus is transmitted through household contact through discharge from the patient’s hands (spread from the hands to the mucous membranes of the eyes, nose and mouth) and household items (towels, dishes, tables, surfaces). Virus A retains its pathogenic properties in the environment for 2-8 hours.
The influenza virus is unstable in the external environment and escapes when:
- exposure to bactericidal agents;
- exposure to alcohol solution;
- temperature rises to 75 C.
The vast majority of people do not have immunity to swine flu viruses, which could prevent the development of infection. Swine flu can occur in the form of sporadic cases and epidemic outbreaks with a predominantly winter-spring seasonality.
The patient poses a danger to others starting from the last day of the incubation period and the next 7 days from the onset of clinical symptoms. If the duration of the disease is more than 7 days from the moment of the first symptoms, then such patients should be regarded as potentially contagious until all signs of the disease disappear. It should be taken into account that the duration of the period of contagiousness can vary significantly depending on the characteristics/specificity of the influenza A/H1N1 virus strain. Children may be potentially infectious for a longer period of time.
Swine flu is a highly contagious disease with universal susceptibility to infection. There are several groups at high risk of developing severe forms of influenza A/H1N1:
- adults over 65 years of age and children under 2 years of age;
- pregnant women;
- patients with excess body weight (body mass index ≥ 35);
- persons with concomitant chronic diseases ( diabetes mellitus , immunodeficiency , chronic pulmonary diseases, blood diseases, oncology , heart disease, liver disease, urinary system ).
Immunity in patients after swine flu is short-lived (up to 1 year) and type-specific.
Today: modern vaccines
The production of flu vaccines is generally a constant evolution. The first vaccines were live
.
Weakened viruses were used during production. Used as a nasal spray. Had a lot of side effects. Representative: Ultravac (Russia).
Then they began to use inactivated
vaccines.
The first of them contained, although purified, whole viruses ( whole virion vaccines
).
Their reactogenicity (ability to cause side effects) was very high. Representative: Grippovac (Russia).
Later, they began to produce vaccines with the destroyed virus ( split or split vaccines
).
They have fewer adverse reactions and fairly high immunogenicity. Such vaccines include all virion proteins of the virus (both surface and internal antigens), but due to high purification they do not contain viral lipids and chicken embryo proteins. Representatives: Ultrix (Russia), FLU-M (Russia), Vaxigrip (France), Fluarix (Germany), Fluvaxin (China).
The next class of vaccines is subunit
.
They contain only purified influenza virus surface antigens. Not only the virion and chicken embryo proteins were removed, but also internal antigens. Due to this, a significant reduction in reactogenicity was achieved. To increase the duration and intensity of immunity, manufacturers of subunit vaccines often add an adjuvant to the composition - a substance that enhances the immune response. Representatives: Influvac (Netherlands), Grippol plus (Russia), Sovigripp (Russia).
The last generation includes virosomal
vaccines in which surface antigens are presented in the form of virosomes (pseudoviral structures) that mimic the influenza virus, due to which the vaccine better “educates” the immune system of the person being vaccinated.
Representative: Inflexal V (Switzerland).
In addition to updating the technology for inactivation, assembly, and purification of influenza vaccines, other scientific work is underway to find ways to improve the quality, tolerability and effectiveness of influenza vaccines.
One of the ways to increase efficiency was the WHO recommendation to reorient production from 3-valent to 4-valent ones
vaccines.
Quadrivalent
vaccines contain proteins from four dangerous strains.
Examples: Ultrix Quadri (Russia), Grippol quadrivalent (Russia).
The Russian new generation vaccine “Ultrix Quadri” contains two strains A and B. Among the type A viruses there is H1N1 (similar to the culprit of “Spanish Flu 1918” and “Swine Flu 2009”). It is noteworthy that it was with this drug that Russian President Vladimir Putin, Health Minister Veronika Skvortsova and other members of the Government were vaccinated in 2021.
Symptoms
The symptoms of swine flu in humans are not fundamentally different from those of seasonal flu. The onset of swine influenza A (H1N1) pdm 2009 in adults usually develops against the background of a short-term (1-2 hours) prodromal period or generally complete health. Characteristic for its onset is the predominance of intoxication syndrome over catarrhal symptoms of lesions of the respiratory tract (nasopharynx, trachea, larynx). Body temperature reaches a level of 38.5–40°C already in the first hours of the disease with the simultaneous manifestation of other symptoms of intoxication, the manifestation of which varies from mild to extremely severe, which, in fact, determines the severity of the disease.
The main manifestations of intoxication syndrome are: severe weakness, headache , chills , pain when pressing/moving the eyeballs, aching muscles/joints, photophobia , lacrimation, increased fatigue, lethargy . , dizziness , convulsions , fainting , hallucinations , and delirium may occur .
Catarrhal syndrome (respiratory tract syndrome) with swine flu is usually not expressed sharply and is manifested by scanty serous-mucous rhinitis , difficulty in nasal breathing, sore throat, rawness/dry infrequent rough “tracheal” cough, accompanied by chest pain. Swine flu is characterized by moderate hyperemia of the arches with a bluish tint, injection/graining of blood vessels on the soft palate, as well as the posterior wall of the pharynx.
The developing hemorrhagic syndrome is manifested primarily by nosebleeds, less often, petechial/pinpoint rash on the skin of the neck, chest, face and upper extremities, as well as hemorrhages on the back wall of the pharynx, mucous membrane of the oro/nasopharynx, conjunctiva of the eyes, less often - blood in the sputum and vomit. masses.
In severe forms, adults may develop signs of pneumonia with the appearance of sweating, scattered moist wheezing, persistent cough, high body temperature, severe symptoms of intoxication, as well as the rapid development of respiratory distress syndrome . Also, one should take into account the possibility of bacterial infections and exacerbation of chronic diseases, which significantly aggravate the course of the disease.
When to call a doctor if you have the flu?
For children, the reason to call a doctor is frequent and difficult breathing, bluish skin tint, lethargy and drowsiness, refusal to drink and eat, repeated vomiting, high temperature (39 or more).
For adults – shortness of breath, worsening during the day, chest pain, repeated vomiting, severe weakness and dizziness, high fever.
In order for the efforts of doctors to be effective, you need to seek help from doctors in a timely manner, i.e. immediately when the above symptoms appear.
Tests and diagnostics
Clinical diagnosis is difficult due to the lack of specific symptoms and the similarity of the swine flu clinic to the symptoms of regular seasonal flu. Establishing a diagnosis can indirectly help:
- The patient has had contact with patients with a confirmed diagnosis of swine flu (epidemiological history).
- Absence/unexpressed sore throat accompanied by a strong, predominantly dry cough.
- The presence of gastrointestinal disorders against the background of respiratory syndrome and fever.
- Development of pneumonia on 2-3 days.
A final diagnosis of swine flu is possible only on the basis of laboratory confirmation, for which the following are used:
- Method of PCR diagnostics of nasopharyngeal mucus samples (detection of RNA of the influenza A (H1N1) virus strain.
- Culture of nasopharyngeal mucus/sputum on certain nutrient media.
Diet
Diet for influenza, ARVI, colds
- Efficacy: therapeutic effect after 4-7 days
- Terms: 5-12 days
- Cost of products: 1500-1600 rubles per week
A diet for influenza, acute respiratory viral infections, and colds, which includes drinking plenty of fluids in order to actively rehydrate the patient’s body and normalize sputum and rheological properties of blood (at least 2.5 l/day). For this purpose, it is recommended to consume non-carbonated alkaline mineral waters, purified warm water with honey, rosehip decoction, herbal teas based on sage, thyme, linden, chamomile, raspberry/currant tea, fruit drink (cranberry/lingonberry), compote, infusion of ginger and honey , and in case of severe dehydration - balanced salt solutions. The volume of free fluid consumed during a febrile period should be 150 ml/kg of body weight for children under 3 years of age, and 80 ml/kg after 3 years of age.
The diet should be complete with a high content of vitamins and protein. It is recommended to consume chicken broth, lean meat, and dairy products. Fatty, spicy, salty, fried and pickled foods are subject to restrictions. Small meals up to 6 times a day.
Prevention
Prevention of swine flu is divided into specific (vaccination) and nonspecific.
Specific prevention
It is carried out by vaccinating the population. WHO changes the composition of vaccine strains every year. Depending on the number of viral particles contained, Russian and foreign 3 and 4 quadrivalent vaccines have been developed, which also provide protection against the swine flu virus. A specific immune response is formed over 4 weeks and persists for a year, that is, vaccination must be done annually. Numerous studies confirm the high effectiveness of vaccination in people of any age and is recommended to everyone as a reliable preventive measure. Modern vaccines are low-reactogenic and well tolerated. Anyone can be vaccinated, with the exception of those with contraindications ( bronchial asthma during attacks, allergy to chicken protein, high fever, heart failure, diseases of the blood and endocrine system, children under 6 months). Vaccination is recommended before the start of the flu season (October, November).
Nonspecific chemoprophylaxis
It is effective only in post-contact cases, if no more than 48 hours have passed since the first contact with the patient. Its duration should be at least 7 days after the last contact with the patient. It is especially recommended for unvaccinated individuals at high risk of developing complications. For this purpose, the antiviral agents Umifenovir ( Arbidol ) are used; interferon preparations: interferon gamma ( Ingaron ), interferon alpha ( Alfaron , Reaferon-Lipint and Grippferon ); interferon inducers ( Cycloferon ), Kagocel , Tiloron ( Lavomax , Amiksin ).
Individual methods of prevention
Aimed at breaking the mechanism of transmission of the influenza virus from a sick person to a healthy person and include:
- Avoid direct contact with flu patients (closer than 1.5 meters); during periods of epidemic rise in incidence, avoid crowded places. Use of protective masks.
- Regular ventilation of premises and wet cleaning.
- Regular hand washing with disinfectant/soap, use of disposable towels, avoiding hand contact with public surfaces during epidemic periods.
- Regular toileting of the nasal cavity (rinsing the external parts of the nasal passages with saline solutions).
- Avoiding hand contact with mouth, nose and eyes.
- Regular and thorough cleaning of public surfaces with antiseptic solutions.
How to avoid the new Spanish flu
The high variability and unpredictability of the influenza virus may sooner or later lead to a new pandemic. To avoid this, various measures are being taken - both at the global and local levels. The World Health Organization (WHO) and regional organizations in different countries constantly monitor circulating influenza strains, as the composition of seasonal strains changes year after year, adding new potentially dangerous variants. The variability of influenza viruses is a major challenge for pharmaceutical companies developing antiviral drugs (27 and 57). Thus, the percentage of influenza strains resistant to oseltamivir is currently growing.
Preventive influenza vaccines are improved every year depending on the predominant strains. They are developed either using whole inactivated virions, or based on fragmented viral particles or even individual surface proteins. Typically, vaccines are aimed at preventing infection by both type A and type B viruses (58).
Often the symptoms of the flu (fever, sore throat and muscles, headache) are also caused by other viruses. The causative agents of colds include coronaviruses, rhinoviruses, and adenoviruses (59). Identifying a specific pathogen in such cases is not always advisable, therefore such diseases are often classified as acute respiratory viral infections (ARVI).
Show links
- Webby R., Nature. 2011 Dec 7;480(7376):S4-5.
- Lam T.T., Zhu H. et al., J Virol. 2011 Oct;85(19):10279-85.
- World Health Organization, Fact sheet N°211 2009 Apr
- US Department of Health & Human Services, Federal government website
- Wang Q., Tao E. J., ed., Caister Academic Press (February 1, 2010)
- Girard MP, Tam JS, et al., Vaccine. 2010 Jul 12;28(31):4895-902.
- Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team, et al., N Engl J Med. 2009 Jun 18;360(25):2605-15.
- Noyce JO, Michels H, et al., Appl Environ Microbiol. 2007 Apr;73(8):2748-50.
- Bean B, Moore BM, et al., J Infect Dis. 1982 Jul;146(1):47-51.
- Lowen AC, Mubareka S, et al., PLoS Pathog. 2007 Oct 19;3(10):1470-6.
- Kwan-Gett TS, Baer A, et al., Disaster Med Public Health Prep. 2009 Dec;3 Suppl 2:S109-16.
- Rothberg MB and Haessler SD, Crit Care Med. 2010 Apr;38(4 Suppl):e91-7.
- Beveridge WI, Hist Philos Life Sci. 1993;15(1):23-32.
- Kawaoka Y., ed., Caister Academic Press (March 1, 2006)
- Crane M. and Hyatt A., Viruses. 2011 Nov;3(11):2025-46.
- Li G., Wang N., et al., Am J Trop Med Hyg. 2008 Apr;78(4):675-80.
- Hilleman MR, Vaccine. 2002 Aug 19;20(25-26):3068-87.
- Graham-Rowe D., Nature. 2011 Dec 7;480(7376):S2-3.
- From Wikipedia, the free encyclopedia,
- ViralZone, SIB Swiss Institute of Bioinformatics
- Noda T., Front Microbiol. 2011;2:269
- Nayak DP, Balogun RA, et al., Virus Res. 2009 Aug;143(2):147-61.
- Calder LJ, Wasilewski S, et al., Proc Natl Acad Sci US A. 2010 Jun 8;107(23):10685-90.
- Roberts PC and Compans RW, Proc Natl Acad Sci US A. 1998 May 12;95(10):5746-51.
- Roberts PC, Lamb RA, et al., Virology. 1998 Jan 5;240(1):127-37.
- Moscona A., N Engl J Med. 2005 Sep 29;353(13):1363-73.
- Palmer R., Nature. 2011 Dec 7;480(7376):S9-10.
- Ekiert DC, Kashyap AK, et al., Nature. 2012 Sep 27;489(7417):526-32.
- Feldmann H., Volchkov V.E., et al., Arch Virol Suppl. 1999;15:159-69.
- Magrane M. and the UniProt consortium, P03452 (HEMA_I34A1)
- Chu VC and Whittaker GR, Proc Natl Acad Sci US A. 2004 Dec 28;101(52):18153-8.
- Cross KJ, Langley WA, et al., Protein Pept Lett. 2009;16(7):766-78.
- Magrane M. and the UniProt consortium, P06821 (M2_I34A1)
- Magrane M. and the UniProt consortium, P03468 (NRAM_I34A1)
- Gamblin SJ and Skehel JJ, J Biol Chem. 2010 Sep 10;285(37):28403-9.
- Lew W., Chen X., et al., Curr Med Chem. 2000 Jun;7(6):663-72.
- Bloom JD, Gong LI, et al., Science. 2010 Jun 4;328(5983):1272-5.
- Magrane M. and the UniProt consortium, P03485 (M1_I34A1)
- Nayak DP, Hui EK, et al, Virus Res. 2004 Dec;106(2):147-65.
- Ruigrok RW, Schoehn G, et al., J Mol Biol. 2000 Jun 30;300(1):103-12.
- Ganser-Pornillos BK, Yeager M, et al., Curr Opin Struct Biol. 2008 Apr;18(2):203-17.
- Veit M. and Thaa B., Adv Virol. 2011;2011:370606.
- Hay AJ, Gregory V., et al., Philos Trans R Soc Lond B Biol Sci. 2001 Dec 29;356(1416):1861-70.
- Noda T., Sugita Y., et al., Nat Commun. 2012 Jan 24;3:639.
- Arranz R., Coloma R., et al., Science. 2012 Dec 21;338(6114):1634-7.
- Ng AK, Zhang H, et al., FASEB J. 2008 Oct;22(10):3638-47.
- Ye Q., Krug RM, et al., Nature. 2006 Dec 21;444(7122):1078-82.
- Dias A., Bouvier D., et al., Nature. 2009 Apr 16;458(7240):914-8.
- Sugiyama K., Obayashi E., et al., EMBO J. 2009 Jun 17;28(12):1803-11.
- Compans RW, Content J., et al., J Virol. 1972 October; 10(4): 795–800.
- Magrane M. and the UniProt consortium, P03466 (NCAP_I34A1)
- Fournier E, Moules V, Nucleic Acids Res. 2012 Mar;40(5):2197-209.
- Paquette JS, Fortin JF, et al., J Virol. 1998 Nov;72(11):9329-36.
- Cantin R., Fortin J.F., et al., J Virol. 1997 Mar;71(3):1922-30.
- Saifuddin M., Hedayati T., et al., J Gen Virol. 1997 Aug;78 (Pt 8):1907-11.
- Shaw ML, Stone KL, et al., PLoS Pathog. 2008 Jun 6;4(6):e1000085.
- Thorlund K., Awad T., et al., BMC Infect Dis. 2011 May 19;11:134.
- Schlütter J., Nature. 2011 Nov 7;480(7376):S6-8.
- Mäkelä MJ, Puhakka T, et al., J Clin Microbiol. 1998 Feb;36(2):539-42.
Consequences and complications
Complications of swine flu include primarily primary (viral) pneumonia , which most often develops on the 2-3rd day of illness, often leading to the development of respiratory distress syndrome . A serious complication is secondary pneumonia (pneumococcal, staphylococcal), which develops 6-10 days from the onset of the disease, bacillus, as well as mixed viral-bacterial pneumonia. Less common complications of swine flu also include the development of infectious-allergic pericarditis , myocarditis , meningoencephalitis , hemorrhagic syndrome , respiratory/cardiovascular failure. In addition, swine flu aggravates/exacerbates the course of concomitant chronic somatic diseases, which complicates and prolongs recovery.
List of sources
- Influenza and other respiratory infections: epidemiology, prevention, diagnosis and therapy / Ed. O.I. Kiseleva, I.G. Marinich, A.A. Somina. - St. Petersburg: “Borges”, 2003. – 244 p.
- Kiselev O.I., Tsybalova L.M., Pokrovsky V.I. Influenza: epidemiology, diagnosis, treatment, prevention. M.: Medical Information Agency; 2012.
- Yatsyshina S.B., Minenko A.N., Kushakova T.E. and others. Pandemic influenza A/H1N1(SW2009) in Russia: epidemiology, diagnosis, clinical picture and treatment. Therapeutic archive. 2010; 11:10-14.
- Gorodin V.N., Pronin M.G., Lebedev V.V. Treatment and outcomes of severe forms of influenza A (NS1). In the book: Materials of the 3rd All-Russian Congress on Infectious Diseases. M.; 2011: 87.
- Diagnosis, prevention and treatment of “swine flu” (swine influenze) // letter from Rospotrebnadzor dated April 26, 2009. No. 01 / 5583-9-23.
Why is it especially important to get vaccinated during COVID-19?
If you get a flu shot, you will protect yourself from becoming infected with the dangerous flu viruses that WHO predicts today. The vaccine will not protect you from coronavirus. But those vaccinated against influenza have a better prognosis and a higher chance of coping with complications. More - because the layering of two infections at the same time will be excluded. In addition, both diseases begin with similar symptoms. Having a flu shot will allow your doctor to make a diagnosis faster, ruling out influenza, and prescribe treatment sooner.