Table of contents
- Etiology and pathogenesis
- Clinical manifestations
- Principles of treatment
Hemosiderosis of the skin (post-traumatic hemosiderosis, pigmentary capillaritis, hemorrhagic pigmentary dermatoses, pigmentary purpuric dermatoses) is a condition that occurs after an injury with blood entering the soft tissues (the appearance of a hematoma), or as a result of diseases, the common manifestation of which is the deposition of hemosiderin in the skin.
In our company you can purchase the following equipment for the treatment of skin hemosiderosis:
- M22 (Lumenis)
- IPL Quantum (Lumenis)
Hemosiderin is a dark yellow pigment composed of iron oxide. It is formed during the breakdown of two proteins - hemoglobin and ferritin, for example after blood enters the body's tissues. This can occur after an injury (bruise, injection), when a hematoma forms under the skin. Macrophages do not always have time to utilize the “subcutaneous” blood, as a result of which hemosiderin begins to accumulate in the area of damage. It forms rather persistent local discolorations, which can cause aesthetic discomfort in patients.
The following diseases are also hemosiderosis:
- Pigmented progressive dermatosis of Schamberg
- Annular telangiectatic purpura of Majocchi
- Lichenoid purpuric pigmentary dermatitis Gougerot-Blum
- Favre-Shay ocher dermatitis
- Touraine's arcuate telangiectatic purpura
- Eczematid-like purpura of Doukas-Kapetanakis
- Itchy Leventhal's purpura
- Pigmented purpuric and telangiectatic dermatitis (Purpura senilis)
- Orthostatic purpura
Below we will focus on the most common conditions and pathologies.
Diagnostics
A dermatologist examines the patient, examines the nature of the rash and the presence of characteristic signs. Laboratory tests are required - blood biochemistry with determination of iron levels, general urine tests, PCR tests. The content of sputum and urine is analyzed using a desferal test. To clarify the diagnosis, the affected segments are sent for a biopsy. Histological studies of the skin, bone marrow, lungs, lymphatic tissues, liver, and kidneys help detect pigment deposits. For diagnostic purposes, bronchoscopy with examination of lavage water can be performed, a chest x-ray, MRI, and computed tomography may be performed.
Etiology and pathogenesis
Post-traumatic hemosiderosis
Its appearance is preceded by trauma - bruise, injection, skin incision, etc. As a result, blood enters the soft tissues, where oxidation of hemoglobin and ferritin occurs with subsequent accumulation of hemosiderin. Other causes and predisposing factors are:
- swelling of the lower extremities;
- diabetes;
- diseases of the cardiovascular system;
- high blood pressure;
- venous hypertension;
- chronic venous insufficiency;
- lipodermatosclerosis.
Pigmented progressive dermatosis of Schamberg
First described in 1901 by English dermatologist Jay Frank Schamberg. The main cause of dermatosis is considered to be increased permeability of small vessels and capillaries located near the surface of the skin, through which red blood cells can pass. Once in the tissues, they are destroyed, resulting in the release of hemoglobin from the red blood cells and subsequently iron. It gradually accumulates in a certain area, forming a specific skin tone.
Annular telangiectatic purpura of Majocchi
Described by the Italian dermatologist Dominico Maiocchi at the end of the 19th century. The etiology of the disease is associated with several factors: increased blood pressure, poor circulation in the legs, chronic spasm of small vessels, diapedesis (leakage) of blood cells into the tissue.
Lichenoid purpuric pigmentary dermatitis Gougerot-Blum
Described by dermatologists Henry Gougereau and Paul Bloom in 1925. The exact cause of the disease is unknown; venous hypertension, systemic diseases, infections, blood thinning medications, increased capillary fragility, etc. play a role.
Eczematid-like purpura of Doukas-Kapetanakis
Etiology unknown. Possible participation in the pathogenesis of increased permeability of small vessels with subsequent diapedesis of blood cells.
Clinical manifestations
Post-traumatic hemosiderosis
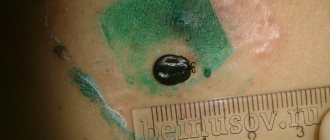
The spots can be of any size and shape, ranging in color from yellow to brown or black. They occur in any area of the body (even around the eyes), but are more common on the lower extremities ( Fig. 1 ).
Pigmented progressive dermatosis of Schamberg
It appears in the form of points of a red-brown or yellow-brown hue with a diameter of several millimeters, which Shamberg himself compared to ground cayenne pepper grains. These points are most often located on the legs, but can also occur on other parts of the body ( Fig. 2 ). The rashes rise somewhat above the surface of the skin and over time can merge into larger irregularly shaped elements. Gradually they turn pale, and in their place foci of skin atrophy form. There are no subjective sensations; in rare cases, there may be slight itching in the affected area.
Annular telangiectatic purpura of Majocchi
Pinkish or reddish spots of irregular shape with a diameter of one to several centimeters appear on the skin. As they grow, the edges of the spots become darker, and the center, on the contrary, becomes lighter ( Fig. 3 ). Gradually, skin atrophy develops in the central part with loss of small hair. There are no subjective sensations.
Lichenoid purpuric pigmentary dermatitis Gougerot-Blum
It is characterized by the appearance of small lichen-like nodules with small rashes among them. There is a point dilatation of small subcutaneous vessels with local darkening of the skin due to hemosiderosis ( Fig. 4A ). Typical localization is in the lower legs, less often on the hips and torso.
Eczematid-like purpura of Doukas-Kapetanakis
Individual petechiae appear on the skin of the legs with a tendency to unite into large spots. At first they are red, but gradually become yellow or brown, fade and may disappear over time. Sometimes the lesions spread to the thighs, trunk and arms ( Fig. 4B,C ). Additionally, the phenomena of parakeratosis, itching and hyperpigmentation are noted.
In table 1 presents the most common hemosideroses and the main differences between them.
Table 1. Differential diagnosis of the most common hemosiderosis of the skin
| Characteristic | Post-traumatic hemosiderosis | Purpura Majocchi | Schamberg's dermatosis | Gougerot-Blum dermatitis | Doukas-Kapetanakis purpura |
| Floor | In both sexes | Usually in women | Usually in men | Usually in men | In both sexes |
| Frequency of occurrence | Often | Rarely | The most common type of hemosiderosis | Rarely | Moderately often |
| Peak incidence | At any age, but as the body ages, the likelihood increases | Children and youth | Teens and young adults | Middle aged people | Children and youth |
| Dynamics of lesions | Lesions arise at the site of previous injury. More often they occur on the legs due to endocrine pathologies, disorders of the venous system and other factors | Lesions first appear symmetrically on the legs, then can spread to the torso and arms | Lesions most often form symmetrically in the shin area, but can also occur on only one leg. The disease may affect the thighs, buttocks, torso or arms | Most often in the lower legs and very rarely in the thighs and torso | On the legs, gradually moving to the hips, torso and arms |
| Clinical manifestations | Spots of various sizes and shapes, colors ranging from yellow to brown or black | Variable numbers of ring-shaped, erythematous plaques and patches, often with central blanching and atrophy | Isolated red-brown spots that do not protrude above the skin and look like grains of ground cayenne pepper | Tiny lichenoid papules with a tendency to unite into large plaques of varying shades | The lesions are usually extensive. Patients complain of severe itching |
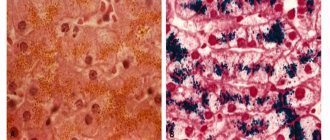
| Histology | Dilation of capillaries in the papillary layer of the dermis, diapedesis, proliferation of capillary endothelium with deposition of hemosiderin in the form of clumps in the interstitial substance, histiocytes, endothelial cells. Slight nonspecific perivascular infiltrate | Perivascular lymphocytic infiltration that extends to the epidermis. Vacuolar changes in the basal layer, spongiosis. Macrophages loaded with hemosiderin are detected, and extravasation of erythrocytes is noted within the lichenoid infiltrate | Perivascular mononuclear infiltration in the upper dermis, swelling of the vascular endothelium. Presence of extravasal erythrocytes and hemosiderin-loaded macrophages | Perivascular lymphocytic infiltration. Lichenoid tissue reaction. Edema of the endothelium and narrowing of the lumen of small vessels | Spongiosis (swelling of the spinous layer of the epidermis) with inflammatory changes |
| Probability of remission | Possible | Possible | Possible | The course is often chronic, but spontaneous remission is possible | Both spontaneous remission and sudden exacerbation of the disease are possible |
| Treatment | Topical corticosteroids, hardware techniques | The disease is congenital and goes away on its own. However, after some time the lesions may appear again | Systemic corticosteroids, antihistamines, vitamin C, PUVA therapy (see below) | Therapy is difficult. Topical and systemic corticosteroids, antihistamines and antipruritics are used. Wearing compression stockings is recommended. Possible use of PUVA therapy (see below), griseofulvin, cyclosporine A, vitamin C and bioflavonoids | Topical corticosteroids and antihistamines |
Rice. 1. Post-traumatic hemosiderosis on the legs (www.healthline.com; Photo: MavCure)
https://i0.wp.com/www.healthline.com
Rice . 2. Chatterjee S. Schamberg disease: uncommon reaction to a common drug. CMAJ 2009; 181(12): E275)
https://www.cmaj.ca
Rice. 3. Annular telangiectatic purpura of Majocchi - in the center of a large lesion, an area of skin lightening is noticeable (Hoesly FJ, et al. Purpura annularis telangiectodes of Majocchi: case report and review of the literature. Int J Dermato 2009; 48(10): 1129–1133)
Rice. 4. Gougerot-Blum dermatitis (A) and Doukas-Kapetanakis purpura (B, C) (Kim DH, et al. Characteristics and clinical manifestations of pigmented purpuric dermatosis. Ann Dermatol 2015; 27: 404–410)
3.Symptoms
The course of idiopathic pulmonary hemosiderosis is usually undulating, chronic, with alternating remissions and exacerbations, expressed to varying degrees. Typical symptoms are hypochromic anemia and respiratory failure, hemoptysis, and in the most severe cases, massive pulmonary hemorrhages. During periods of exacerbation, cough, difficulty breathing, tachycardia, general weakness, sometimes elevated body temperature, chest or abdominal pain are noted. The duration of remissions and crisis exacerbations varies widely (from several hours to several weeks). The disease gradually progresses; in the absence of adequate therapy, the patient’s condition worsens, and the result of increasing cardiopulmonary failure, associated pneumothorax, blockage of the bronchi with coagulated blood, and pulmonary infarction leads to death.
As stated above, pulmonary hemosiderosis is a very difficult disease to diagnose.
The most careful study of the anamnesis, clinical picture, dynamics, heredity, immune-allergic status, a number of biochemical indicators, radiographic data, and the results of functional respiratory tests is necessary. It is also necessary to differentiate idiopathic siderosis from many clinically similar diseases.
About our clinic Chistye Prudy metro station Medintercom page!
Principles of treatment
To date, it is believed that not a single drug has a 100% evidence base for its effectiveness in treating hemosiderosis. Thus, the treatment of these diseases is a problem and a challenge for doctors. However, some hemosiderosis can resolve on its own and then unexpectedly recur.
Corticosteroids are effective in reducing inflammation and suppressing itching in some hemosideroses. Antihistamines inhibit endogenous histamine production and also reduce the feeling of itching in patients.
The administration of griseofulvin, cyclosporine A, vitamin C and bioflavonoids has certain benefits. There is evidence of the positive effect of PUVA therapy (psoralen (P) + ultraviolet A (UVA) = PUVA or PUVA) - irradiation of the skin with ultraviolet light A with preliminary intake of a photosensitizer (psoralen) for greater effectiveness of light exposure.
hardware techniques can be used aimed at selective destruction of the pigment. For local destruction of hemosiderin for aesthetic purposes, IPL therapy can be used: a method in which high-intensity pulsed light destroys the pigment, making it more accessible for evacuation during phagocytosis.
Questions from our users:
- skin hemosiderosis laser treatment
- hemosiderosis of the skin after injections
- hemosiderosis of the skin in adults
- local and general hemosiderosis causes