Publications in the media
Regarding the treatment of this disease, you can contact the Surgical Department No. 2 of the Clinic of Faculty Surgery named after. N.N. Burdenko
Hyperaldosteronism (aldosteronism) is a condition resulting from hypersecretion of aldosterone or a violation of its metabolism. Frequency. 0.5–2% of all cases of arterial hypertension. The predominant age is over 40 years. The predominant gender is female. There are primary and secondary hyperaldosteronism • Primary is a clinical syndrome that occurs with lesions of the adrenal glands and is manifested by arterial hypertension, hypokalemia and low renin levels in the blood serum • Secondary (symptomatic) is caused by causes localized outside the adrenal glands. Renin content is significantly increased.
Etiology • Primary hyperaldosteronism •• Unilateral aldosterone-secreting adenoma (Conn's syndrome) is the most common cause (60%) •• Bilateral zona glomerular hyperplasia of the adrenal cortex (idiopathic aldosteronism) is the second most common cause (34%) •• Bilateral aldosterone-secreting adenoma •• Unilateral aldosterone-secreting carcinoma of the adrenal cortex • Secondary hyperaldosteronism •• Renal artery stenosis •• Malignant hypertension •• Renin-secreting tumors •• Ectopic foci of ACTH secretion •• Bartter's syndrome •• Taking oral contraceptives •• Various conditions accompanied edema (heart failure, liver cirrhosis, nephrotic syndrome), cause ischemia of the cells of the juxtaglomerular apparatus of the kidneys, which leads to the release of renin, which increases the content of angiotensins and aldosterone.
Pathogenesis. Aldosterone increases sodium reabsorption and excretion of potassium and hydrogen ions in the distal renal tubules • Sodium retention causes an increase in blood pressure • Potassium loss leads to muscle weakness, paresthesia, tetany •• Hypokalemia reduces insulin secretion by the pancreas, which reduces carbohydrate tolerance •• Hypokalemia reduces sensitivity of renal tubular receptors to ADH, which leads to polyuria.
Clinical picture • Mild to severe arterial hypertension with a predominant increase in diastolic blood pressure is the dominant sign of the disease • Severe hypokalemia in most cases is accompanied by muscle hypotonicity and cramps, headaches, tachycardia, polydipsia, polyuria and nocturia • Edema is not typical.
Laboratory tests • Hypokalemia in combination with increased excretion of potassium in the urine • Hypernatremia • Hypochloremia (hypochloremic alkalosis) • High concentration of aldosterone in the blood serum and urine, not corrected by drugs. Aldosterone content is determined under standard conditions, because it is influenced by sodium balance, use of diuretics and other factors •• Diuretics and vasodilators are stopped 2 weeks before determination of aldosterone and renin levels •• Sodium loading is carried out to differentiate primary aldosteronism (no suppression with sodium load) from increased aldosterone levels in healthy individuals (suppression with sodium load) • Low renin activity in the blood plasma with primary aldosteronism; in secondary – high • Influence of drugs. Diuretics, estrogens, ACE inhibitors, vasodilators, calcium channel blockers and adrenergic blockers can alter renin secretion • Effect of diseases. Malignant arterial hypertension can lead to hyperreninemia, secondary hyperaldosteronism and hypokalemia.
Special studies • Postural test: record the dynamics of aldosterone secretion caused by a 4-hour stay in an upright position (aldosterone concentration is determined at 8 am and at 12 noon in the afternoon) •• In healthy people and patients with bilateral hyperplasia, the concentrations of renin and angiotensin increase with subsequent increased aldosterone levels •• In patients with unilateral adrenal adenomas, a decrease in aldosterone levels is noted • Trial treatment with spironolactone • CT and MRI can detect adrenal adenomas in 80% of cases. Tomographic sections of the adrenal glands should be made every 3 mm • Angiography of the adrenal vessels • The concentration of aldosterone in blood samples from the adrenal veins obtained by selective catheterization allows us to differentiate the causes of aldosteronism. A unilateral increase in aldosterone levels indicates an adenoma; high concentrations on both sides are characteristic of bilateral hyperplasia.
Differential diagnosis • Diuretic use • Renovascular hypertension • Pheochromocytoma • Renin-secreting tumor • Malignant hypertension • Congenital adrenal hyperplasia • Aldosterone-secreting tumor • Use of GCs in high doses • Excessive consumption of mineralocorticoids or consumption of licorice (licorice root) • Pseudoaldosteronism (Liddle's syndrome).
TREATMENT
Management tactics • Sodium-restricted diet, regular dosed physical activity (set of exercises), optimization of body weight, smoking cessation • Conn's syndrome - unilateral adrenalectomy (correction of hypokalemia with spironolactone is required before surgery) • Idiopathic hyperaldosteronism - long-term drug therapy - potassium-sparing diuretics (spironolactone 25–50 mg 3 times / day) and other antihypertensive drugs (for example, calcium channel blockers, ACE inhibitors, small doses of thiazide diuretics).
Observation • Determination of blood pressure • Determination of serum potassium levels • Determination of urinary aldosterone concentrations within 24 hours after adrenalectomy • All patients with arterial hypertension and hypokalemia of unknown etiology should be examined for aldosteronism.
Drug therapy
Drugs of choice • Spironolactone 75–150 mg/day (to compensate for hypokalemia) • Antihypertensive drugs: calcium channel blockers, ACE inhibitors or thiazide diuretics in small doses • For Bartter's syndrome - potassium-rich foods, nutritional supplements in combination with spironolactone, triamterene, amiloride or propranolol usually reduce the clinical manifestations of the disease, but do not completely prevent potassium loss.
Complications. Cardiac arrhythmias (possibly fatal) associated with severe hypokalemia.
Course and prognosis. Surgical removal of an aldosterone-secreting adenoma leads to the disappearance of arterial hypertension in approximately 70% of cases. Arterial hypertension usually disappears gradually over 1–4 months.
ICD-10 • E26 Hyperaldosteronism
Note. Sodium loading, methods of implementation • Measure the level of aldosterone excretion in 24-hour urine after the patient has taken more than 150 mEq of sodium for at least 3 days (sodium chloride tablets are usually prescribed). Sodium loading may further reduce serum potassium levels, so use caution in case of hypokalemia. Elevated aldosterone levels in 24-hour urine containing more than 150 mEq of sodium indicate primary aldosteronism • Plasma aldosterone levels are measured after infusion of 2,000 ml of 0.9% sodium chloride solution over 4 hours. Normal values are below 8–10 ng%. Contraindications: severe arterial hypertension and congestive heart failure.
Causes and pathogenesis of hyperaldosteronism
The cause of the syndrome is increased secretion of aldosterone, which occurs with the development of aldosteroma, aldosteronoma, cancer or diffuse hyperplasia of the adrenal cortex. In primary hyperaldosteronism, decreased renin activity is observed.
The mechanism of development of the disease is associated with the influence of excess aldosterone on water and electrolyte balance. Reabsorption of sodium ions, water in the renal tubules, as well as increased excretion of potassium ions in the urine contributes to the development of hypervolemia, reduces renin activity, increases the susceptibility of the vessel wall to external pressor factors, and resistance of peripheral vessels to blood flow. This leads to the development of hypertension, suppression of insulin production and decreased glucose tolerance.
Clinical picture
Hypertension is one of the most persistent symptoms of PHA. Hypertension is manifested by headache, dizziness, the appearance of spots before the eyes, etc. The nature of hypertension varies from malignant, resistant to traditional antihypertensive therapy, to moderate and mild, amenable to correction with small doses of antihypertensive drugs (the higher the concentration of aldosterone in the blood, the higher the blood pressure values) . Hypertension can have either a crisis or persistent course. Disorders of neuromuscular conduction and excitability (muscle weakness, paresthesia, convulsions, bradycardia, rarely tetany) are mainly associated with hypokalemia. Due to electrolyte disturbances, the function of the renal tubules changes (thirst, polyuria, nocturia). At the same time, all of the indicated signs of PHA may not be present, and cases of oligosymptomatic or even asymptomatic progression are often observed. The absence of neuromuscular and renal disorders should not be considered as a criterion for excluding PHA.
Diagnosis of hyperaldosteronism
The sooner an endocrinologist can diagnose the disease, the greater the patient’s chances for a successful recovery. To assess the clinical picture, it is necessary to find out the etiological causes of the disease or the underlying disease that led to its appearance. The most effective methods for diagnosing hyperaldosteronism today are the following:
- Blood tests.
- Selective venography.
- Urine tests.
- MRI and CT for the primary form of the disease / ECG, ultrasound, duplex scanning, Doppler ultrasound for the secondary form.
- Scintigraphy.
- Ultrasound sonography.
It is not always possible to make a diagnosis the first time. Therefore, to clarify the diagnosis, doctors often prescribe additional sampling. In this case, diuretics (usually veroshpiron or furosemide) or sodium chloride are used.
Symptoms of secondary hyperaldosteronism
With hyperaldosteronism of the secondary form, one can usually detect a fairly high level of blood pressure, which gradually leads to tissue ischemia and damage to the vascular walls, as well as changes in the fundus (neuroretinopathy, hemorrhages), and deterioration in kidney function. The most characteristic symptom of secondary hyperaldosteronism is edema. Sometimes, (for example, pseudohyperaldosteronism in Barter syndrome), hyperaldosteronism of the secondary form occurs without the presence of arterial hypertension.
The course of hyperaldosteronism may be asymptomatic, but in quite rare cases.
Modern methods of treatment
Treatment must be comprehensive. Specific measures are prescribed depending on the causes of the disease. For secondary hyperaldosteronism, drug treatment is predominantly used with the following drugs:
- Inhibitors of glucocorticoid synthesis.
- Potassium supplements.
- Hormonal means.
- Spironolactone.
- Drugs indicated in the treatment of the primary disease.
Primary hyperaldosteronism is recommended to be treated surgically (resection of the affected adrenal gland). Then restore the body with the help of properly selected drug therapy.
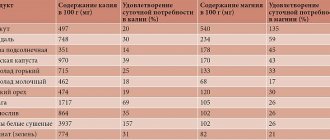
Also, in both cases, the patient is prescribed a diet. It includes low-sodium meals and potassium-rich foods (for example, rice, potatoes, raisins).
If you notice the first symptoms of the disease, do not put off visiting a doctor. Medical specialists use modern diagnostic equipment, and therefore can detect hyperaldosteronism even at an early stage. Make an appointment and get effective treatment.
Etiology
Adrenal aldosteroma is a solitary tumor (adenoma) of the adrenal cortex that secretes aldosterone. About 80% of aldosterones, due to the complete loss of negative feedback between tumor cells and the renin-angiotensin system, produce aldosterone absolutely autonomously, and 20% of adrenal adenomas that secrete aldosterone are sensitive to angiotensin II to varying degrees. A very rare variant (0.3–1%) of solitary adrenal tumor with aldosterone hypersecretion is considered to be aldosterone-producing carcinoma. Due to the low differentiation of the cells of this tumor, they are characterized by resistance to angiotensin II.
Idiopathic hyperaldosteronism.
The morphological substrate of idiopathic hyperaldosteronism is bilateral diffuse nodular hyperplasia. In this form of the disease, adenomatous changes in the adrenal gland can often reach the size of a macroadenoma (>1 cm). The main distinguishing feature of idiopathic hyperaldosteronism from adrenal aldosteroma is the functional dependence of adrenal cortex cells on angiotensin II, even at the lowest values of renin activity in the blood.
Unilateral adrenal hyperplasia is a rare form of PHA. This form of the disease is characterized by unilateral lesions in the absence of adenomatous changes. The pathogenesis of functional changes in unilateral adrenal hyperplasia is unclear.
Glucocorticoid-dependent (glucocorticoid-suppressed) hyperaldosteronism (familial hyperaldosteronism type 1) is detected extremely rarely. This disease is considered hereditary (autosomal dominant inheritance). With it, aldosterone synthesis occurs in the zona fasciculata of the adrenal cortex under the regulatory influence of ACTH, in contrast to other forms of PHA, when aldosterone is synthesized in the zona glomerulosa. In glucocorticoid-dependent hyperaldosteronism, which is resistant to angiotensin II, a clear therapeutic effect is noted after the administration of glucocorticoids.
The syndrome of ectopic aldosterone production is an extremely rare cause of PHA; it occurs when aldosterone-producing tumors are located extra-adrenally (thyroid cancer, ovarian, pancreatic, intestinal tumors, etc.).
The term “low-renin form of arterial hypertension” means an increase in blood pressure, accompanied by low renin activity in the blood and normal aldosterone levels in the absence of changes in the adrenal glands. As with idiopathic hyperaldosteronism, with low-renin system. Probably, the low-renin form of hypertension is the initial stage of idiopathic hyperaldosteronism and has no independent significance.