Chronic lack of iron in the body occurs due to iron deficiency and is characterized by impaired synthesis of hemoglobin, which is contained in red blood cells. The human body receives its first reserves of iron from the mother through the placenta; after birth, iron is replenished through food intake or iron-containing medications. Iron is removed from the body by the urinary and digestive systems, sweat glands and during menstruation in women. About 2 grams of iron are excreted per day, so in order to prevent depletion of reserves, it must be constantly replenished. According to WHO, every 3rd woman and every 6th man in the world suffers from iron deficiency anemia. Pregnant women, children under 3 years of age and teenage girls are at risk.
Causes of iron deficiency anemia (IDA)
- insufficient intake of iron from food: fasting, vegetarianism, or a diet depleted in iron and protein, followed for a long time. In breastfed children, the cause may be iron deficiency anemia of the mother, early transfer to artificial feeding, late introduction of complementary foods
- impaired iron absorption: enteritis (inflammation of the mucous membrane of the small intestine caused by infection or helminthic infestation), gastritis and peptic ulcer of the stomach and duodenum; hereditary diseases (cystic fibrosis and celiac disease); autoimmune damage to the intestinal mucosa and possibly the stomach (Crohn's disease); condition after removal of the stomach and/or duodenum; stomach and intestinal cancer
- chronic blood loss. This is the most basic reason. This includes losses due to: gastric and duodenal ulcers, nonspecific ulcerative colitis, Crohn's disease, hemorrhoids and anal fissures, intestinal polyposis, bleeding from disintegrating tumors of any location and varicose veins of the esophagus; hemorrhagic vasculitis; pulmonary hemorrhages, pulmonary hemosiderosis; chronic pyelonephritis, polycystic disease and cancer of the kidneys and bladder; losses during hemodialysis; uterine fibroids, endometriosis, hyperpolymenorrhea, cervical cancer; nosebleeds
- congenital deficiency of iron in the body (prematurity, birth from multiple pregnancy, severe iron deficiency anemia in the mother, pathological bleeding during pregnancy and childbirth, fetoplacental insufficiency)
- alcoholism (the mucous membrane of the stomach and intestines is damaged, making it difficult to absorb iron)
- use of medications: non-steroidal anti-inflammatory drugs (diclofenac, ibuprofen, aspirin) reduce blood viscosity and can promote bleeding, in addition, these drugs can provoke the occurrence of stomach and duodenal ulcers; antacids (Almagel, Gastal, Rennie) reduce the production of hydrochloric acid, which is necessary for effective absorption of iron; iron-binding drugs (desferal), these drugs bind and remove free iron and iron in ferritin and transferrin, and in case of overdose can lead to iron deficiency states
- donation (with donations more than 4 times a year, iron deficiency develops)
- disruption of transferrin synthesis. Transferrin is an iron transport protein that is synthesized in the liver.
Normal hemoglobin level in the blood: in women – 120-140 g/l, in men – 130-160 g/l
Introduction
Anemia is a global problem: approximately 25–30% of people suffer from this disease, and half of all anemia is caused by iron deficiency [1, 2].
Diagnostic criteria for anemia, according to WHO, are hemoglobin levels below 130 g/l in men of all ages and postmenopausal women, for non-pregnant women of reproductive age less than 120 g/l, for pregnant women - less than 110 g/l. These WHO standards are used by physicians in most countries for professional consistency purposes [3, 4]. According to the degree of severity, according to the level of hemoglobin (Hb), anemia is divided into mild (Hb≥90 g/l), moderate (Hb 90–70 g/l), severe (Hb 69–50 g/l) and extremely severe anemia (<50 g/l) [5, 6].
Iron deficiency anemia (IDA) is an acquired disease that is characterized by a reduced iron content in the blood serum, tissue depots, and bone marrow, resulting in the development of hypochromia and trophic disorders in tissues [7–9]. IDA is one of the most common pathological conditions in the world, and in women of childbearing age it is in first place in terms of occurrence [7].
Clinical manifestations of IDA
Anemic syndrome - occurs due to a decrease in the level of red blood cells and hemoglobin in the blood, reducing the saturation of cells and tissues with oxygen. The signs of anemic syndrome are difficult to recognize, but they help to suspect the presence of anemia and, in combination with the data of other examinations, make a diagnosis. These are general weakness, high fatigue and decreased performance, dizziness, tinnitus and flashing “spots” before the eyes, periodic palpitations, shortness of breath with little physical exertion, and fainting. Upon examination, pallor of the skin and visible mucous membranes, slight swelling of the legs, feet, face (mainly the area around the eyes), tachycardia, various types of arrhythmia, moderate heart murmurs, and muffled heart sounds are revealed.
Sideropenic syndrome - caused by iron deficiency in tissues, which causes a decrease in the activity of many enzymes (protein substances that regulate many vital functions), manifested by numerous symptoms:
- change in taste (desire to eat unusual foods: sand, chalk, clay, tooth powder, ice, as well as raw minced meat, unbaked dough, dry cereals)
- tendency to eat hot, salty, spicy foods
- distortion of the sense of smell (attracted by the smell of gasoline, acetone, the smell of varnishes, paints, lime)
- decreased muscle strength and atrophy
- dry, flaky skin; fragility and hair loss; dullness, transverse striations, spoon-shaped concavity of nails; Minor injuries and abrasions do not heal for a long time
- dryness and cracks in the corners of the mouth in 10-15% of patients
- feeling of tongue fullness, redness and atrophy, frequent periodontal disease and caries
- dryness of the esophageal mucosa, which causes pain when swallowing and difficulty swallowing solid food, the development of atrophic gastritis and enteritis
- urgency to urinate, inability to hold urine when coughing, laughing, sneezing, episodes of bedwetting
- the symptom of “blue sclera” is characterized by a bluish coloration of the sclera
- prolonged increase in body temperature to subfebrile levels (37.0-37.9°C) for no apparent reason
- frequent ARVI
Why does anemia occur?
Causes of anemia:
- metabolic disorders involved in hematopoiesis - iron, vitamins B6 and B-12;
- weakness of the hematopoietic system;
- increasing the body's intake of iron and vitamins;
- blood loss;
- hereditary abnormalities of red blood cells;
- gastrointestinal diseases leading to impaired absorption of microelements and vitamins;
- infections;
- immune pathologies;
- breakdown of red blood cells;
- acute and chronic (occupational) poisoning;
- irradiation
There are conditions that require periodic laboratory testing for anemia:
- chronic pathologies of hematopoiesis, gastrointestinal tract of the heart, liver, kidneys;
- period of pregnancy and lactation;
- hemorrhoids, hypermenorrhea, fibroids and other ailments accompanied by bleeding;
- childhood;
- puberty;
- recent operations or injuries accompanied by significant blood loss;
- professional sports;
- systemic diseases - lupus, rheumatism, vasculitis;
- infections;
- condition after blood transfusion;
- following strict diets;
- undergone radiation and chemotherapy;
- work in hazardous industries.
Diagnosis of IDA
- clinical blood test: decreased level of hemoglobin, red blood cells, decreased hemoglobin content in one red blood cell, often increased ESR
- biochemical blood test: decrease in serum iron level, increase in total iron-binding capacity of serum, decrease in ferritin content in blood serum
If an iron deficiency is detected in the patient’s body using tests, then the next step will be to search for the causes of this deficiency. To identify the cause of iron deficiency, a comprehensive examination is carried out, including esophagogastroduodenoscopy, sigmoidoscopy, colonoscopy, bronchoscopy, chest x-ray, ultrasound examination of the abdominal organs, pelvis and kidneys, examination by a gynecologist, urologist, hematologist, stool analysis for occult blood and eggs. helminths, as well as examination of red bone marrow from the sternum or ilium (sternal puncture, trephine biopsy).
Changes in blood tests due to anemia
To diagnose anemia and determine its type, blood is taken from a finger and a vein. For some types of anemia, a urine test is performed for bile pigments, which are formed as a result of the breakdown of red blood cells and concomitant liver damage.
Determine in blood:
- Red blood cell content and hematocrit;
- Reticulocyte concentration;
- The presence of red blood cells of irregular shape , composition and size;
- Color index (CI) , based on this criterion, anemia is divided into three types: hypochromic - CP is reduced; normochromic - CP is not changed; hyperchromic - the CPU is increased.
- Serum iron concentration . Based on this criterion, anemia is divided into three types: normosideremic - the indicator is normal; hyposideremic – iron concentration is less than normal; hypersideremic – iron content is increased.
- Saturation of blood serum with transferrin , a protein that transports iron, for the formation of red blood cells;
- Leukocyte content . With anemia, both the general indicator and the content of leukocytes of any type (lymphocytes, monocytes, eosinophils, basophils) may change;
- Concentration of bilirubin and haptoglobin;
- Mean erythrocyte diameter (EDD) . Anemia is: normocytic, red cells are normal; microcytic – the size of red blood cells is reduced; macrocytic and megaloblastic - unnaturally large red blood cells are found.
Complications of IDA
Complications arise with prolonged anemia without treatment and reduce the patient’s quality of life: decreased immunity, increased heart rate, which leads to heart failure; in pregnant women, the risk of premature birth and fetal growth retardation increases; in children, iron deficiency causes retarded growth and development; a rare and severe complication is hypoxic coma; hypoxia due to iron deficiency complicates the course of existing cardiopulmonary diseases (coronary artery disease, bronchial asthma, chronic cerebral ischemia, etc.) until the development of emergency conditions, such as acute or repeated myocardial infarction and acute cerebrovascular accident (stroke).
Hemorrhagic anemia
This type of anemia can be acute, resulting from massive blood loss due to surgery, miscarriage, ectopic pregnancy, difficult childbirth. Anemia can be chronic, caused by minor but frequent bleeding.
The erythrocyte content drops to less than 3.5 1012 l; immediately after the loss of a large amount of blood, the indicator can be significantly reduced down to 2.1 1012 l. The hemoglobin content decreases - the lower this indicator, the more severe the anemia.
The average volume of red blood cells decreases. In the blood, the content of underdeveloped or deformed red cells increases, which cannot function properly. The number of immature red blood cells - reticulocytes - increases because red blood cells do not have time to mature.
The number of leukocytes in the blood drops, because with blood loss not only red blood cells are lost, but also white cells.
Treatment of IDA
The basic principles of treatment for iron deficiency anemia include eliminating the cause of iron deficiency, correcting the diet, and replenishing iron deficiency in the body.
- The diet for iron deficiency anemia consists of eating foods rich in iron. Patients are advised to have a nutritious diet with the obligatory inclusion in the diet of foods containing heme iron (veal, beef, lamb, rabbit meat, liver, tongue). Plant foods rich in iron include beans, beans, lentils, peas, spinach, cauliflower, potatoes, carrots, beets, bananas, apricots, peaches, apples, blueberries, raspberries, strawberries, almonds and walnuts. It should be remembered that ascorbic acid, which is found in bell peppers, cabbage, rose hips, currants, citrus fruits, sorrel, enhances the absorption of iron in the gastrointestinal tract, and oxalates and polyphenols (coffee, tea, soy protein, milk, chocolate) worsen the absorption of iron. calcium, dietary fiber and other substances. However, no matter how much meat we eat, only 2.5 mg of iron will enter the bloodstream per day - this is exactly how much the body can absorb. And 15-20 times more is absorbed from iron-containing complexes - that’s why the problem of anemia cannot always be solved with the help of diet alone, and therefore iron-containing drugs are prescribed
- Oral iron supplements differ from other medications by special rules of administration: - short-acting iron-containing preparations are not taken immediately before or during meals. The medicine is taken 15-20 minutes after meals or in the pause between doses; prolonged medications (sorbifer durules, tardiferron-retard, etc.) can be taken before meals and at night (1-2 times a day); - iron supplements are not taken with milk and milk-based drinks (kefir, fermented baked milk, yogurt) - they contain calcium, which will inhibit the absorption of iron - tablets (except for chewable ones), dragees and capsules are not chewed, are swallowed whole and washed down with plenty of water, rosehip decoction or clarified juice without pulp Oral iron supplements (in tablets, drops, syrup, solution) are the initial treatment for mild to moderate anemia; if there is pregnancy, the intake is agreed with an obstetrician-gynecologist. The duration of treatment is 4–8 weeks until hemoglobin levels normalize, then the drug is taken for 4–6 weeks at half the dose. The most commonly prescribed: - sorbifer durules/fenuls 100 mg, 1-2 tablets 1-2 times a day until hemoglobin levels are restored (in pregnant women, for prevention, 1 tablet 1 time a day, for treatment, 1 tablet 2 times a day) - ferretab comp . 1 capsule per day, up to a maximum of 2-3 capsules per day in 2 divided doses, minimum period of use is 4 weeks - maltofer/actiferrin comes in three dosage forms (drops, syrup, tablets), intake 40-120 drops/10-30 ml syrup / 1-3 tablets per day in 1-2 doses - tardiferron 80 mg, 1-2 tablets per day, pregnant women 1 tablet per day, II-III trimester - totema (combined preparation of iron, copper and manganese) 2- 4 ampoules per day, solution diluted in 1 glass of water, taken for 3-6 months - ferlatum 15 ml 1-2 bottles per day in 2 divided doses
- Injectable iron preparations (venofer, likfer, cosmofer, ferrinject) are used exclusively in the hospital (it is necessary to have the ability to provide anti-shock care), contraindicated during pregnancy and lactation
- Hemotransfusion (transfusion of red blood cell-containing blood components) is performed in case of severe anemia, according to strict indications and in a hospital setting.
Iron metabolism
It is known that iron is an important trace element, which is used mainly as a component of heme in erythrocytes for oxygen transport, and is present in smaller quantities in muscles in the form of heme-myoglobin and in the liver in the form of ferritin [10]. Its sufficient level is necessary to maintain physiological homeostasis [11]. However, excess iron levels can lead to cell death through the formation of free radicals and lipid peroxidation of biological membranes, toxic damage to proteins and nucleic acids. It is important that both iron deficiency and overload can have catastrophic consequences for the body, therefore the content of this microelement is strictly regulated [7, 9, 12–14].
The body of a healthy person contains about 3–5 g of iron, most of which, 2100 mg, is found in blood cells and bone marrow. Approximately 2.5 g of this iron is present in hemoglobin for oxygen transport, and another 2 g is stored as ferritin, mainly in the bone marrow, liver and spleen [9]. In the bone marrow, iron is used to form hemoglobin, liver iron is the main reserve of the microelement, and reticuloendothelial cells of the spleen remove old red blood cells. Finally, relatively small amounts of iron (approximately 400 mg) are present in cellular proteins such as myoglobin and cytochromes, and approximately 3–4 mg is bound to transferrin in the circulation [10, 15]. Almost all metabolically active iron is bound to proteins, and free iron ions can be present in extremely low concentrations.
Under natural conditions, no more than 0.05% (<2.5 mg) of the total amount of iron is lost daily due to exfoliating epithelium of the skin and gastrointestinal tract (GIT), as a result of sweating [12, 13, 16, 17]. The processes of absorption, recycling and storage of iron reserves are regulated by a special hormone - hepcidin, which is produced by liver cells. Under physiological conditions, hepcidin production is controlled by a complex interaction of signals, primarily the level of iron in the blood and the degree of oxygenation of liver tissue. Under pathological conditions, its production is regulated by proinflammatory cytokines, of which interleukin-6 plays a major role [7, 12, 13, 18].
Iron deficiency is detected in people of all age and social groups, but more often in women of reproductive age, young children and the elderly [5, 6]. The main reasons for the development of iron deficiency include decreased food intake, decreased absorption and blood loss. In developed, resource-rich countries, adult diets are almost always adequate, and the most common cause of iron deficiency is blood loss [2, 6].
Forecast and prevention of iron deficiency anemia
In most cases, iron deficiency anemia can be successfully corrected. However, if the cause is not addressed, iron deficiency may recur or progress. Iron deficiency anemia in infants and young children can cause delayed psychomotor and intellectual development.
In order to prevent iron deficiency anemia, annual monitoring of clinical blood test parameters, nutritious nutrition with sufficient iron content, and timely elimination of sources of blood loss in the body are necessary. Persons at risk may be advised to take prophylactic iron supplements.
Iron refractory anemia
Iron-refractory (sideroblastnaya, sideroahristicheskaya) anemia occurs due to impaired absorption of iron, which occurs in hereditary pathologies, systemic diseases, metabolic disorders, chronic poisoning, and malignant tumors.
With this disease, the serum iron content in the blood reaches 225-260 µmol/l. The excess is deposited in sideroblasts and siderocytes - cells of the spinal cord, the number of which can reach up to 70%. Formations are formed in the organs - hemosiderosis, consisting of glandular compounds.
Improper iron metabolism interferes with the production of red blood cells, the concentration of which drops to 1.0 • 1012 / l., and hemoglobin can be less than 30 g / l. The color index also decreases
The number of reticulocytes increases. Macrocytes are found in the blood - large immature red blood cells, defective and ugly blood cells.
Hypoplastic anemia
This type of anemia is caused by infections, hereditary pathologies, industrial poisoning, bone marrow depletion, diseases of the immune and endocrine systems, and radiation.
This form of anemia is caused by weakness of hematopoiesis. Blood elements have a normal shape and size, but their quantity is less than normal. Pancytopenia occurs, a condition caused by the death of cells from which red blood cells should be formed. A poor prognostic sign is a decrease in the number of neutrophils below 0.5 • 109/l.
The number of platelets is also reduced, so the blood does not clot well. Analyzes reveal an acceleration of ESR, an increase in the concentration of serum iron and bilirubin.
There is devastation in the cellular contents of the bone marrow caused by inhibition of blood cells.
Iron deficiency conditions in gynecological diseases and methods for their correction
Iron deficiency anemia (IDA) is a hematological syndrome characterized by impaired hemoglobin synthesis due to iron deficiency. Anemia is based on tissue hypoxia, which develops as a result of a decrease in the amount of hemoglobin due to blood loss, impaired formation of red blood cells, their destruction, or a combination of these reasons [1, 2].
Iron deficiency occurs in almost 1/3 of the world's inhabitants, and iron deficiency anemia accounts for 80–90% of all anemias. The prevalence of anemia varies depending on gender, age, climatic-geographical and environmental-industrial causes [1, 3, 4].
A corresponding deficiency develops when iron losses exceed iron intake of 2 mg/day, and is observed in various physiological conditions and diseases [5, 6].
Iron deficiency (hypochromic, microcytic) anemia usually occurs due to a decrease in iron resources in the body due to chronic blood loss or insufficient external iron supply.
The most vulnerable to the development of iron deficiency are women of reproductive age due to monthly physiological blood loss during menstruation, pregnant women due to their high need for microelements, children and adolescents due to the high needs of a growing body, elderly people suffering from chronic diseases and having poor nutrition.
Iron is an essential microelement that plays an important role in the functioning of cells in many body systems, the main of which is the participation of iron in the processes of tissue respiration. The total amount of iron in a woman’s body reaches 2–3 g, and its concentration is 40–50 mg per kg of body weight.
There are two types of iron: heme and non-heme. Heme iron is part of hemoglobin, is found only in meat products, is easily absorbed, and its absorption is practically not affected by the composition of food.
Non-heme iron is found in free ionic form - ferrous or ferric iron. The absorption of non-heme iron (found primarily in vegetables), which accounts for up to 90% of the iron in the total diet, depends on a number of factors. The main part of iron is included in hemoglobin and myoglobin - 70%; iron depot - 18% (intracellular accumulation in the form of ferritin and hemosiderin); functioning iron - 12% (myoglobin and iron-containing enzymes); transported iron - 0.1% (iron bound to transferrin) [7–9].
The most important iron-containing compounds include: hemoproteins, the structural component of which is heme (hemoglobin, myoglobin, cytochromes, catalase, peroxidase), non-heme enzymes (succinate dehydrogenase, acetyl-CoA dehydrogenase, xanthine oxidase), ferritin, hemosiderin, transferrin.
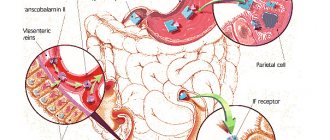
In the mucous membrane of the small intestine, only divalent non-heme iron is absorbed from food. In order for iron to contact proteins and enter the cell, ferric iron is reduced to divalent iron in the presence of an acidic environment; in most cases, ascorbic acid plays the main role in this process [10–13]. Then, to enter the blood plasma and bind to transferrin, iron is again oxidized to trivalent. In the transferrin-bound state, iron is delivered to tissues through endocytosis, where it is either utilized by the cell or deposited in ferritin. Ferritin stores iron in an easily accessible and non-toxic form. Ferritin level is the “gold” standard indicator of the amount of stored iron in the body. Each microgram of ferritin corresponds to 8 mg of deposited iron and for women is normally 15–150 mg/ml [2, 14–16]. The concentration of serum iron is subject to significant daily fluctuations and averages 6.6–26 µmol/l in women. Therefore, its definition is not of paramount importance [2].
Hemoglobin is an oxygen transport protein containing heme iron. The hemes are combined into a protoporphyrin framework, in the center of which there is one divalent iron atom. One hemoglobin molecule can carry a maximum of 4 oxygen molecules. Thus, the number of red blood cells and hemoglobin plays an important role in oxygen transport [2].
During iron deficiency, successive stages are distinguished: latent iron deficiency, in which iron losses exceed iron intake without changes in hemoglobin concentration, and iron deficiency anemia itself, which, depending on the severity, is divided into compensated, subcompensated and decompensated forms [3].
Hemoglobin concentration is expressed in grams per liter. The normal hemoglobin level in women is considered to be 115-145 g/l (MCHC, Mean Corpuscular Hemoglobin Concentration - the average concentration of hemoglobin in a cell is 320-360 g/l); anemia is indicated when hemoglobin decreases below 110 g/l. The severity of anemia is judged by the level of hemoglobin. According to the severity of anemia, there is a mild degree - 90-109 g/l, a moderate degree - 70-89 g/l and a severe degree - less than 70 g/l [3, 14, 15].
In addition, iron deficiency anemia is characterized by a decrease in hematocrit, hypochromia (MCH, Mean Corpuscular Hemoglobin - the average absolute content of hemoglobin in one erythrocyte), microcytosis (MCV, Mean Corpuscular Volume - the average volume of an erythrocyte), hyposiderosis (a decrease in the amount of serum iron, an increase in total iron-binding ability of blood serum, decrease in ferritin level in blood serum and in hemolysate) [3, 5]. The number of red blood cells, hematocrit and hemoglobin constitute the measured values, and MCV, MCH, MCHC are derivatives of these values [2].
The clinical picture of anemia is caused by oxygen starvation of tissues, progressive hemic hypoxia with the subsequent development of secondary metabolic disorders. Clinical symptoms appear as the severity of the disease increases: general weakness, dizziness, headache, palpitations, shortness of breath, fainting, decreased performance, insomnia. Symptoms characteristic of IDA include changes in the skin, nails, hair, muscle weakness, and distortion of the sense of taste. The skin becomes dry and cracks appear on it. Due to impaired carotene metabolism, iron deficiency causes yellowness of the skin. The shape of the nails changes, they flatten, become concave and brittle. Hair becomes thinner, breaks and falls out profusely, and gray hair appears. With IDA, symptoms of damage to the cardiovascular system are also possible: palpitations, shortness of breath, chest pain and sometimes swelling in the legs [6, 14].
The main compensatory mechanisms are circulatory and ventilatory adaptation, including an increase in cardiac output, vasodilation, a decrease in vascular resistance, an increase in tissue perfusion, blood redistribution, an increase in minute volume of respiration, and an increase in erythropoietin activity. Acute, severe and uncompensated anemia can lead to circulatory collapse and shock [2].
The main cause of the development of iron deficiency anemia in women is blood loss of various etiologies. Iron deficiency is 6 times more common in women than in men. A significant amount of blood is lost during menstruation, pregnancy, and childbirth. With heavy menstruation, iron loss of 50–250 mg of iron is possible [2]. Most often, hyperpolymenorrhea is associated with the presence of uterine fibroids, adenomyosis, hyperplastic processes of the endometrium, and dysfunctional uterine bleeding. Metrorrhagia with uterine fibroids is most often associated with submucosal localization of nodes, in which the menstrual surface increases, the permeability of blood vessels supplying the fibroids increases, and the contractility of the uterus decreases. With fibroids, the regeneration of the bleeding surface of the uterus slows down after desquamation of the endometrium. With adenomyosis, the uterine myometrium is affected, which leads to prolonged heavy menstruation and secondary iron deficiency anemia.
Menstrual irregularities occur in women at different ages. Various reasons can lead to the development of hypermenstrual syndrome - severe emotional shocks, malnutrition, vitamin deficiencies, obesity, occupational hazards, infectious and septic diseases, immaturity of hypothalamic structures in puberty and involutive changes in premenopause. In a significant proportion of cases of menometrorrhagia in women, they are accompanied by anemia of varying severity, which contributes to the development of trophic disorders in various organs and tissues. Prevention and treatment of anemia in women with menstrual irregularities and organic gynecological diseases are the most important factors in restoring their health [1, 4, 17].
Regardless of the cause of menometrorrhagia (fibroids, endometriosis, ovarian dysfunction) and the need to influence the corresponding factor, long-term therapy with iron preparations for oral administration is required. The dose, dosage regimen and specific drug are selected individually, taking into account the iron content in the drug, its tolerability, etc.
When choosing a specific drug and the optimal dosage regimen, it is necessary to keep in mind that an adequate increase in hemoglobin levels in the presence of IDA can be ensured by the intake of 30 to 100 mg of ferrous iron into the body [18]. Dietary measures alone cannot compensate for iron deficiency and achieve a therapeutic effect.
Antianemic therapy should be carried out with oral medications and should not be stopped after hemoglobin normalization. Indications for parenteral administration are quite limited: intestinal pathology with malabsorption, intolerance to oral drugs, social reasons (use in patients with personality changes, the mentally ill). According to many studies, parenteral forms do not have advantages over oral ones, and a large number of serious side effects are noted [4, 10, 19]. Blood transfusions for IDA should be carried out only for health reasons.
Modern oral ferrous preparations are salts of ferrous iron (ferric ions are not absorbed in the digestive tract) or compounds consisting of a hydroxide-polymaltose complex of ferric iron (the absorption mechanism differs from that of ionic preparations) [20].
Ferric sulfate salt has the highest bioavailability, therefore ferrous sulfate is mainly contained in ferrous preparations [19, 21]. Ferrous sulfate is the most studied, proven form, which has proven itself with long-term use, therefore it is most often included in preparations for oral administration. It has the highest degree of absorption of all iron preparations.
In the process of absorption of divalent iron in the intestine, ascorbic acid is of great importance, which helps maintain iron in divalent form, so its presence in the preparation is very important [22]. In hematopoiesis, folic acid plays a significant role, enhancing nucleic acid metabolism. For normal folic acid metabolism, cyanocobalamin is necessary, which promotes the formation of its active form. Deficiency of these substances, which often occurs in anemia associated with blood loss, leads to disruption of DNA synthesis in hematopoietic cells, while the inclusion of these components in the drug increases the active absorption of iron in the intestine and its further utilization. The presence of ascorbic and folic acids, as well as cyanocobalamin in the drug significantly increases the rate of hemoglobin synthesis and increases the effectiveness of therapy for iron deficiency conditions and iron deficiency anemia [14, 23, 24].
The listed components that increase the bioavailability of iron are part of the complex antianemic drug Ferro-Folgamma® [24], which was developed and produced in accordance with the recommendations of the World Health Organization (1998).
1 capsule contains 112.6 mg of ferrous sulfate (elemental iron 37 mg), which is the optimal dose for therapy and reduces the incidence of side effects.
Absorption of iron from salt preparations (Fe2+) occurs in the form of passive diffusion according to a concentration gradient, does not depend on pH and motor activity of the gastrointestinal tract (GIT), which ensures rapid saturation.
Ascorbic acid improves the absorption of iron in the intestine, prevents its transition from divalent to trivalent form, accelerates the transport of iron and its inclusion in heme, and also participates in the process of releasing iron from the depot.
Ascorbic acid is necessary for the formation and preservation of the reduced form of folic acid - tetrahydrofolic acid.
In turn, folic acid is an essential factor for the synthesis of DNA and RNA, protein metabolism and the formation of red blood cells, and also acts as an additional stimulator of erythropoiesis and hematopoiesis [21, 23, 25].
Cyanocobolamine is necessary for the formation of hemoglobin, red blood cells, metabolism of proteins, fats, carbohydrates, and energy production.
Ferro-Folgamma® is highly effective, providing an average increase in hemoglobin of 2.5 g/l/day (the highest rate of increase in hemoglobin among ferrous sulfate preparations). When using the drug Ferro-Folgamma®, a weakening of the clinical symptoms of posthemorrhagic anemia is observed during the first 10 days of use [6].
Ferro-Folgamma® is prescribed 1 capsule 3 times a day after meals for 3–4 weeks for mild forms of anemia, for moderate forms — 1 capsule 3 times a day for 8–12 weeks, and for severe forms of anemia — 2 capsules 3 times a day for 16 weeks or more. During pregnancy, it is prescribed to prevent folic acid and iron deficiency, 1 capsule 3 times a day in the II and III trimesters, in the postpartum period during breastfeeding.
After cessation of treatment with Ferro-Folgamma®, the positive effect and stabilization of blood serum parameters (hemoglobin level, red blood cells, serum iron, total iron-binding capacity of blood serum) are guaranteed to persist for at least one month [4].
The active components of Ferro-Folgamma® are in a special neutral shell, which ensures their absorption in the upper part of the small intestine, which eliminates irritating effects on the stomach. The components are dissolved in rapeseed oil, which improves the absorption of iron and at the same time reduces the irritating effect of iron on the gastric mucosa, promoting good tolerability of the drug in the digestive tract [1, 13]. Due to the absence of an aggressive effect on the gastrointestinal mucosa, Ferro-Folgamma® can be successfully used to correct anemic syndrome, with a deficiency of vitamin B12 and folic acid against the background of impaired absorption in the gastrointestinal tract (atrophy of the gastric and duodenal mucosa).
In addition, Ferro-Folgamma® is effectively used for combined iron-folate-B12-deficiency anemia caused by chronic blood loss, chronic alcoholism, infections, taking anticonvulsants and oral contraceptives, anemia during pregnancy and breastfeeding.
The effectiveness of Ferro-Folgamma® for the treatment and prevention of iron deficiency anemia with good tolerability and favorable pharmacoeconomic characteristics (cost/iron dose/efficacy) was proven in several Russian studies that included a wide range of patients, including pregnant women and women with gynecological diseases [4, 18, 19]. Indications for the use of the drug Ferro-Folgamma® are anemia caused by a combined deficiency of iron, folic acid and vitamin B12, occurring against the background of chronic blood loss (menorrhagia and metrorrhagia, etc.), as well as with chronic alcoholism, infectious diseases, taking anticonvulsants and oral contraceptives. The drug is approved for the prevention and treatment of iron and folic acid deficiency in the second and third trimesters of pregnancy, in the postpartum period and during lactation.
Thus, anti-anemic therapy using the drug Ferro-Folgamma® with optimal iron content is highly effective with a rapid increase in hemoglobin (complete clinical and hematological remission in 93% of patients after 3 weeks of therapy). There is good tolerability - the absence of side effects in 95% of patients, allergic reactions and negative effects on the body of women, as well as the stability of the results achieved and the maintenance of a positive effect for a month after treatment, which makes it possible to recommend the drug Ferro-Folgamma® to a wide range of patients.
Literature
- Transcript of the scientific symposium “Iron deficiency conditions in obstetrics and gynecology.” III Russian Forum “Mother and Child”. M., 2001, 29.
- Hook R., Breiman K. Anemia during pregnancy and the postpartum period. M., 2007, 74.
- Gorodetsky V.V., Godulyan O.V. Iron deficiency conditions and iron deficiency anemia: diagnosis and treatment. Guidelines. M.: Medpraktika-M, 2005; 28.
- Konovodova E. N., Dokueva R. S.-E., Yakunina N. A. Iron deficiency conditions in obstetric and gynecological practice // Breast Cancer. 2011; 20: 1228–1231.
- Dolgov V.V., Lugovskaya S.A., Morozova V.T., Pochtar M.E. Laboratory diagnosis of anemia. M., 2001. P. 84.
- Kozlovskaya L.V. Hypochromic anemia: differential diagnosis and treatment // New Med. magazine 1996; 56:8–12.
- Shekhtman M. M. Guide to extragenital pathology in pregnant women. M., 2005, 816, 373–399.
- Johnson-Wimbley TD, Graham DY Diagnosis and management of iron deficiency anemia in the 21st century // Therap. Adv. Gastroenterol. 2011; 4 (3): 177–184.
- UNICEF/UNU/WHO. Iron Deficiency Anemia: Assessment, Prevention, and Control. A Guide for Program Managers. Geneva: WHO/NHD, 2001.
- Arkadyeva G.V. Diagnosis and treatment of iron deficiency conditions. Educational and methodological manual. M.: 1999: 22–25.
- Burlev V. A., Gasparov A. S. et al. Epocrine in the treatment of iron deficiency anemia in patients with uterine fibroids after hysterectomy // Problems of reproduction. 2003; 6:59–64.
- Kasabulatov N.M. Iron deficiency anemia in pregnant women // Breast cancer. 2003; 11, 1: 18–20.
- Lebedev V. A., Pashkov V. M. Principles of treatment of iron deficiency anemia in gynecological patients // Difficult patient. 2013, 11, 11: 3–7.
- Dvoretsky L.I., Zaspa E.A. Iron deficiency anemia in the practice of an obstetrician-gynecologist // Breastfeeding. 2008; 29.
- Kazyukova T.V., Samsygina G.A., Kalashnikova G.V. et al. New possibilities of ferrotherapy for iron deficiency anemia // Klin. pharmacology and therapy. 2000; No. 9 (2): 88–91.
- Pasricha SR, Flecknoe-Brown SC, Allen KJ et al. Diagnosis and management of iron deficiency anemia: a clinical update // Med. J. Aust. 2010; 193(9):525–532.
- Fernandez-Gaxiola AC, De-Regil LM Intermittent iron supplementation for reducing anemia and its associated impairments in menstruating women // Cochrane Database Syst. Rev. 2011. 12. CD009218.
- Burlev V.A., Konovodova E.N., Ordzhonikidze N.V., Serov V.N., Elohina T.B., Ilyasova N.A. Treatment of latent iron deficiency and iron deficiency anemia in pregnant women // Russian Bulletin of Obstetrics- gynecologist. 2006. No. 1. P. 64–68.
- Vertkin A.L., Godulyan O.V., Gorodetsky V.V., Skotnikov A.S. Iron deficiency anemia and the choice of drug for its correction // Russian Medical Journal. 2010. No. 5.
- Gratsianskaya A.N. Iron deficiency anemia: Ferro-Folgamma // Breast cancer. 2013; No. 29.
- Arvas A., Gur E. Are ferric compounds useful in the treatment of iron deficiency anemia? // Turk J Pediatr. 2000. Vol. 42(4). R. 352–354.
- Teucher B., Olivares M., Cori H. Enhancers of iron absorption: ascorbic acid and other organic acids // Int J Vitam Nutr Res. 2004. Vol. 74(6). R. 403–419.
- Konovodova E. N., Burlev V. A. Ferro-Folgamma + Erythropoietin - new possibilities for the treatment of anemia in patients with uterine fibroids // Farmateka. 2004. No. 15 (92). pp. 70–73.
- Ferro-Folgamma. Therapy with iron, folic acid, vitamin B12 and ascorbic acid. Scientific review. Werwag Pharma. M., 2001.
- Ghinea MM Treatment of iron deficiency anemia with Ferro-Folgamma // Rom J Intern Med. 2004. Vol. 42(1). R. 225–230.
A. Z. Khashukoeva1, Doctor of Medical Sciences, Professor S. A. Khlynova, Candidate of Medical Sciences M. V. Burdenko, Candidate of Medical Sciences M. R. Narimanova O. V. Kozlova, Candidate of Medical Sciences, Associate Professor
GBOU VPO RNIMU im. N. I. Pirogova Ministry of Health of the Russian Federation, Moscow
1 Contact information
Abstract. The role of Ferrum in the human organism has been analyzed, mechanisms of its digestion from food, clinical presentations of hypoferric conditions and women's hypoferric anemia, as well as approaches to therapy and prophylaxis of hypoferric anemia with modern oral preparations.