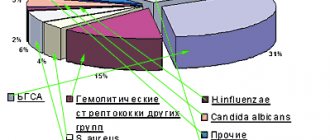
CT diagnostic method for detecting pulmonary fibrosis
Fibrosis is the proliferation of connective tissue with the appearance of scars due to disruption of the healing mechanisms of the wound surface.
When healing does not proceed properly, scarring can occur, causing the organ to fail to function fully.
Accordingly, pulmonary fibrosis is scarring of the lung tissue. The number of cells capable of saturating the blood with oxygen decreases. Consequently, respiratory efficiency decreases - respiratory failure develops, leading to intoxication, first during exercise, as the disease worsens - at rest, and then even during sleep. Scar tissue in the lungs not only has reduced functional properties, but also serves as an excellent environment for the development of associated infections, for example, bacterial (pneumococcal or staphylococcal) pneumonia.
Pulmonary fibrosis is the outcome of tissue inflammation during interstitial (that is, damage to the intercellular connective tissue) lung disease. The reasons for the development of such a disease may include lung injuries, high environmental pollution, smoking, inhalation of drugs, mold, organic, asbestos, quartz and coal dust, infectious, autoimmune, viral diseases and their complications - bronchitis, tuberculosis, pneumonia, COVID- 19 and much more.
Until recently, pneumofibrosis was synonymous with interstitial diseases themselves, but, fortunately, it was found that not all variants of such lung diseases are fibrosing.
The most complex and practically untreatable is primary or idiopathic pulmonary fibrosis - a rapidly progressive fibrosing disease of the lungs, the cause of which is unknown.
Symptoms of pulmonary fibrosis
Pulmonary fibrosis is characterized by symptoms of shortness of breath and dry cough (rarely productive - with sputum) during physical activity, persistent pain in the chest area, fatigue due to difficulty breathing, weight loss without changing the diet. When auscultating the lungs (listening with a phonendoscope), early (in the inhalation phase) inspiratory wheezing is detected, that is, respiratory wheezing, most often localized in the lower posterior zones of the lungs.
Fibrosis can develop in one lung or in two at the same time. Focal and total forms of fibrosis are also possible. In the total form, surgical intervention is often required, since most of the lungs are affected. In the focal form, changes are local in nature.
CT diagnosis of pulmonary fibrosis
The gold standard for diagnosing pulmonary fibrosis is high-resolution computed tomography. CT diagnostics of pulmonary fibrosis allows one to reliably identify the degree of lung damage and determine the localization of scar tissue. This diagnostic method is recognized as one of the most sensitive non-invasive methods for detecting pulmonary fibrosis. Thus, comparative studies conducted already in 1990 showed that pulmonary fibrosis using high-resolution computed tomography (HRCT) was detected in 91% of cases and only in 39% using chest radiography.
In the presence of pulmonary fibrosis in a serious stage, a CT scan shows a pattern (a term adopted to denote pathological signs in medicine) of the so-called “honeycomb” lung - this condition is visible on scans as cysts of the same type, located in several rows, containing air, in the affected parts of one or both lungs. In the early stages of pulmonary fibrosis, a similar picture is not observed, so it was necessary to search for signs on CT that would allow identifying the disease at its onset. One of these signs was the presence of a “frosted glass” pattern in the images—foci of slight compaction of the lung tissue. Also, specific signs of fibrosis in a patient can be detected by performing a CT scan of the lungs with functional tests. Thus, one of the signs—subpleural enhancement of the peripheral pulmonary interstitium—was previously considered a sign of the absence of pathology. Such changes are almost impossible to track using other hardware diagnostic methods.
At the moment, the accuracy of CT diagnostic methods is increasing due to the introduction of new research protocols and careful study of the results of numerous studies. In this case, the leading role in the diagnostic process is given to the radiologist, who interprets visible changes as pulmonary fibrosis or its absence. Finding early radiation signs of fibrosing lung disease is key to timely initiation of antifibrotic therapy.
Also, when a diagnosis is made, multislice CT is used to assess the rate of disease progression, identify favorable and unfavorable types of fibrotic changes, the success of treatment and the correct selection of therapeutic drugs.
Current approaches in the treatment of idiopathic pulmonary fibrosis
Carrying out X-ray morphological comparisons and studying the features of the pathogenesis of IPF made it possible to identify its distinctive features from other interstitial lung diseases (ILD). Identification of signs of usual interstitial pneumonia (UIP) on a computed tomography scan or in a lung biopsy in the absence of known causes and factors associated with damage to the pulmonary interstitium formed the basis for the diagnosis of IPF. However, to date, the problem of phenotyping IPF has not lost its relevance. As it turned out, the severity of the disease, assessed by the rate of progression of pulmonary dysfunction, is not determined solely by CT data, which are used to diagnose IPF, and the high (more than 50%) percentage of unscreened patients in a number of international RCTs indicates that this pathology is very similar to other pathologies. IZL.
The results of studying the mechanisms of fibrosis formation in lung tissue in IPF allowed us to formulate the concept of the development of fibrosis as a consequence of dysfunction of the alveolar epithelium, which occurred spontaneously or resulted from damage by an unknown agent. Disruption of the repair process of the epithelium (probably also of the vascular endothelium) during the persistence of the damaging mechanism is accompanied by the migration of myofibroblasts into the alveolar tissue that has lost its regenerative ability, an increase in their local number, an increase in the synthesis of extracellular matrix components and its deposition into the lung tissue, which ultimately leads to its irreversible remodeling.
Despite numerous studies, it is not possible to explain the occurrence of IPF in a particular patient and significant differences in the rate of progression of IPF in different patients (except in cases of genetically determined pathology), which confirms the concept of the existence of various diseases united under the single term IPF.
The short life expectancy of patients with IPF (the median survival from the moment of diagnosis is 2–3 years, and the 5-year survival rate does not exceed 50%) and the ineffectiveness of anti-inflammatory and immunosuppressive therapy have led to the attitude towards this disease as a potentially fatal and resistant to therapeutic treatment, while a greater or lesser positive effect of glucocorticosteroids and immunomodulatory therapy (azathioprine, methotrexate, cyclophosphamide, cyclosporine, rituximab, mycophenolate mofetil) is observed in other ILDs. However, the issue of the balance between the benefits and risks of using immunomodulatory drugs in ILD has not been resolved; their use in these diseases is not approved in most countries of the world and remains a subject of debate.
The appearance in 2014 of data from a study of the effectiveness of nintedanib and pirfenidone in patients with IPF proved the possibility of drug effects on its pathogenetic mechanisms and marked the beginning of a new period in the study of this pathology. The protein kinase inhibitor nintedanib demonstrated clinical efficacy in IPF in the INPULSIS and INPULSIS ON studies, significantly reducing the rate of FVC loss, the frequency of exacerbations of the disease, and reducing the risk of death from respiratory causes during treatment. Nintedanib is currently approved for the treatment of IPF.
Its antifibrotic effect is realized at the level of receptors for fibroblast growth factor, as well as platelet and vascular endothelial growth factors and consists of reducing the synthesis of profibrotic cytokines, limiting the possibility of transforming fibroblasts into myofibroblasts, suppressing their migration into the alveolar interstitium and the production of extracellular matrix components.
Data from the conducted studies allow us to assert that there are differences in the clinical and radiological manifestations of IPF, the rate of disease progression and response to treatment in different patients, which determines the relevance of the search for biomarkers for grouping IPF patients according to their sensitivity to one or another “targeted” therapy. This problem has not yet been solved and requires more data, which to date have been obtained mainly from retrospective studies conducted on small groups of patients. In addition, biomarkers common to IPF may exist in other chronic ILDs.
A picture of progressive pulmonary fibrosis with the development of severe respiratory failure, resistance to immunomodulatory therapy and low life expectancy is observed in a number of patients with hypersensitivity pneumonitis (HP), idiopathic nonspecific interstitial pneumonia (NSIP), as well as with lung damage in patients with scleroderma, rheumatoid arthritis, interstitial pneumonia with autoimmune manifestations, changes on CT scans in which correspond to the picture of AIP.
There is a similar relationship between the rate of decline in FVC and the mortality rate in IPF, HP, lung damage in systemic scleroderma and rheumatoid arthritis. Disturbances in the structure and function of the alveolar epithelium, which are characteristic of IPF, were found in severe cases of chronic HP, pulmonary sarcoidosis, NSIP, as well as ILD associated with diffuse connective tissue diseases. Thus, the processes of fibrosis formation in these essentially different diseases proceed (at least at certain stages of their development) according to a similar scenario. The data obtained provide grounds for identifying a “progressive fibrotic phenotype” of ILD, which implies the presence of pulmonary fibrosis as a component of a complex pathogenetic process that exists regardless of the initial trigger factors and has the ability to self-maintain, progress and determine the severity and prognosis of the disease.
The question of the advisability of changing the existing nomenclature of ILD and the place of IPF in it is currently being discussed by leading world experts. Combining diseases that differ in etiopathogenetic characteristics into a common “progressive fibrotic phenotype” requires the search for biomarkers that reflect the mechanisms of development of pulmonary fibrosis, and may be relevant in light of the possibility of targeted therapy that modifies the course of the disease. In this regard, the use of nintedanib, which has proven its effectiveness in IPF, may be promising in other ILDs that occur with severe pulmonary fibrosis.
In order to evaluate new treatment options for fibrosing ILD, multicenter, double-blind, placebo-controlled, phase III clinical trials of the efficacy and safety of nintedanib were initiated: SENSCIS and INBUILD. Patients with IPF were not included in these studies. The SENSCIS trial, launched in 2015, examined the effects of nintedanib treatment in patients with systemic scleroderma with pulmonary involvement. The rate of disease progression was assessed by changes in FVC, as well as the dynamics of skin manifestations of systemic scleroderma and quality of life indicators. The study is expected to be completed by the end of 2021. The INBUILD study, launched in 2021, aims to study the efficacy and safety of nintedanib in patients with pulmonary manifestations of systemic connective tissue diseases (rheumatoid arthritis, systemic scleroderma, mixed connective tissue disease), as well as patients with HP, NSIP, unclassified pulmonary fibrosis, sarcoidosis lungs, pneumoconiosis, asbestosis and other fibrosing ILDs, in which changes on CT correspond to AIP or AIP without signs of “honeycomb lung”. The progressive nature of pulmonary fibrosis in this study was assessed using universal criteria for all included entities: a decrease in FVC of 5–10% over 24 months, an increase in the severity of signs of pulmonary fibrosis on CT, and worsening dyspnea. The hypothesis put forward by the researchers is that the effectiveness of nintedanib in fibrosing ILD is comparable to that in patients with IPF, in particular, the slowdown in FVC loss per year of treatment can be 50%.
It remains to be assumed that if the effectiveness and safety of nintedanib, previously proven in IPF, is established in the course of these studies, there will be additional grounds for identifying a single fibrotic phenotype of ILD, and the medical community will be able to reasonably use nintedanib for the pathogenetic therapy of progressive pulmonary fibrosis in patients with various IZL.
Idiopathic pulmonary fibrosis (IPF), which morphologically corresponds to common interstitial pneumonia (IP), can claim to be one of the most prognostically unfavorable variants of interstitial pulmonary lesions, which is characterized by a rapid rate of formation of practically irreversible PF with severe respiratory failure and pulmonary hypertension. The treatment tactics for IPF remain predominantly pathogenetic, not fundamentally different from those used for other IP; Moreover, its features are largely determined by the individual experience of a particular clinical center. In this regard, the importance of consensus recommendations of a number of professional societies published in 2011 can hardly be overestimated from the point of view of the high relevance of attempts to unify the tactics of managing IPF. The difficulty of implementing these efforts in practice is understandable, especially given the clear lack of clinical studies involving patients with IPF that would be conducted taking into account the standards of evidence-based medicine.
The 2011 guidelines defined IPF as a specific form of chronic progressive fibrosing PV of unknown origin, observed primarily among adults, especially the elderly, and without features of a systemic disease. The diagnosis of IPF requires the mandatory exclusion of the provoking role of known etiological factors of interstitial lung diseases (for example, occupational ones), and the presence of characteristic signs of ordinary IP, recorded with high-resolution computed tomography (CT). It is recognized that the accuracy of the diagnosis of IPF increases with a lung biopsy (preferably surgical, but not transbronchial), and the course of the disease, as a rule, is characterized by steady progression: only in a small part of patients the pulmonary process stabilizes, but repeated exacerbations are possible. It should be emphasized that IPF should certainly be considered as one of the most unfavorable variants of interstitial lung diseases: it is in patients suffering from it that the rate of formation of irreversible PF is maximum up to the stage of honeycomb lung and severe chronic respiratory failure. The mentioned features of the clinical evolution of IPF are largely related to the expression profile of inflammatory cytokines and chemokines in the lung tissue, typical for this disease: in comparison with other forms of PV, it is in IPF that the expression of transforming growth factor-β is maximum [3].
Features of the expression of mediators of inflammation and fibrosis, as well as existing descriptions of familial cases of IPF [4], make it necessary to discuss the contribution of genetic determinants to its development. At the same time, it is already obvious today that IPF is not a monogenic disease; it will not be possible to identify those genetic determinants that would clearly form a predisposition to the disease and/or modulate its development in a significant proportion of patients. Repeated attempts have been made to demonstrate the contribution of polymorphisms of individual genes to the progression of IPF. It has been demonstrated that in smokers suffering from IPF, the TT755 variant of the matrix metalloproteinase-1 gene, detected on fibroblasts, is significantly more common [5]. A recently published meta-analysis by NM Korthagen et al. (2012) [6] showed the significance of individual variants of the gene encoding the interleukin-1 receptor antagonist protein as a risk factor for IPF. An association of IPF with carriage of the 308A allele of the tumor necrosis factor α gene in both hetero- (the probability increases by 2.9 times) and homozygous (the probability increases by 13.9 times) form has also been shown [7]. G6A polymorphism of the angiotensinogen gene, as demonstrated by M. Molina-Molina et al. (2008) [8], may influence the course of IPF, in particular the severity of respiratory disorders, but not the formation of a predisposition to it. The intense progression of IPF may also be reflected by the maximum expression of matrix metalloproteinase-9 by cells from broncho-alveolar lavage [9]. Comparison of the genetic “portrait” of lung tissue obtained by biopsy in patients with IPF and pneumonitis caused by hypersensitivity reactions showed that IPF is characterized by predominant expression of genes for tissue remodeling, proliferation of epithelial cells and fibroblasts, while hypersensitivity is characterized by predominant expression of inflammatory genes and activation of T lymphocytes [10]. Overall, the 2011 guidelines emphasize that IPF should not be considered a genetically determined disease. At the same time, further search for certain genetic determinants of the development and progression of the disease is obviously justified, since it allows us to get closer to understanding the pathogenetic features of IPF, which in the future could become the target of specially developed targeted therapeutic strategies.
The 2011 guidelines discuss in detail the importance of other potential etiological factors for IPF, which are of interest primarily in the implementation of appropriate treatments. Among them, smoking is of particular importance. Back in the early 1990s. H. de Cremoux et al. (1990) [11] demonstrated that IPF patients who smoked were characterized by a predominance of lymphocytes in the broncho-alveolar lavage fluid, a worse response to glucocorticosteroids and worse survival. It has also been established that smokers suffering from IPF have the most severe respiratory disorders [12]. A multicenter clinical study that included 248 patients with IPF showed that smoking is associated with a significant 1.6-fold increase in the risk of developing IPF. Former smokers were also characterized by an increased risk of IPF (odds ratio – 1.9), with the highest risk in smokers with 21 to 40 pack years of experience (odds ratio – 2.3) [13]. It has also been established that smokers, including former smokers, who have IPF, have significantly worse survival [14]. It can be argued that all patients with IPF should use all possible means of treating nicotine dependence, although smoking is not an obligate risk factor for IPF.
Among the possible determinants of IPF, various environmental factors are also named, including metal dust (copper, steel, lead) [15]. Organic dust can also be considered as potential factors for the development of IPF: there are known cases of IPF development among agricultural workers, poultry farmers, and livestock farmers [16]. However, from an epidemiological point of view, the connection between IPF and environmental factors has not yet been convincingly confirmed, and each specific patient in whom such a connection is suspected needs a particularly detailed examination and discussion, obviously by a council of specialists. Interpretation of the role of exogenous factors in the development of IPF must be very cautious, especially when the patient's occupational history is used as part of the evidence.
Various infectious agents are also discussed as provocateurs for the development of IPF, primarily viruses: Epstein–Barr, cytomegalovirus, herpes viruses type 7 and 8 [17, 18]. At the same time, despite the fact that the DNA of these viruses could be detected, including in samples of lung tissue obtained by biopsy, the frequency of their detection in general does not differ from that in patients with interstitial pulmonary processes of a different nature. In this regard, the importance of the vast majority of viruses, including Epstein-Barr and representatives of the herpes group, which are credited with a role in the development of many variants of immunopathological lesions of internal organs, in particular systemic diseases, as risk factors for IPF should not be exaggerated, especially unreasonably carrying out antiviral therapy in this category of patients.
Chronic HCV infection is considered one of the most realistic risk factors for IPF [19], although the frequency of its detection in this category of patients, according to various clinical studies, varies significantly. In the first half of the 1990s. T. Ueda et al. (1992) [20] demonstrated that, in comparison with healthy representatives of the control group, the presence of anti-HCV antibodies in the blood serum of patients with IPF can be detected almost 8 times more often. A study of native Italians with IPF showed that the presence of antibodies to HCV could be detected in 13.3% of them, only in 0.3% of blood donors and in 6.1% of patients suffering from other interstitial lung diseases, but not IPF [21]. There are indications that HCV infection is not only more common among patients with IPF, but may also be considered a risk factor for its development. Y. Arase et al. (2008) [22] observed a group of 6150 patients with HCV infection and 2050 patients with HBV infection, the average follow-up duration was 8.0 ± 5.9 for HCV-infected and 6.3 ± 5.5 years for HBV-infected . During the observation period, IPF developed in 15 HCV-infected patients and in none of the HBV-infected patients. The total incidence of IPF in the presence of HCV infection was 0.3% by the 10th year of observation and 0.9% by the 20th year. IPF, therefore, developed significantly more often among HCV-infected people compared to HBV-infected people. Risk factors for IPF in persons with chronic HCV infection included age ≥ 55 years, heavy smoking, or the presence of liver cirrhosis. It should be emphasized that the development of IPF during HCV infection can be associated with cryoglobulinemia and typical damage to internal organs: there are reports of the effectiveness of antiviral therapy (interferon-alpha) in this situation [23]. Apparently, each case of IPF associated with HCV infection should, at least initially, be considered as its extrahepatic manifestation; However, in such patients, the effectiveness of antiviral therapy in terms of the effect on the pulmonary process has not been established and for them, as a rule, glucocorticosteroids and cytostatics have to be used.
Recommendations of the 2011 version consider gastroesophageal reflux (GER) as one of the priority risk factors for IPF. It is believed that microaspirations of aggressive gastric contents observed with it can cause combined chemical, immunological and bacterial damage to the lungs, resulting in the formation of IPF [24]. According to some data [25], GER can be detected in the vast majority of patients with IPF, and it is in them that it reaches its maximum severity. GER can be detected in 65% of patients with IPF who are candidates for lung transplantation. In general, today we can say that treatment of GER is justified for all patients with IPF, since, although not being the main therapeutic approach, it can still help improve the prognosis. JS Lee et al. (2011) [26] recently published the results of an analysis of the effect of GER and its therapy on the survival of patients with IPF. A total of 204 patients were analyzed, of which 34% had complaints characteristic of GER, 45% had a confirmed history of GER, and 47% were taking medications for GER. It turned out that taking medications used to treat GER is associated with an increase in survival of patients with IPF and a decrease in the area of the LF assessed on CT. It is obvious that examination aimed at identifying GER and its most active treatment are justified for all patients with IPF.
The 2011 guidelines clearly state the diagnostic criteria for IPF:
• absence of possible causes of IPF (exogenous factors, including occupational, systemic diseases, medications);
• the presence of signs of conventional PV on high-resolution computed tomograms (a sufficient sign for those who have not undergone a lung biopsy);
• the presence of signs of conventional IP on high-resolution CT and characteristic morphological features in lung tissue samples obtained through surgical biopsy.
It is fundamentally important that this version of the recommendations clearly postulates that IPF is not only a clinical diagnosis and its confirmation requires the mandatory use of CT, and, if possible, surgical (but not transbronchial) lung biopsy. It should, however, be emphasized that justification for the use of these methods is impossible without a thorough analysis of the details of the anamnesis of the pulmonary process and the correct interpretation of the data obtained during a general clinical examination. In general, IPF is often diagnosed late, and the prescription of pathogenetic therapy is often preceded by several (at least 1.5) years of repeated courses of various antibacterial drugs [3], used for imaginary “chronic” bacterial pneumonia. IPF must be assumed always when, during auscultation of the lungs, the only additional phenomenon heard is crepitus, especially bilateral and spreading, without being replaced by moist rales, typical of the involvement of the walls of small bronchi in the inflammatory infiltration of the walls of small bronchi, which is characteristic of true bacterial pneumonia. Fever and other general symptoms of intoxication characteristic of pneumonia are usually absent in IPF: progressive respiratory failure comes to the fore in the clinical picture. In such patients, one should always first exclude interstitial lung diseases, in particular IPF, and long-term therapy with antibacterial drugs is harmful to them both from the point of view of a dramatic increase in the risk of adverse events, and due to the fact that more effective ones are not used. methods of pathogenetic therapy.
In general, today we can say that the use of high-resolution CT and surgical (including transthoracic) lung biopsy makes it possible to clearly confirm IPF in the majority of patients who actually suffer from this disease. The features of IPF that should be screened for by these diagnostic methods are defined in the 2011 guidelines (see table).
In contrast to diagnostic tactics for IPF, treatment tactics for this disease are still far from ideal, primarily because controlled clinical trials have not been able to confirm the effect of the therapeutic strategies most often used in routine clinical practice. The recommendations of the 2011 version recognize the use of glucocorticosteroids, most cytostatics (cyclophosphamide, azathioprine), cyclosporine, interferon-gamma-1, acetylcysteine and anticoagulants in monotherapy and in combinations in the treatment of IPF as inappropriate. Unfortunately, it is not yet possible to talk about the validity of the use of those drugs that are considered promising (etanercept, bosentan, which would be especially justified given the presence of pulmonary hypertension in the majority of patients with IPF), including the antifibrotic agent pirfenidone, which , according to individual clinical studies [26], has a positive effect on respiratory function and survival of patients with IPF. The discussion of sildenafil (its target of action is the same as that of the previously mentioned endothelin-1 antagonist bosentan) and imatinib mesylate in the 2011 recommendations did not lead to a statement of the advisability or inappropriateness of their use. Indications for starting long-term oxygen therapy are recommended to be determined individually. Lung transplantation is considered the preferred treatment for IPF, which has shown a positive effect on prognosis [27]. However, this section of the recommendations should not be accepted unconditionally, and in patients with IPF, especially with relatively early diagnosis, the tactics of immunosuppressive therapy can be active, including the use of glucocorticosteroids and cytostatics (for example, cyclophosphamide), including in ultra-high doses. Passively waiting for the development of indications for lung transplantation is unacceptable, including taking into account the low availability of this intervention in our country.
Of course, the 2011 version of the IPF recommendations is an important step forward towards developing consensus among experts regarding the management of this disease. Risk factors and approaches to diagnosing IPF are currently generally beyond doubt; The interdisciplinary approach to the management of IPF proposed by the expert committee is also key. The difficulties in determining therapeutic strategies and the lack of clear evidence of the effectiveness of most currently used drugs should stimulate new controlled clinical trials.
What is liver fibrosis
Liver fibrosis is scarring of the tissue.
The liver is capable of healing itself, however, this system does not work at full capacity if the liver is damaged or the injury is long-term and very serious. All attempts at regeneration cause an accumulation of connective tissue (these are tough, inert fibers) instead of functioning liver cells. Liver fibrosis is not a specific disease, but rather a symptom of another liver problem. The most common conditions that lead to liver fibrosis are alcoholism, chronic hepatitis C and non-alcoholic fatty liver disease (NAFLD).
Liver fibrosis itself does not cause any symptoms. Doctors can detect signs of liver fibrosis using blood tests and an ultrasound, CT scan, or MRI. If it is detected early, it can be treated. But if it goes undetected and damage continues, fibrosis can progress to cirrhosis.
Degrees of liver fibrosis in adults
Experts distinguish 5 degrees of scarring of liver tissue.
No fibrosis.
In this case, there is no evidence of liver cell death (necrosis) or scarring, despite liver inflammation (hepatitis).
Portal (mild) fibrosis.
In this case, there are areas of necrosis and scarring affecting the small and medium branches of the portal vein, which carries blood from the small intestine. The structure and function of the liver remain normal.
Periportal (moderate) fibrosis.
This is an option with an increase in foci of necrosis, scarring and impaired liver function.
Bridging (severe) fibrosis.
At this stage, scarring has disrupted normal blood flow to the liver and function is further impaired.
Cirrhosis.
This is permanent scarring and irreversible loss of liver function.
Popular questions and answers
We asked gastroenterologist Valeria Lomova to answer popular questions about liver fibrosis.
Why is liver fibrosis dangerous?
The danger of fibrosis lies in the fact that it does not manifest itself in any way for a long time - the patient does not report complaints and does not seek help from a medical institution. In this case, fibrosis can progress, and all liver functions are disrupted, which leads to disaster throughout the body.
Who is most likely to have liver fibrosis?
At risk are:
- patients with viral hepatitis B and C;
- patients who have been drinking alcohol in hepatotoxic doses for more than 5 years;
- people suffering from obesity, autoimmune liver diseases, and storage diseases (hemochromatosis, Wilson's disease).
The development of liver fibrosis is also possible due to the toxic effects of certain groups of drugs.
Can fibrosis be cured completely?
Fibrosis regression is possible at all stages. But if it turns into cirrhosis, this is already the point of no return.
What complications can occur with liver fibrosis?
With long-term liver fibrosis, liver cirrhosis can develop, in which healthy connective tissue is completely replaced with disruption of all liver functions, which can lead to death.
Diagnosis and treatment
To diagnose pulmonary fibrosis, a pulmonologist performs the following tests and studies: general blood test; chest x-ray; computed tomography of the lungs, magnetic resonance imaging of the lungs; lung biopsy; breath tests. Treatment of pulmonary fibrosis is determined by a qualified specialist depending on the characteristics of the disease in a particular person. Glucocorticoids, cytostatics and immunosuppressants are used for severe forms of fibrosis. Lungs affected by fibrosis often become a favorable environment for the attachment of pathogenic microflora and the development of inflammation. To prevent this, antibacterial drugs are prescribed; oxygen inhalation and cardiac glycosides will be useful. For debilitating cough and shortness of breath, bronchodilators are prescribed. Drug treatment of pulmonary fibrosis should be supported by therapeutic breathing exercises, while large physical activities are contraindicated for the patient. It is also necessary to exclude exposure to fibrosis-provoking factors on the body.
Symptoms of pulmonary fibrosis
At the initial stage, the disease manifests itself as general weakness and increased fatigue. Patients experience pale skin with a bluish tint, especially in the nasolabial triangle, nose and limbs. Many patients report drowsiness during the day and insomnia at night, as well as unmotivated weight loss.
Then shortness of breath joins the above complaints. At the beginning, it bothers the patient only during physical activity, but as the pathology progresses, it begins to occur at rest.
Some patients have a dry or wet, unproductive cough. In the second case, a scant amount of viscous mucous sputum is detected. The appearance of purulent discharge indicates the addition of a secondary bacterial infection.
In patients suffering from pulmonary fibrosis for a long time, there is a change in the shape of the nails, which become like “watch glasses” and the terminal phalanges of the fingers like “drumsticks”.
At the peak of the disease, heart failure occurs, manifested by peripheral edema, palpitations, arrhythmia, pulsation of the neck veins, and severe shortness of breath at rest.
Causes
Pulmonary fibrosis can be caused by various reasons, including:
- chronic inflammatory processes in the lungs (for example, sarcoidosis or Wegener's granulomatosis);
- infections, the influence of environmental factors (asbestos, silicon, exposure to certain gases);
- exposure to ionizing gases (for example, radiation therapy used to treat breast tumors);
- chronic autoimmune diseases (lupus, rheumatoid arthritis);
- taking certain medications.
In allergic pneumonia, pulmonary fibrosis can develop as a consequence of an increased immune response to organic dust or chemicals that enter the lungs during inhalation. Some people may develop fibrosis without any specific cause. In this case, as a rule, they talk about idiopathic pulmonary fibrosis, which is not amenable to therapeutic treatment, while with other types of fibrosis (for example, interstitial pneumonia), the patient’s condition improves with properly selected treatment.
Publications in the media
Idiopathic fibrosing alveolitis is a pathological process in the lungs of unknown nature, characterized by inflammation and progressive fibrosis of the pulmonary interstitial tissue and air spaces, disorganization of the structural and functional units of the parenchyma, and the development of increasing respiratory failure.
Classifications. Previously, idiopathic fibrosing alveolitis was divided into mural, desquamative and mixed forms. Currently, several classifications are used, dividing idiopathic fibrosing alveolitis depending on the morphology, histological picture and clinical manifestations • Morphological classification of idiopathic interstitial pneumonia •• Usual interstitial pneumonia •• Desquamative interstitial pneumonia (respiratory bronchiolitis and interstitial lung disease are also distinguished) •• Obliterating bronchiolitis with organizing pneumonia •• Acute interstitial pneumonia •• Nonspecific interstitial pneumonia • Histological classification of idiopathic interstitial pneumonias (ATS/ERS, 2000) •• Usual interstitial pneumonia •• Alveolar macrophage pneumonia •• Respiratory bronchiolitis •• Organizing pneumonia •• Diffuse alveolar damage •• Nonspecific interstitial pneumonia •• Lymphocytic interstitial pneumonia • Clinical classification of idiopathic interstitial pneumonia (ATS/ERS, 2000) •• Idiopathic fibrosing alveolitis (idiopathic pulmonary fibrosis, cryptogenic fibrosing alveolitis) •• Desquamative interstitial pneumonia •• Respiratory bronchiolitis, interstitial lung disease •• Cryptogenic organizing pneumonia (idiopathic bronchiolitis obliterans with organizing pneumonia) •• Acute interstitial pneumonia •• Nonspecific interstitial pneumonia •• Lymphocytic interstitial pneumonia.
Incidence • The disease is more common in people aged 50 years and older • In the United States, the prevalence is 20 per 100,000 men and 13 per 100,000 women; incidence is 11 per 100,000 men and 7 per 100,000 women • In the UK, the prevalence is 6 cases per 100,000 population • In Russia there are no exact statistical data (due to underdiagnosis).
The etiology is not exactly known. Factors that can cause primary damage to lung tissue: tobacco smoke, metal, silicate and wood dust, asbestos, viruses (hepatitis C viruses, herpes viruses, including Epstein-Barr and cytomegalovirus [CMV]; adenoviruses). An association has been established between idiopathic fibrosing alveolitis and reflux esophagitis.
Genetic features. A genetic predisposition to excessive fibrosis formation in the lungs in response to nonspecific epithelial damage (presence of familial forms of the disease, frequent development of pulmonary fibrosis in some hereditary diseases) has been identified.
Pathogenesis • Acute stage (form) •• Damage to alveolar epithelial or endothelial cells by inhaled or circulating pathogenic factors with subsequent development of interstitial and intraalveolar edema (acute alveolitis) •• Release of chemotactic factors by activated inflammatory and immune cells •• Release of inflammatory mediators (oxidants , cytokines) and fibrogenic factors (eg, fibroblast growth factor, interleukin-1 [IL-1]) •• Possible either complete reversal or progression to acute interstitial pneumonia • Chronic stage (form) •• Process progresses to extensive damage lung and collagen deposition (widespread fibrosis) •• Characterized by hypertrophy of smooth muscles and an increase in alveolar spaces due to ruptures of the walls of the alveoli, lined with atypical (cuboidal) cells • Terminal stage •• Fibrous tissue completely replaces normal pulmonary structures with the formation of expanded air cavities •• Pulmonary the fabric takes on a characteristic “honeycomb” appearance.
Pathomorphology • Accumulation of inflammatory cells (mainly lymphocytes and plasma cells), fibroblasts and collagen fibers in the lumen of terminal and respiratory bronchioles and alveoli (pulmonary fibrosis) • Changes predominate in the subpleural region of the lung parenchyma and posterobasal segments • Characteristic is the development of dense fibrosis of the pulmonary parenchyma with an inhomogeneous type morphological changes.
Clinical picture • Clinical manifestations reflect increasing respiratory failure. According to the rate of increase in symptoms, acute, chronic and intermittent courses are distinguished • Complaints of inspiratory or mixed shortness of breath, dry cough. Chills and cough with sputum appear with bacterial superinfection (complication). Often fatigue, general malaise, aching chest pain, aggravated by deep inspiration, later - weight loss • Physical examination in the early stages may be uninformative •• In 40% of patients, body temperature rises to subfebrile and febrile, the peak increase occurs in the middle of the day •• With progression, tachypnea, tachycardia, cyanosis, deformation of the fingers in the form of “drumsticks” occur (with a long course of the disease) •• On inspiration, crepitus of the “cellophane cod” type is heard (usually in the basal parts of the lungs), in the later stages - sclerosiphonia (rough crepitus, reminiscent of the sound of a balsa wood plug rubbing) •• Signs of right ventricular failure appear.
Laboratory data • CBC data vary from normal to pronounced deviations: increased ESR, leukocytosis (more often with the addition of a bacterial infection); in the later stages, erythrocytosis and high Ht are characteristic • There may be an increase in the activity of lactate dehydrogenase (LDH) in the blood serum, the presence of circulating immune complexes (CIC), serum markers of idiopathic fibrosing alveolitis - surfactant proteins A and D, mucin Ag KL-6, alveolomucin 3EG5.
Instrumental data • X-ray of the chest organs •• With minimal changes against the background of severe clinical symptoms: small-focal infiltration, reticulation in the middle or lower lobes of the lungs (reticular changes) •• In late stages: picture of a “honeycomb lung” • High-resolution X-ray CT: picture “ground glass”, thickening and irregularity of the bronchial walls; changes in the pleura and lymphadenopathy are uncharacteristic • FVD: restrictive or mixed type of disorders (flow-volume curve, general body plethysmography), decreased diffusion capacity of the lungs; decreased compliance of the lungs • ECG: hypertrophy of the right heart (a consequence of the development of pulmonary hypertension), possible signs of myocardial hypoxia • Open or video thoracoscopic lung biopsy makes it possible to establish a diagnosis and determine the prognosis of the disease (morphological type of idiopathic fibrosing alveolitis) • Fiberoptic bronchoscopy allows for differential diagnosis with neoplastic processes in the lungs (may manifest as pulmonary dissemination) • Bronchoalveolar lavage is of auxiliary value; in the lavage fluid, a predominance of neutrophils and eosinophils is detected, less often - lymphocytosis.
Diagnostic tactics, diagnostic algorithms. To make a diagnosis, the presence of four major criteria and (at least) three minor criteria is necessary • Major criteria •• Exclusion of other interstitial lung diseases caused by known causes (drug intake, exposure to harmful environmental factors, systemic connective tissue diseases) •• Changes in pulmonary function, including restrictive changes and gas exchange disturbances •• Bilateral reticular changes in the basal lungs with minimal ground-glass changes on high-resolution CT •• Transbronchial biopsy or bronchoalveolar lavage does not suggest an alternative diagnosis • Minor criteria •• Age over 50 years •• Invisible, gradual onset of shortness of breath during exercise •• Duration of the disease for more than 3 months •• Inspiratory crepitus in the basal regions of the lungs.
Concomitant diseases • Pathology of the cardiovascular system due to the predominance of patients in older age groups • Iatrogenic conditions caused by the use of GCs and cytostatics (Itsenko-Cushing syndrome, secondary immunodeficiency).
Treatment • General tactics •• There is no specific treatment for idiopathic fibrosing alveolitis •• Anti-inflammatory, antifibrotic, antioxidant and symptomatic therapy • The regimen depends on the patient’s condition • Drug treatment. The basis of treatment is GCs and/or cytostatics for at least 6 months. Careful monitoring of the possible development of side effects of therapy is required •• In the early stages - acetylcysteine orally (600 mg 3 times a day for 3 months or more) •• GK (for example, prednisolone) ••• For underweight at a dose of 0.5 mg per 1 kg of body weight per day for 4 weeks ••• For normal body weight 0.25 mg per 1 kg of body weight per day for 8 weeks ••• Then the dose is reduced to 0.125 mg/kg/day or 0. 25 mg/kg every other day •• For underweight, GCs are combined with azathioprine at a dose of 2–3 mg per 1 kg of body weight per day or with cyclophosphamide at a dose of 2 mg per 1 kg of body weight per day. The maximum dose for both drugs is 150 mg/day, the initial dose is 25–50 mg/day. The dose is increased by 25 mg every 1–2 weeks until the maximum dose is reached •• Antifibrotic therapy (penicillamine) •• Bronchodilators (b2-adrenergic agonists, anticholinergic blockers or their combination in inhalations, intravenous aminophylline or prolonged forms of theophylline orally) are advisable only with instrumental proven bronchial obstruction (not considered a specific sign of idiopathic fibrosing alveolitis) • Oxygen therapy is indicated when paO2 is less than 50–55 mm Hg • Surgical treatment - lung transplantation.
Age characteristics • The main group of patients consists of elderly people, therefore it is necessary to take into account the high probability of concomitant pathology of the cardiovascular system • Pregnancy: the feasibility and risk of pregnancy depends on the degree of respiratory failure and the therapy performed.
Complications and their treatment • With the development of bronchiectasis and their superinfection, antibacterial therapy and transbronchial sanitation are necessary • With pneumosclerosis, “honeycomb lung”, severe respiratory failure, treatment of the underlying condition in combination with symptomatic therapy is necessary.
Dispensary observation, prevention • Observation by a pulmonologist at least once every 3 months, long-term • Monitoring of the respiratory function (flow-volume curve, diffusion capacity of the lungs), x-ray examination • There is no specific prevention.
Course and prognosis • The prognosis is favorable in the absence of progression or objective improvement after treatment, in other cases it is unfavorable • The prognosis depends on the course: •• acute course - death within 6 months to 2 years from the moment the first signs of the disease appear; •• chronic course - gradual progression with death on average after 6 years; •• relapsing course - average life expectancy 2–5 years • Favorable factors: young age (younger than 50 years), female gender, less than 1 year from the onset of signs of the disease, not very pronounced shortness of breath, preservation of respiratory function indicators, the presence of changes like “ ground glass" according to high-resolution CT, an increase in the proportion of lymphocytes (20–25%) in the bronchoalveolar lavage fluid, clinical improvement or a stable course of the disease after 3–6 months of GC therapy.
Synonyms. Hamman-Rich disease (acute form) • Hamman-Rich syndrome (chronic form) • Idiopathic pulmonary fibrosis • Cryptogenic fibrosing alveolitis • Skedding syndrome • Sclerosing alveolitis • Interstitial pneumonia • Interstitial pneumonitis • Diffuse interstitial lung disease • Fibrous dysplasia of the lungs.
ICD-10 • J84.1 Other interstitial pulmonary diseases with mention of fibrosis • J84.9 Interstitial pulmonary disease, unspecified