In May 2021, the US Food and Drug Administration (FDA) approved Aimovig (international nonproprietary name: erenumab), the first fully human antibody for the treatment of migraine. This medicine, developed jointly by the pharmaceutical companies Novartis and Amgen, has a fundamentally different mechanism of action than the drugs traditionally used to treat migraine. Will Aimovig be able to significantly reduce symptoms and improve the quality of life of migraine sufferers? Let's try to figure it out.
Modern medicines
A special project about modern medicines, the history of their creation, development methods and development trends.
The special project partner, Cytiva, was formed as a result of the sale of the GE Healthcare Biopharma division to Danaher Corporation. Cytiva is a global provider of technologies and services that advance and accelerate the development and manufacturing of therapeutics. The company has a rich heritage dating back hundreds of years. Cytiva's clients conduct life-saving activities ranging from basic biological research to the development of innovative vaccines, biologics and novel cell and gene therapies. The company's mission is to provide the tools and services they need to do things better, faster and safer, leading to better outcomes for patients.
The first two articles of our special project “Modern Medicines” were devoted to general issues of how the drug industry developed [1] and how scientists search for new drug targets [2]. This article opens a number of news materials about interesting modern medicines.
Side effects of drugs
Such drugs can be taken only 10 days a month. Otherwise some problems may arise. More frequent use of triptans may lead to the development of headaches that occur while taking the drug. In addition, drugs of this type have side effects, including:
- Feeling of warmth and stiffness in the limbs, drowsiness, asthenia, dizziness, sensory disturbance.
- Gastric or splenic infarction, ischemic colitis, hemorrhagic diarrhea, dry mouth, abdominal pain and nausea.
- Myalgia and muscle weakness.
- Spasm of coronary vessels, myocardial infarction, angina pectoris, tachycardia, rapid heartbeat.
- Polyuria and frequent urination.
- Anaphylactic shock, Quincke's edema, urticaria.
Despite all this, triptans for migraines are a quick-acting cure. If you take the medications strictly according to the instructions, then there will be no problems. The only noticeable drawback of such medications is the cost. Not everyone can afford to purchase such a drug.
How big is the problem?
Migraine, a neurological disease characterized primarily by severe attacks of headache, has been known for more than 3000 years [3]. However, despite the well-studied symptoms and manifestations, the causes of migraine have not yet been fully established. It was previously believed that migraine is caused by changes in cerebral circulation, but many researchers now suggest that this is not the main cause [4].
Current understanding of the pathogenesis of migraine involves the involvement of certain neural pathways and neuropeptides, particularly the trigeminal nerve and CGRP, a calcitonin gene-related peptide. Research has shown that excited nerve cells can activate the trigeminal nerve, leading to the release of CGRP and other neuropeptides. CGRP greatly dilates blood vessels, causing local swelling, and this attracts cells involved in the process of inflammation. With inflammation of the vessels of the skull and dura mater, proinflammatory molecules stimulate pain endings in the meninges, which leads to migraine (Fig. 1) [5–8].
This excitation of nerve cells, which triggers migraine, is associated with heredity and physiology, but today its causes are far from precisely determined [3]. It is only known that this process can be provoked by a variety of factors: from banal stress, fatigue and insufficient sleep to current hormonal levels, depressive states and medication use [9].
Figure 1. Pathogenesis of migraine
What happens during a migraine attack?
At the same time, migraine manifests itself not only as a headache: the symptoms of this serious illness are much more diverse, and often more painful. Debilitating migraine attacks can be painful and unbearable and sometimes last from several hours to several days, accompanied by nausea, vomiting and increased sensitivity to light, sound and smell [3], [10]. Such attacks deprive millions of people around the world of the ability to think, live and work normally. It is believed that every seventh inhabitant of the planet suffers from migraine today, and in the ranking of causes limiting the ability to work, this disease took second place in the world (according to 2021 data) [11], [12].
It is not surprising that migraine was included by the World Health Organization in the list of diseases that most disrupt the social adaptation of patients [3].
Mode of application
The tablets should be taken orally. The triptan dosage is 2.5 mg. If the pain returns, you can repeat taking the drug, but not earlier than 2 hours after taking the previous tablet. The spray is sprayed into the nasal cavity, which ensures better absorption.
The use of triptans is completely contraindicated in the presence of the following diseases:
- Hypertension;
- Arrhythmia;
- Ischemic disease;
- Angiospastic angina;
- Cerebrovascular accident;
- High sensitivity to the components included in triptans;
- Adolescence.
The drug should be used with extreme caution during lactation, pregnancy, as well as severe liver or kidney failure.
Migraine treatment today
Unfortunately, today there is no medicine that can get rid of migraines once and for all. The drugs used can mainly reduce the intensity and number of attacks or reduce symptoms and relieve pain. In this regard, therapy with such drugs is divided into two groups:
- Abortive (acute) therapy - to relieve or reduce symptoms of migraine that has already appeared.
- Preventative treatment – to reduce the intensity, duration or frequency of attacks.
In this article we talk about drug treatment and prevention, but leave behind the scenes a variety of non-pharmacological treatments for migraine: from relaxation techniques to cognitive behavioral psychotherapy and transcranial electrical stimulation. Meanwhile, these methods in some cases can be an effective alternative to medications in case of resistance or contraindications to drug therapy, and sometimes effectively complement it in the combined treatment of migraines [13].
Abortion therapy
In the treatment of mild to moderate migraines, various analgesics and NSAIDs (non-steroidal anti-inflammatory drugs) are prescribed, including the well-known paracetamol, acetylsalicylic acid and ibuprofen, sometimes in combination with caffeine, codeine or psychotropic substances in combination medications [14], [15]. ]. A significant drawback is the possible reverse effect of uncontrolled use of analgesics: worsening headaches, which in such conditions can become daily [8], [15].
When it comes to dealing with more severe and prolonged attacks of migraine pain, the “heavy artillery” comes into play, namely ergot alkaloids and triptans. Triptans were the first drugs created specifically for the treatment of migraine; They began to be developed back in 1972. Even then it was known that the ergot alkaloid ergotamine can reduce migraine attacks, which was associated with its vasoconstrictor effect [16]. This drug remained the only specific treatment for migraine until, in 1991, rational research finally led to the emergence of sumatriptan, the first drug of a new class that acts in a similar way to ergotamine, but is more effective and safe (Fig. 2) [16].
Unlike its famous derivative, LSD, ergotamine itself does not have hallucinogenic properties.
Figure 2. Triptans, medications used to relieve migraines, are selective serotonin receptor agonists. They bind to and activate specific subtypes of these receptors (5HT1B, 5HT1D and 5HT1F). This leads to inhibition of the release of neurotransmitters from the presynaptic membrane of the trigeminal nerve endings (shown in yellow), located in the vessels of the head. At the same time, the release of the already mentioned CGRP, a key neurotransmitter that causes migraines, is also inhibited. This “neural” mechanism of action is believed to block the main pathological link in the development of migraine. It is also known that taking triptans selectively constricts the vessels of the dura mater, reduces the permeability of the vascular wall and reduces edema. Either way, these medications are effective—they reduce inflammation and pain, as well as the intensity of accompanying migraine symptoms [17]. The ergot alkaloids ergotamine and dihydroergotamine act in a similar way, although they are less selective - they can bind to dopamine and adrenergic receptors, which is why their effectiveness and safety are lower.
[18]
However, despite their good efficacy and safety profile, triptans may theoretically be dangerous for patients with coronary artery disease due to their vasoconstrictor effects, which limits their widespread use as therapy for migraine [16].
Preventive therapy
Drug prevention is indicated when migraines are regular (more than 2-3 times a month), and it must be said that today such therapy is not entirely safe and effective: it is associated with significant side effects and the development of rapid tolerance to treatment (tachyphylaxis) [14]. In this case, several classes of drugs are used, originally developed for other indications, and so far with a largely unclear mechanism of action for migraine. These medications include: tricyclic antidepressants, antiepileptic drugs, beta blockers, calcium channel blockers, ACE inhibitors and some others [14], [19].
By the way, you can read about many of the listed drugs, their direct indications, history of appearance and mechanism of action in the first article of our series “Three generations of drugs” [1].
Material and methods
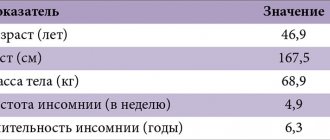
An open, randomized, prospective, comparative study was conducted in 60 patients with episodic migraine with and without aura aged 18 to 65 years. The study included patients with migraine, the diagnosis of which was established in accordance with the ICHD-3 beta diagnostic criteria (2013). The frequency of headache attacks was no less than 2 and no more than 15 days in 1 month, which excluded the participation of patients with chronic migraine. The study did not include patients under 18 years of age or over 65 years of age, patients with drug-induced headache, taking migraine prophylaxis or other specific anti-migraine drugs. Patients with other neurological or psychiatric pathologies, as well as with a history of coronary heart disease or cerebrovascular disease were also not included.
Two groups were formed using simple randomization. Group 1 included 30 patients, whose average age was 31.0±6.7 years ( p
<0.01), predominantly women - 90% (
n
= 27).
6 (20%) patients had migraine with aura and 24 (80%) without aura, with a frequency of 2.2±1.0 attacks per month ( p
<0.01). Patients of group 1 took L.P. Migrepam in accordance with the instructions for medical use of the drug in a therapeutic dose of 2.5 mg.
Group 2 also included 30 patients, of which 24 (80%) were predominantly women. The mean age in the group was 31.5±7.4 years ( p
<0.01).
9 (30%) patients had episodic migraine with aura and 21 (70%) without aura with an average frequency of 2.2±1.3 attacks per month ( p
<0.01). In group 2, patients were prescribed L.P. as a drug to relieve headache attacks. Sumatriptan at a dose of 50 mg.
A comparison of the baseline characteristics of the study groups is presented in Table. 2.
Table 2. Comparative analysis of clinical and demographic indicators of the study groups Note. Data are presented in number (%) or mean (SD) format. VAS - visual analogue scale. * - p-value - statistical significance of differences compared to the average value in the study groups (p <0.05). Note. Data are presented in number (%) or mean (SD) format. VAS - visual analogue scale. * — p-value — statistical significance of differences in comparison with the average value in the study groups (p<0.05)
When examined in the study groups, the average age was comparable and fell in the third decade of life; in terms of gender distribution, females predominated in both groups. According to diagnostic criteria, migraine without aura predominated in both groups, with comparable frequency and intensity of headaches.
Participation in the study included three follow-up visits.
During the first (baseline) visit, inclusion criteria were determined, a clinical neurological examination was performed, vital signs (blood pressure, heart rate) were recorded, and concomitant medications or other therapy were assessed. The intensity of headache, photo- and phonophobia was determined using a 10-point VAS scale. The criteria for assessing headache included the following characteristics: frequency, severity of associated symptoms, number of attacks relieved by triptans. In addition, we studied indicators of the degree of influence of headache on the general condition and quality of life (HIT-6 index - Headache Impact Test), time of disability associated with headache (HALT index - The Headache-Attributed Lost Time), and the degree of maladaptation caused by migraine (MIDAS). Patient satisfaction with the therapy used for migraine attacks was assessed (MIGRAINE-ACT - The Migraine Assessment of Current Therapy). On the 2nd visit after 30 days, while taking L.P. Migrepam and L.P. Sumatriptan was subjected to a clinical neurological examination and assessment of headache characteristics (frequency, severity of attack and associated symptoms when relieved with the appropriate triptan). During the visit, questionnaires HIT-6, HALT, MIDAS, MIGRAINE-ACT were filled out. At the 3rd visit, after 60 days, the patients were finally examined and all the above-mentioned questionnaires were filled out. The effectiveness of therapy for L.P. Migrepam and L.P. Sumatriptan was assessed using specially designed symptom diaries completed by patients during three consecutive attacks.
Clinical characteristics of the impact of headache on patients in the study groups during the baseline visit are presented in Table. 2. The average value of the degree of influence of headache on the general condition and quality of life (HIT-6 index) was 59.9±5.9 points in group 1, 55.9±8.9 points in group 2, ( R
<0.05), which corresponds to a significant impact of migraine on daily activities.
The severity of pain and the degree of maladjustment on the MIDAS scale in group 1 exceeded the value in group 2 ( p
<0.01), however, both indicators indicated the presence of a pronounced limitation of daily activity in patients of both groups (≥21 points corresponds to grade IV severity ) [8].
The HALT index over the last 3 months before the start of treatment in the 1st group was 27.5±4.7 days, and in the 2nd group - 22.4±7.4 days ( p
<0.01), which indicates on the strong influence of headache on the functional state in the study groups and the need for drug correction of headaches. During the examination, satisfaction with the previously used therapy for migraine attacks according to the MIGRAINE-ACT questionnaire in group 1 was noted by 9 (30%) patients, which was comparable to the value in group 2 - 11 (38%).
Statistical analysis was carried out depending on the distribution of the sample population using parametric tests of Student, Pearson and Fisher's exact test using Excel 2021 and the statistical software package Statistica 12. To present the obtained data, methods of descriptive statistics were used (with the calculation of average values, standard deviation, standard errors of the mean). The results were regarded as significant at p
-value <0.05.
Targeted therapy for migraine: a solution to the problem?
Since migraine is a chronic disease and the effectiveness and safety of the drugs used for prevention is poor, there is clearly an unmet need in this area; however, there are few new drugs specifically developed for this indication [14].
Amgen and Novartis can boast of a breakthrough today, having received approval in May 2021 for the use of the targeted drug Aimovig erenumab antibodies ) for the prevention of migraine in adult patients [20]. This is the first fully human antibody to be commercialized whose preventive effect is due to binding and blocking the CGRP receptor, which is considered critically important in the development of migraine (Fig. 3).
Figure 3. Aimovig specifically binds to the CGRP receptor, preventing CGRP from binding to it. The binding of CGRP to its receptor in a molecular complex (shown on the left) results in the transmission of pain signals associated with migraine. In people with migraine, CGRP levels are elevated during a painful attack and return to normal levels when the migraine pain subsides.
About Aimovig® (erenumab) in migraine prevention
Aimovig was approved after three series of clinical trials, the results of which, although slightly different, were similar in one thing: the drug showed a significant reduction in the number of days with attacks and the total duration of migraine pain. Moreover, in phase III trials, in 50% of patients taking 140 mg of Aimovig, the number of painful days decreased by half compared to placebo, and the safety and tolerability of the drug turned out to be quite similar to placebo [21], [22]. . These results are very encouraging, and it is clear that although Aimovig is not a panacea, its use will definitely change the lives of patients suffering from frequent and severe migraines for the better.
Antibody purification using continuous countercurrent chromatography
Biotechnologically derived antibodies can be purified using the chromatography equipment of this material's partner, Cytiva. This is done in continuous counter-current chromatography (PCC) mode on an ÄKTA pcc . In combination with the minimal dimensions of the system, continuous chromatography technology ensures the most efficient use of the chromatographic sorbent (resin). This method is particularly suitable for the purification of unstable molecules, as the rapid process ensures the stability of the target product. The ÄKTA pcc system is based on the well-established and widely used ÄKTA chromatography system platform by scientists around the world. Key features of the ÄKTA pcc system:
- Flow rate: 0.5–75 ml/min.
- Maximum operating pressure: 20 bar.
- Supports three and four column PCC configuration (3C and 4C PCC).
- Integrated UV detectors: one tunable wavelength (three values) and three fixed wavelength (280 nm).
- Monitors for tracking pH and conductivity readings.
- Interactive visualization that continuously shows column status and process progress.
- Trend lines that allow you to immediately begin analyzing the information received about the process.
ÄKTA chromatography systems can be used in conjunction with AxiChrom columns, although they are also suitable for larger scale protein purifications. A wide range of column sizes of the same type (Figure 4) allows protein purification to be scaled up with minimal parameter changes.
Figure 4. AxiChrom is a family of pilot-scale to industrial-scale protein purification columns with i.d. diameters of 50–1600 mm. AxiChrom columns successfully combine standardization and customization and are compatible with a variety of advanced media, such as MabSelect SuRe™ antibody purification resin.
Cytiva's research has confirmed the similarity between the protein purified in the laboratory and in production. In this case, the volume of the drug was scaled by 294 times (Fig. 5).
Figure 5. Comparison of chromatograms obtained using ÄKTA pcc on HiTrap columns (a) and AxiChrom 50 columns (b)
Material provided by our partner - Cytiva
"Aimovig" and competitors
It must be said that Novartis and Amgen already have serious competitors in the field of targeted anti-migraine therapy: Eli Lilly released Emgality, and Teva Pharmaceutical released Ajovy. These drugs are humanized monoclonal antibodies that target the ligand rather than the CGRP receptor, and in this way they differ from Aimovig, being inferior to the latter at least in tolerability. When using Ajovy, 43–45% of patients experienced pain, redness and itching at the injection site, when using Emgality, 18% of patients experienced such symptoms, and Aimovig caused such reactions only in 5–6% of cases. At the same time, Aimovig is also more convenient to use, since of the three listed drugs, only it comes in the form of an auto-injector - a device that resembles an insulin syringe pen - which needs to be used only once a month. The listed advantages, coupled with the fact that Aimovig became the first targeted drug for the treatment of migraine and immediately filled an empty niche in the market, will most likely provide it with a bright financial future: according to experts, its market share in 2024 will be $2 billion, while the predicted shares of competitors are approximately half as much [20].
The success of Aimovig, apparently, cannot be hampered even by the extremely high price ($575 per month according to the Amgen price list - however, in the United States, the drug is covered by insurance for many patients), which, by the way, some experts consider unreasonable [11]. The company is conducting research on Aimovig in Russia, but when the drug will appear on the market, how much it will cost and who will pay for it is still unknown.
How to quickly and effectively stop a migraine attack?
In order to get rid of a migraine attack, there is an effective and proven scheme:
- first of all, you should take 1000 mg of aspirin, 10-20 mg of Motilium and drink a cup of drink with caffeine and sugar;
Motilium - if after 45 minutes there is no visible relief, you need to take one of the triptans;
- if the use of analgesics does not bring the desired result for three attacks in a row, you should immediately take triptans;
- in cases where migraine is accompanied by an aura, acetylsalicylic acid should be taken immediately after the onset of unpleasant symptoms, and after the onset of headaches, a triptan should be taken immediately.
In addition, you can alleviate the condition of a migraine if you lie down in a dimly lit room, periodically take a cool shower, and drink soothing decoctions of medicinal herbs.
You can rub ointments containing menthol or regular “Star” into your temples, and also massage the points that are responsible for brain activity.
Migraine is a disease that can affect anyone. There are medications to relieve attacks, they are called triptans. This group has a large list of medications. Thanks to its use, you can eliminate the unpleasant symptoms of migraine. The most important thing is to consult a doctor to select a medication and adhere to the information specified in the instructions for use.
Literature
- Three generations of drugs;
- Search for drug targets;
- Sanoeva M.Zh. and Saidvaliev F.S. (2016). Migraine - yesterday, today, tomorrow. A modern view of the problem. "International Neurological Journal". 8, 72–78;
- How a migraine happens. Johns Hopkins Medicine;
- Migraine headaches. (2018). WebMD;
- Paul L. Durham. (2006). Calcitonin Gene-Related Peptide (CGRP) and Migraine. Headache
.
46 , S3-S8; - What to know about the new anti CGRP migraine treatment options. (2018). American Migraine Foundation;
- Silberstein S. D. (2016). Migraine. MSD Directory;
- Migraine triggers: your personal checklist. (2019). WebMD;
- Rusakova E. (2018). The FDA has approved the drug to prevent migraines. N+1;
- Kolata G. (2018). The FDA approves the first drug designed to prevent migraines. The New York Times;
- Theo Vos, Amanuel Alemu Abajobir, Kalkidan Hassen Abate, Cristiana Abbafati, Kaja M Abbas, et. al.. (2017). Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet
.
390 , 1211-1259; - Francesca Puledda, Kevin Shields. (2018). Non-Pharmacological Approaches for Migraine. Neurotherapeutics
.
15 , 336-345; - Doodipala Samba Reddy. (2013). The pathophysiological and pharmacological basis of current drug treatment of migraine headache. Expert Review of Clinical Pharmacology
.
6 , 271-288; - Ogbru A. and Ogbru O. Prescription migraine medications. RxList;
- Boyce S., Ali Z., Hill R. G. (2001). New developments in analgesia. Drug Discovery World;
- Azimova Yu.E. (2017). Triptans: an era of specific treatment for migraine. "Nervous diseases". 1, 10–14;
- Ameri M. and Lewis H. (2018). The evolution of transdermal drug delivery and treating migraine. Drug Discovery World;
- Migraine medications. (2013). TMedWeb;
- Dmitriev R. (2019). "Aimovig" will turn chronic migraine into episodic. "Mosmedpreparaty";
- Aimovig (erenumab) for the treatment of episodic migraine. Clinical Trials Arena;
- Khoruzhaya A. (2018). A new anti-migraine drug goes on sale. "Neuronews";
- Targeted therapy is a targeted strike against the disease.