Mucous swelling of the skin, brittle hair and nails, a rough hoarse voice, freezing caused by circulatory failure, heart pain, fatigue, drowsiness, decreased overall tone, general lethargy and impaired ability to concentrate, decreased appetite, constipation - all these are symptoms of myxedema.
Below in the article you will find the causes of the disease; the doctors who treat him; necessary medical procedures for treatment; as well as general information about the disease, its localization, features of diagnosis of diseases and their treatment. However, we advise you to consult a doctor, because self-medication is 90% fraught with complications. Make an appointment and consultation
Myxedema. general information
Myxedema is an endocrine disease characterized by decreased thyroid function and is a severe form of hypothyroidism. The disease most often occurs in adolescents and adults. The primary and secondary nature of the onset of the disease are distinguished. Myxedema can also be congenital or acquired.
When treating Myxedema, doctors at the BIOSS clinic use both time-tested and the latest developments and proprietary techniques.
Our clinic employs the best doctors in Moscow who have extensive experience in the treatment of Myxedema
Complications
The main danger of a long-term course of severe myxedema in the absence of treatment is the onset of myxedema coma. At risk are elderly patients and people with a weakened immune system due to acute infections, hypothermia, long-term hypothyroidism and chronic diseases. The list of symptoms of coma includes a drop in body temperature, intestinal obstruction, slowing of the pulse and breathing, heart failure, confusion. The probability of death for patients in this condition reaches 80%.
Symptoms of myxedema
Thyroid hormones affect the functioning of the body as a whole, so myxedema is a disease characterized by a multiplicity of symptoms that are present in all body systems. However, there are characteristic symptoms of myxedema, the combination of which is a diagnostic sign of this disease.
These signs include:
- Mucous swelling of the skin and subcutaneous tissue. Mucosal edema differs from other types of edema in that when pressed with a finger, there is no depression left on the skin, as happens with other types of edema. As a result of edema, the face becomes puffy and mask-like, facial features are rough, bags appear under the eyes;
- Hair is brittle, thin, falls out easily, nails are brittle and peeling. This symptom of myxedema is caused by dystrophic changes in the skin and subcutaneous tissue that occur due to mucous edema;
- A rough, hoarse voice, which occurs due to swelling of the vocal cords; due to swelling of the tongue, speech may become slurred and blurred;
As follows from the above, the leading symptoms of myxedema are a consequence of the same mucous edema.
The remaining symptoms of myxedema are characteristic of all types of hypothyroidism: freezing caused by circulatory failure, heart pain, fatigue, drowsiness, decreased general tone, general lethargy and impaired ability to concentrate, decreased appetite, constipation. The musculoskeletal system suffers, myalgia (muscle pain), muscle weakness, arthralgia (joint pain), and arthrosis appear. Polyserositis occurs - combined inflammation of the internal membranes (peritoneum, pericardium, pleura).
Myxedema in childhood is manifested by a delay in physical, mental and sexual development. Myxedema in children can be congenital or early. The earlier the thyroid function is disrupted, the more serious the consequences are for the child’s health. Congenital myxedema is manifested by cretinism - a severe disorder of all body systems, the most pronounced of which is growth retardation, deformity due to improper development of the musculoskeletal system, and a significant decrease in intelligence. With early myxedema, the child’s development is suspended from the moment the disease occurs.
Ascites with myxedema: a clinical case of regression of ascites during thyroid therapy
A clinical case was considered regarding a patient with ascites, the cause of which was primary hypothyroidism. For ten years the patient was treated unsuccessfully for liver cirrhosis. Therapy with thyroid hormones led to complete regression of ascites. In addition, the causes, pathogenesis and other cases of the development of ascites with myxedema described in the literature are given.
Indicators of protein in ascitic fluid and serum-ascitic albumin gradient in patients with myxedematous ascites, g/dL
Introduction
Hypothyroidism (myxedema) is an endocrine disease that develops as a result of a deficiency of thyroid hormones. Severe hypothyroidism is characterized by a mask-like puffy face, periorbital edema, dry skin, hair loss, decreased hearing, decreased body temperature, slowed speech, hoarseness, constipation, hypotension, bradycardia, impaired memory and intelligence, amenorrhea and infertility in women [1]. Symptoms of hypothyroidism are nonspecific and can occur with other chronic somatic and mental diseases. The diagnosis is confirmed by determining the level of thyroid hormones. However, a direct relationship between the level of thyroid hormones and the severity of clinical manifestations of the pathology has not been noted [2]. A feature of hypothyroidism is the presence of numerous masks that imitate other diseases, which greatly complicates its recognition. Currently, the following hypothyroidism masks are described: dermatological (alopecia, hyperkeratosis, onycholysis), cardiological (arterial hypertension, dyslipidemia, hydropericardium), gynecological (uterine bleeding, oligo-/amenorrhea, infertility), rheumatological (polyarthritis, polysynovitis, osteoarthritis), gastroenterological (constipation, biliary dyskinesia, cholelithiasis, chronic hepatitis, jaundice with increased transaminase levels) [3, 4]. In elderly people, hypothyroidism can occur in the form of monosymptomatic forms: hydropericardium, pleurohydropericardium, ascites, depression, paranoid psychosis, seizures, paresthesia, muscle weakness. Such patients are observed for a long time by various specialists: general practitioner, cardiologist, neurologist, gastroenterologist. There are cases when the only symptom of hypothyroidism is hydropericardium [5]. Quite rarely (in 4% of patients) it can occur with ascites [6].
Below we consider a clinical case of hypothyroidism, the most pronounced manifestation of which was long-term ascites, tolerant to conventional therapy. Complete regression of ascites was facilitated by treatment with thyroid hormones.
Clinical case
Description
Patient T. born in 1965. She was treated in the gastroenterological and endocrinological departments of the Novosibirsk Regional Clinical Hospital from March 20 to April 19 and from November 23 to December 6, 2021, respectively. Upon admission, the patient complained of pain in the epigastric region after eating and overeating, in the right hypochondrium, worsening after eating, severe weakness, fatigue, decreased appetite, swelling of the face and legs, drowsiness, chilliness, constipation, increased abdominal volume, decreased hearing , sometimes interruptions in the functioning of the heart.
For ten years, the patient was observed by a physician at her place of residence for cryptogenic cirrhosis of the liver (toxic etiology of cirrhosis was also not excluded) of moderate activity, progressive course, decompensated portal hypertension, chronic hepatocellular failure class B according to the Child-Pugh classification, splenomegaly, ascites. The diagnosis was confirmed by laparocentesis; the amount of ascitic fluid reached 20 liters. Laparocentesis was performed every six months, the last time in May 2021. She was treated at the place of residence. She took courses of hepatoprotectors and diuretics. Since November 2021, the condition has worsened: the volume of the abdomen has increased significantly, swelling of the face and legs, drowsiness, chilliness, constipation, and hearing loss have appeared. She was hospitalized on March 20, 2021 in the gastroenterology department for examination and treatment.
When collecting anamnesis, it was also established that in 2002 the patient was diagnosed with pulmonary tuberculosis, and in 2008 she was removed from the register. An examination by a phthisiatrician conducted on March 12, 2021 (on an outpatient basis) confirmed residual changes in the lungs resulting in dense foci. The patient has not worked for the last 15 years and is a disabled person of the second group. His mother died from laryngeal cancer, his father from stomach cancer. She previously smoked and abused alcohol; for the last ten years she has not taken or smoked alcohol. Married. Five pregnancies, three births. Menopause occurred at 38 years old.
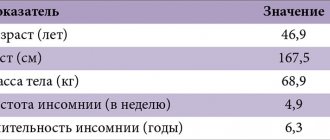
Objectively: the condition is serious, body temperature is 36.6 ºС. Weight – 64 kg, height – 162 cm, body mass index – 24.6 kg/m². The skin is pale, dry skin, swelling of the face, legs, feet. Visible mucous membranes are pale, hair is sparse. The face is amicable, mask-like. The voice is quiet. Lymph nodes are not enlarged. The thyroid gland is not enlarged, dense, painless, mobile, the structure is heterogeneous. The respiratory rate is 16 per minute. The lung boundaries are within normal limits. Vesicular breathing. Heart rate – 64 per minute, pulse of good tension and filling. Blood pressure – 100/80 mm Hg. Art. The boundaries of the heart are within normal limits. Heart sounds are clear and rhythmic. No pathological noises were detected. The tongue is moist, covered with a white coating with teeth marks. The abdomen is enlarged in size due to ascites, participates in the act of breathing, and is painful on palpation in the right hypochondrium. The liver is along the edge of the costal arch, dimensions according to Kurlov are 10 × 9 × 8 cm. He suffers from constipation. Breast glands without visible pathology. On the second day of hospitalization, a paroxysm of atrial fibrillation was registered. The electrocardiogram recorded during the paroxysm showed atrial fibrillation (normosystolic variant) and diffuse changes in the myocardium. Sinus rhythm restored independently, without treatment. Holter monitoring was performed. Within 21 hours 20 minutes, sinus rhythm was recorded, the average frequency of ventricular contractions was 64 per minute, the minimum was 49, the maximum was 117 per minute, and an episode of pacemaker migration through the atria. No ST segment shift was noted during the day. Circadian index – 1.07.
Upon admission, a general blood test was performed: level of red blood cells – 2.75 × 1012/l (normal 3.5–5.1 × 10/12 l), hemoglobin – 87 g/l (normal 120–150 g/l), leukocytes – 5.35 × 109/l (normal 4.0–9.0 × 109/l), lymphocytes – 30.0% (normal 19.0–38.0%), neutrophils – 63.0% (normal 40 ,0–72.0%), monocytes – 4.0% (normal 3.0–11.0%), eosinophils – 3.0% (normal 0.0–5.0%), erythrocyte sedimentation rate (ESR ) – 44.0 mm/h (normal 2.0–20.0 mm/h).
Biochemical blood test: increase in total protein to 109.3 g/l (over time to 102.91 g/l) (normal 66.0–83.0 g/l). Changes in protein fractions: albumin – 42.99% (normal 55.0–67.0%), α1-globulin – 3.36% (normal 1.8–5.2%), α2-globulin – 11.24% (normal 5.0–13.1%), β-globulin – 16.38% (normal 7.9–13.6%), γ-globulin – 28.95% (normal 10.0–19.0% ). Increased tumor marker CA-125 - more than 500.0 IU/l (normal range 0.0–21.0 IU/l), aspartate aminotransferase (AST) up to 85.5 U/l (normal range 0.0–35.0 U/l ), cholesterol up to 7.4 mmol/l (normal 2.9–5.2 mmol/l), β2-microglobulin up to 5660.0 µmol/l (normal 0.0–2400.0 µmol/l), creatinine up to 140.9 µmol/l (normal 58.0–97.0 µmol/l), urea up to 8.7 mmol/l (normal 2.8–7.2 mmol/l). Decrease in glomerular filtration rate (GFR) to 37.01 ml/min/1.73m2 (normal range 80.0–145.0 ml/min/1.73m2). The rest of the indicators were within normal limits: total bilirubin – 8.4 µmol/l (normal range 5.0–21.0 µmol/l), direct bilirubin – 2.4 µmol/l (normal range 0.0–7.9 µmol/l) l), alanine aminotransferase (ALT) – 22.9 U/l (normal 0.0–35.0 U/l), alkaline phosphatase – 50.8 U/l (normal 30.0–120.0 U/l) , blood amylase – 97.1 U/l (normal 28.0–100.0 U/l), glucose – 4.0 mmol/l (normal 3.3–6.0 mmol/l), potassium – 5, 16 mmol/l (normal 3.5–5.5 mmol/l), sodium – 135.3 mmol/l (normal 130.0–150.0 mmol/l), chlorides – 100.7 mmol/l (normal 98.0–107.0 mmol/l), iron – 13.1 µmol/l (normal 9.0–30.0 µmol/l), ferritin – 71.8 µg/l (normal 13.0–150, 0 µg/l), α-fetoprotein – 13.2 IU/ml (normal range 0.0–14.4 IU/ml). A slight decrease in cortisol in daily urine – 38.75 mg/day (normal 48.0–403.0 mg/day). Examination of urine sediment according to Nechiporenko: leukocytes - 110 × 103, erythrocytes - 15 × 103, hyaline casts - 7. Ascites was confirmed by the results of an ultrasound examination of the pelvic organs: there is a large amount of free fluid in the abdominal cavity, the fluid level in the retrouterine space is 56.0 mm. In addition, diffuse changes in the liver, pancreas, and kidneys were detected. Echo signs of the uterus and ovaries were consistent with menopause. The results of magnetic resonance imaging (MRI) of the abdomen and pelvis also confirmed the presence of ascites. In addition, MRI of the abdominal cavity revealed a formation of parietal peritoneum.
Thus, when assessing the objective status and routine tests, peripheral edema and ascites, dry skin, hypotension, paroxysmal rhythm disturbance (atrial fibrillation), anemia, increased ESR, hyperproteinemia, renal failure, cytolysis, hypercholesterolemia, leukocyturia, β2-microglobulinemia were previously identified , formation of the parietal peritoneum.
Differential diagnosis was carried out between liver cirrhosis, cardiac fibrosis, tuberculous process in the abdominal cavity and kidneys, paraproteinemic hemoblastosis, peritoneal carcinomatosis, toxic (alcoholic) or medicinal (tuberculostatics, loop diuretics, non-steroidal anti-inflammatory drugs) kidney damage, amyloidosis, chronic pyelonephritis.
During fibrogastroduodenoscopy (FGDS), no signs of portal hypertension or varicose veins of the esophagus were detected. According to the results of irrigography, there were no organic changes in the colon. When performing multislice computed tomography (MSCT) of the abdominal cavity and retroperitoneal space, in addition to ascites, compaction of the fiber of the mesentery of the small intestine and greater omentum (of inflammatory or tumor origin), as well as diffuse changes in the parenchyma of the left kidney were detected.
Laparoscopy was performed with a biopsy of the liver and the area of compaction of the tissue of the mesentery of the small intestine and the greater omentum. Histological examination revealed a picture characteristic of liver fibrosis of the first or second degree. There were no signs of tuberculosis or carcinomatosis. Laparoscopy revealed an uneven surface of the liver. Cytological examination of ascitic fluid reveals single lymphocytes, neutrophilic leukocytes, groups of mesothelial cells with proliferative-degenerative changes. There were no elements of malignant growth. Based on the results of laparoscopy with visual examination of the liver, liver biopsy, and cytological examination of ascitic fluid, liver cirrhosis was excluded. A tumor and metastatic process of any localization is rejected taking into account the data of MSCT, X-ray contrast and endoscopic studies (irrigography, FGDS), laparoscopy, histological report, and analysis of ascitic fluid.
Considering the presence of anemia and hyperproteinemia, the patient underwent sternal puncture and trephine biopsy. Myelogram: the total number of myelocytes in the bone marrow punctate is moderate, the punctate is cellular, there is no blastosis, the ratio of leukocytes to erythrocytes is 15.9:1.0. The ratio is increased due to a decrease in erythroid cells, erythropoiesis of the normoblastic type. Trepanobioptate: all hematopoietic germs are sharply narrowed, erythrocyte and granulocytic germs are represented by discretely located mature and intermediate forms, megakaryocytes are single in all fields of view. Bone marrow hypoplasia/aplasia occurs. Myelogram and trephine biopsy data allowed us to exclude paraproteinemic hemoblastosis.
The patient had a tuberculous etiology of ascites excluded. MSCT of the chest organs was performed with reconstruction of the magnetic resonance imaging image. Signs of emphysematous changes in the lungs, single bullae in S1 of the right lung, multiple calcifications of different sizes in the lungs, and areas of pneumofibrosis in the upper lobes of both lungs were found. An ultrasound examination of the abdominal aorta and renal vessels revealed no changes, there is sufficient blood flow in the kidneys, and the parameters are within normal limits. Bacteriological culture of urine was performed - no population growth was recorded. Polymerase chain reaction of urine did not detect Mycobacterium tuberculosis. Bacteriological culture of ascitic fluid - no growth of Mycobacterium tuberculosis was recorded. A microscopic examination of a fragment of the duodenal mucosa revealed signs of moderate chronic inflammation without atrophy of the intestinal villi. In small areas of the submucosal layer there are several arterioles and venules, their walls are not thickened, the staining for amyloid is questionable, and when examined in polarized light, there was no greenish glow in the walls of the vessels. Based on data from laparoscopy and biopsy of formations of the parietal peritoneum, polymerase chain reaction for the presence of Mycobacterium tuberculosis and examination of ascitic fluid, microscopic examination of a fragment of the duodenal mucosa, the diagnoses of “tuberculous mesadenitis” and “amyloidosis” were rejected. Echocardiography was performed to exclude cardiac fibrosis of the liver. Normal heart sizes, sclerosis of the aortic root and aortic valve leaflets, focal sclerosis of the left ventricular myocardium, and normal left ventricular systolic function (ejection fraction 63%) were determined. Type 1 left ventricular diastolic dysfunction. The cavities of the heart are not enlarged.
Despite numerous studies, the diagnosis remained unclear. To exclude endocrine pathology, an endocrinologist was invited to a consultation, who, based on the medical history and clinical signs (dry skin, slow speech, hearing loss, severe peripheral edema, constipation, hypotension, anemia), diagnosed hypothyroidism. In addition, for the first time, the presence of ascites was explained as a consequence of endocrine pathology. Primary manifest hypothyroidism is confirmed by hormonal studies: the level of thyroid-stimulating hormone (TSH) is more than 100.0 µIU/ml (normal range is 0.35–4.94 µIU/ml), free thyroxine (free T4) is less than 3.86 pmol/ l (normal 11.5–22.7 pmol/l). Antibodies to thyroid peroxidase (AT-TPO) – 140.0 U/ml (normal range 0.0–30.0 U/ml).
Ultrasound examination of the thyroid gland: total volume – 9.1 ml. Echo signs of diffuse changes in the thyroid gland. Consequently, symptoms such as ascites, impaired renal function, anemia, hyperproteinemia were manifestations of hypothyroidism against the background of autoimmune thyroiditis.
The patient was prescribed hormone replacement therapy with levothyroxine with a gradual increase in dose from 50 to 125 mcg/day (taking into account the presence of heart rhythm disturbances) for two months under the control of TSH levels, st. T4.
While taking levothyroxine at a dose of 125 mcg/day, the target values of thyroid hormones were achieved: TSH – 3.5 μIU/ml, st. T4 – 12 pmol/l.
Upon re-hospitalization eight months later, the patient noted a significant improvement in her health: appetite improved, weight increased by 10 kg, constipation, swelling and dry skin, and ascites disappeared.
On examination: hearing and speech were restored. Body temperature – 36.6 °C, body weight – 73.8 kg, height – 162 cm, body mass index – 28.4 kg/m2. Skin moisture was normal, there was no peripheral edema. The thyroid gland is not enlarged. Heart rate – 60 per minute, blood pressure – 90/60 mmHg. Art. No changes in the respiratory and cardiovascular systems were observed. The tongue is moist and clean. The abdomen is not enlarged and is painless on palpation. The liver is not enlarged, the spleen is not palpable. There is no free fluid in the abdominal cavity. Regular bowel movements, once a day.
The results of a general blood test indicate an improvement in indicators. Thus, the level of erythrocytes – 3.98 × 1012/l, leukocytes – 4.52 × 109/l, hemoglobin – 118 g/l, platelets – 216 × 109/l, eosinophils – 1.5%, neutrophils – 47.4 %, monocytes – 14.8%, lymphocytes – 35.6%, ESR – 24 mm/h.
In urine analysis according to Nechiporenko: level of leukocytes – 87.5 × 103, erythrocytes – 8.25 × 103, cylinders – 0. With bacteriological culture of urine: no population growth. This made it possible to diagnose a urinary infection. After a course of antibiotic therapy, urine analysis improved significantly.
There was a significant improvement in biochemical blood parameters: the level of total protein decreased to 83.5 g/l, liver and kidney function indicators, and lipid spectrum normalized. In particular, total bilirubin – 9.1 µmol/l, ALT – 11.8 U/l, AST – 24.4 U/l, urea – 8.1 mmol/l, creatinine – 85.7 µmol/l, potassium – 4.88 mmol/l, sodium – 140 mmol/l, cholesterol – 4.9 mmol/l, glycemic profile within normal limits, GFR – 67.7 ml/min/1.73 m2, albumin – 43.7 g /l, cortisol – 16.1 mcg/dl. Thyroid status corresponded to compensation of primary hypothyroidism: TSH – 1.27 µIU/ml, st. T4 – 17.2 pmol/l, AT-TPO – 79 U/ml.
According to the results of electrocardiography, sinus rhythm, heart rate - 61 per minute, signs of left ventricular hypertrophy, metabolic changes.
When conducting echocardiography: ejection fraction - 67%, the cavities and walls of the heart are of normal size, the valve apparatus without structural pathology. Regurgitation on the atrioventricular valves of the zero-first degree, accessory chord in the left ventricle. Systolic and diastolic functions of both ventricles are normal, heart rate is 64 per minute.
Ultrasound examination of the abdominal cavity and kidneys: the size of the liver is within normal limits, the contours are clear, the echostructure is moderately enhanced, homogeneous, the portal vein of the liver: the extrahepatic section is 11 mm (normal is up to 14 mm), there are no pathological formations. Conclusion: echoscopic signs of diffuse changes in the liver.
Replacement therapy with levothyroxine 125 mcg/day was continued. For the treatment of anemic syndrome, Sorbifer (one tablet per day), folic acid 1 mg (one tablet three times a day), vitamin B12 500 mcg (intramuscular once a week) are prescribed. For the treatment of urinary tract infections, amoxicillin in combination with clavulanic acid 1000 mg (one tablet twice a day for seven days) is recommended under the supervision of urine tests.
Discussion
As noted earlier, hypothyroidism syndrome is characterized by imitation of the manifestations of various non-thyroid diseases. In older patients, manifestations of hypothyroidism are often considered signs of normal aging. It is especially difficult to diagnose hypothyroidism when symptoms associated with isolated accumulation of fluid in the cavities come to the fore. The literature mainly describes cases of massive pericardial effusion in hypothyroidism [3, 7]. With hydropericardium, a high content of protein, cholesterol and mucin is found in the fluid. Cardiac tamponade is rare in hypothyroidism due to the slow accumulation of fluid [8, 9].
As part of polyserositis in hypothyroidism, hydropericardium and hydrothorax can be combined with ascites [1, 3, 10]. Ascites caused by myxedema is rare, but responds well to replacement therapy [6, 11]. If the cause of ascites is not identified and it is tolerant to various treatment methods, this may be a diagnostic criterion for myxedematous ascites [12, 13]. The patient we observed was unsuccessfully treated for ten years for ascites due to suspected liver cirrhosis, and after the prescription of thyroid therapy, it regressed within a few months.
Diagnosis of ascites in hypothyroidism is often delayed; patients undergo unnecessary examinations, such as liver biopsy, laparotomy, etc. [13]. JS Ji et al. described a clinical case of a 71-year-old patient whose first manifestation of hypothyroidism was ascites [6]. It resolved completely with replacement therapy. In Korea, 51 cases of ascites due to myxedema have been documented. In this case, a high level of protein in the ascitic fluid (more than 2.5 g/dL) and a low number of leukocytes with a high proportion of lymphocytes were noted [6]. Often, ascitic fluid takes on a gel-like appearance. In addition, a slow rate of accumulation and non-inflammatory nature of ascitic fluid are observed [14].
Laparocentesis is a fast, safe and low-cost method for diagnosing the cause of ascites. Before performing the procedure, a coagulogram study or correction of coagulopathy is not required [15]. The causes of ascites can be judged by the high or low level of protein in ascitic fluid obtained during laparocentesis [16, 17].
Initially, ascites in hypothyroidism was regarded as a manifestation of chronic right-sided heart failure due to cardiac fibrosis of the liver. However, normal pressure in the right ventricle of the heart was subsequently discovered [18–21].
Currently, there are two main theories for the development of ascites in hypothyroidism. The first hypothesis is that thyroid hormone deficiency causes an increase in capillary permeability and extravasation of plasma proteins into the extravascular bed [6]. The second is a direct hygroscopic effect associated with the accumulation of hyaluronic acid. It can interact with albumin to form complexes that alter lymphatic drainage. As a result, albumin clots form. High production of antidiuretic hormone cannot be ruled out. Decreased nitric oxide and high levels of vascular endothelial growth factor in hypothyroidism may lead to increased capillary permeability [22]. Oxidative stress activates inflammation and also affects capillary permeability. The serum-ascitic albumin gradient (SAAG) indicator is necessary to clarify the cause of ascites. To calculate SAAG, the difference between plasma and ascitic albumin concentrations is determined [15, 23]. High SAAG (more than 1.1 g/dl) occurs in portal hypertension in 97% of cases, low – in cirrhosis, malignant neoplasms, congestive heart failure, tuberculous peritonitis, alcoholic and purulent peritonitis, constrictive pericarditis, pancreatitis, liver metastases, nephrotic syndrome, Budd–Chiari syndrome. In hypothyroidism, SAAG can vary from low to high values [15]. Due to increased capillary permeability, as well as transudation of fluid and albumin not only into the interstitial space, but also into other cavities, hydropericardium, hydrothorax, and ascites can develop in patients with hypothyroidism [24]. Data on the amount of protein in ascitic fluid and the level of SAAG in patients with hypothyroidism, according to various sources, are presented in the table [6, 12, 13, 25, 26]. Thus, in most patients, the protein level in ascitic fluid was more than 2.5 g/dl, the average SAAH value was 1.5 g/dl. Most often, ascites is found in patients with newly diagnosed hypothyroidism. However, this may be a complication after stopping replacement therapy. S. Khalid et al. described the case of a 56-year-old female patient who suffered from Hashimoto's thyroiditis and hypothyroidism for 30 years. Six months after stopping levothyroxine, she developed ascites and severe peripheral edema [25]. The authors conducted an extensive examination to determine the etiology of ascites. As a result, cardiac pathology, hepatitis, tumor, vascular pathology, pancreatitis, and viral hepatitis were excluded as causes. Primary hypothyroidism was confirmed. In the ascitic fluid, an increase in protein content was recorded to 3.5 g/dl, SAAG - 0.9 g/dl.
Another clinical observation describes the case of a 64-year-old patient who abused alcohol, suffered from gastroesophageal reflux disease and hypothyroidism [24]. The patient did not take levothyroxine and omeprazole prescribed to him for several months. Two weeks before hospitalization, he received ibuprofen at a dose of 400–1200 mg/day for spinal pain, after which an episode of syncope, daily melena and gastric bleeding were noted. Physical examination revealed ascites for the first time. Upon admission to the clinic, the TSH level was up to 60 µIU/ml, st. T4 – 0 pmol/l. During FGDS, a clot is found in the distal esophagus. Laparocentesis and liver biopsy were performed. Liver cirrhosis was excluded. The hepatic-venous pressure gradient is normal. Portal hypertension was excluded. In ascitic fluid, the albumin content is 3.1 g/dl, SAAG is 1.9 g/dl. Bacterial culture of ascitic fluid is negative. Thus, ascites is regarded as myxedematous. The patient was given intravenous drips of levothyroxine and hydrocortisone. During replacement therapy with levothyroxine 300 mcg/day with dose titration to 150 mcg/day over eight days, ascites decreased. The patient continued to receive replacement therapy on an outpatient basis.
There is a close connection between the thyroid gland and the liver. On the one hand, thyroxine and triiodothyronine regulate the basal metabolism of hepatocytes. On the other hand, thyroid hormones are metabolized in the liver. Hypothyroidism can imitate liver pathology and directly affect its structure and function, causing an increase in AST, cholestasis against the background of decreased excretion of bilirubin and bile. In combination with hypercholesterolemia and hypotension of the gallbladder, the risk of developing cholelithiasis increases [18, 21, 27, 28]. Ascites in hypothyroidism, as in our case, is often differentiated from ascites in liver cirrhosis. Therefore, in the presence of liver pathology and in the absence of convincing data in favor of cirrhosis, it is necessary to examine the function of the thyroid gland.
In the pathogenesis of ascites in right-sided heart failure, central liver damage with the formation of congestive liver fibrosis is important. Increased capillary permeability and insufficient lymphatic drainage are observed [21]. In our patient, the possibility of a combined origin of ascites was not excluded - against the background of cardiac pathology and hypothyroidism, taking into account an episode of cardiac arrhythmia. Non-enlarged heart size according to echocardiography and normal ejection fraction allowed us to exclude congestive heart failure.
It is known that sinus bradycardia is a characteristic, but not obligatory sign of hypothyroidism. HE. Kryuchkova et al. described the possibility of developing a tachysystolic form of atrial fibrillation and atrial flutter in hypothyroidism [21]. In some cases, when alternating bradycardia and arrhythmia, sick sinus syndrome is mistakenly diagnosed. Prescription of antiarrhythmic drugs may aggravate hypothyroid arrhythmia [21].
Laboratory diagnostic signs of hypothyroidism include anemia, leukopenia, hyponatremia, hypochloremia, hypoglycemia, increased creatinine, creatine phosphokinase, transaminases, and lipids [1]. They, like the clinical symptoms, are nonspecific, therefore, in addition to liver cirrhosis and hypothyroidism, other somatic diseases had to be excluded in the patient. A noteworthy fact was the presence of hyperproteinemia in the patient; during the examination, paraproteinemic hemoblastosis was excluded. In the analyzed literature, no information was found on the development of hyperproteinemia in hypothyroidism. However, data on hyperproteinemia in many other somatic diseases is provided. Only in the experimental work of L. Ratzmann et al. It was shown that in rats with induced hypothyroidism (due to radiothyroidectomy or administration of thyreostatics), after four to seven weeks, higher levels of serum protein were observed compared to the control (p 1- and γ-globulin. Protein fractions changed depending on the duration of hypothyroidism. With it After seven weeks of compensation, protein fractions were restored [29].
Hypothyroidism affects kidney function. Due to a decrease in cardiac output and the development of arterial hypotension, renal perfusion and their filtration capacity are impaired. Tubular reabsorption, plasma renin activity, aldosterone and atrial natriuretic peptide levels also decrease, and sodium excretion increases [5, 30]. This leads to acute kidney injury [31]. Our patient also had impaired renal function with subsequent recovery of GFR due to compensation for hypothyroidism. In most cases, normalization of renal function begins in the second week from the start of thyroid hormone replacement therapy [31].
Conclusion
Despite the well-known clinical picture of hypothyroidism, doctors of different specialties need to remember the presence of different masks of hypothyroidism and examine the thyroid status in order to timely prescribe replacement therapy. Ascites is not an independent disease. This is one of the manifestations of various pathologies, including hypothyroidism. That is why its diagnosis must be approached comprehensively and comprehensively. Therapy with thyroid hormones leads to complete regression of myxedematous ascites.
Conflict of interest:
All authors declare that there are no potential conflicts of interest to disclose in this article.
Treatment of myxedema
Treatment of myxedema consists of correcting hormonal deficiency by supplying thyroid hormones from the outside. The dosage is calculated individually; the drug containing hormones is taken once a day.
If iodine deficiency is established, iodine preparations and a diet rich in iodine-containing foods (seaweed, sea fish and other seafood, walnuts, iodized salt) are prescribed.
Lost thyroid function is not restored, so treatment for myxedema must be lifelong.
Diagnostics
A specialist can make a primary diagnosis already at the stage of collecting an anamnesis. Warning factors are the patient's drowsiness, decreased performance, headaches, noticeable dry skin, shortness of breath, and impaired nasal breathing. The following measures for diagnosing myxedema can confirm the endocrinologist’s assumptions:
- General and biochemical blood test to clarify the content of proteins, cholesterol and iodine in the body, hemoglobin level and ESR.
- Hormonal blood test to determine the content of thyroxine and triiodothyronine. When hormone levels increase, experts talk about the primary form of the disease; when hormone levels decrease, they speak about secondary hypothyroidism.
- Scintigraphy of the thyroid gland, which allows you to determine the activity of glandular tissues. When the absorption of radioactive iodine decreases, the thyroid gland produces less hormones, and nodules form in its structure.
- Ultrasound of the thyroid gland to exclude malignant formations in its structure, calcifications and nodes. With hypothyroidism, there is often a decrease in the volume of the organ relative to its normal size.
Myxedema prognosis
The disease is characterized by a slow increase in symptoms, so if it is possible to diagnose myxedema in time and begin adequate treatment of myxedema, the disease will proceed benignly, although it will have to be treated for life. As for myxedema in childhood, the earliest possible recognition of the disease is of great importance, which is difficult in practice. With congenital myxedema, the prognosis is unfavorable; if it is early, it is possible to significantly improve the patient’s condition with hormone replacement therapy, but, as a rule, it is not possible to achieve complete elimination of the symptoms of myxedema.
Links[edit]
- ^ ab Berger, William D. James, Dirk M. Alston, Timothy G. (2011). Andrews Skin Diseases: Clinical Dermatology
(11th ed.). [London]: Saunders/Elsevier. ISBN 978-1-4377-0314-6. - Schneider, Arthur S.; Kim, Philip A. Szanto; with special contributions from Sandra I.; Swanson, Todd A. (2009). Pathology (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. P. 314. ISBN 978-1451109061.
- "Pretibial myxedema". Archived from the original on 2016-03-04. Retrieved March 27, 2009.
- ^ abc McConaughey, W. M. (March 1978). "Diagnostics and treatment of myxedema and myxedema coma." Geriatrics
.
33
(3): 61–66. ISSN 0016-867X. PMID 624451. - ^ ab Lindholm, J.; Laurberg, P. (2011). "Hypothyroidism and thyroid replacement: historical aspects". Journal of Thyroid Research
.
2011
: 809341. doi: 10.4061/2011/809341. PMC 3134382. PMID 21760981. - Vanderpas, Jean B.; Rivera-Vanderpas, Maria T.; Bourdoux, Pierre; Luvivila, Kapata; Lagasse, Raphael; Perlmutter-Kremer, Noemi; Delange, Francois; Lanoy, Leo; Ermans, Andre M. (1986-09-25). "Reversibility of severe hypothyroidism with iodine supplementation in patients with endemic cretinism." New England Journal of Medicine
.
315
(13):791–795. DOI: 10.1056/NEJM198609253151302. ISSN 0028-4793. PMID 3018564. - "Food Organs for the Treatment of Disease". Tacomed.com
. Archived from the original on September 6, 2021. Retrieved June 15, 2021.
Pretibial myxedema
Separately, it is necessary to consider a disease such as pretibial myxedema, or thyroid dermopathy. Unlike classic myxedema, pretibial myxedema occurs not with decreased, but with excessively increased thyroid function, the so-called thyrotoxicosis. The cause of thyrotoxicosis is most often diffuse toxic goiter, more popularly known as Graves' disease.
Pretibial myxedema has local manifestations, in contrast to ordinary myxedema, which manifests itself diffusely. A symptom of pretibial myxedema is the appearance of modified areas of skin on the lower part of the anterior surfaces of the legs. The skin in these areas becomes rough, thickens, acquires a red or purple-red color, and increased keratinization is noted. Protruding hair follicles appear on the affected areas of the skin, and subsequently the hair falls out.
External symptoms of pretibial myxedema are sometimes accompanied by a feeling of severe itching. Treatment of pretibial myxedema is carried out in combination with the correction of thyroid disorders that caused the disease. Local treatment of myxedema, when the disease is accompanied by itching, consists of using ointments containing steroidal anti-inflammatory drugs. In most cases, patients with pretibial myxedema are only concerned about a cosmetic defect, and then special treatment for myxedema is not carried out, but the underlying disease is treated.
Pathophysiology[edit]
Myxedema describes a specific form of cutaneous and cutaneous swelling secondary to increased deposition of connective tissue components. The connective fibers are separated by an increased amount of protein and mucopolysaccharides. These may include glycosaminoglycans such as hyaluronic acid, chondroitin sulfate and other mucopolysaccharides. [1] This protein-mucopolysaccharide complex binds water, causing swampy swelling without ulcers, especially around the eyes, hands, feet and in the supraclavicular fossa. Myxedema causes thickening of the tongue and the mucous membranes of the larynx and pharynx, leading to the slurred speech and hoarseness that is commonly seen with hypothyroidism.
Increased glycosaminoglycan deposition is not fully understood, but two mechanisms predominate:
- Stimulation of fibroblasts. Stimulation of fibroblasts by the thyroid-stimulating hormone (TSH) receptor is thought to increase glycosaminoglycan deposition, leading to osmotic edema and fluid retention. It is believed that many cells responsible for the formation of connective tissue respond to increased TSH levels. [ citation needed
] - Stimulation of lymphocytes. In Graves' thyroid disease, lymphocytes react against the TSH receptor by inappropriately producing thyroid-stimulating immunoglobulin (IgG; type II hypersensitivity). Lymphocytes react not only against thyroid receptors, but also against any tissue with cells expressing the receptor. This can lead to tissue damage and scar tissue formation, which explains the deposition of glycosaminoglycans. [ citation needed
]