general characteristics
Aldosterone is the main mineralocorticoid hormone of the adrenal cortex, a regulator of water-salt homeostasis. It is synthesized from cholesterol in the cells of the zona glomerulosa of the adrenal cortex. Under its influence, sodium retention occurs in the body (prevailing over water retention) and the release of potassium and hydrogen ions. The main regulators of aldosterone secretion are the renin-angiotensin system, which is activated in response to fluctuations in blood volume, as well as the level of potassium in the blood. Hyperkalemia stimulates and hypokalemia suppresses aldosterone production. In case of hypokalemia, it is necessary to compensate for the potassium deficiency before the study. The content of aldosterone in the blood changes throughout the day (the lowest concentration is around midnight) and depending on the position of the body (increases when moving to a vertical position). Aldosterone levels increase during the luteal phase of the menstrual cycle and during pregnancy. In patients over 60 years of age, aldosterone levels decrease by 50%, which is important to consider when interpreting the results. Increased salt intake leads to a decrease in blood aldosterone levels, while decreased salt intake leads to an increase in its concentration. Aldosterone is metabolized in the liver and kidneys. Also see Aldosterone-Renin ratio.
How to get tested
The analysis requires venous blood taken strictly on an empty stomach. The most suitable time for the procedure is from 8 to 11 am. Repeated studies should be carried out at the same time of day.
The main method for studying biomaterial is the enzyme immunoassay method (ELISA). Aldosterone in blood serum is detected by adding a labeled reagent to it. It binds only to this hormone and at the same time colors the entire test substance. The level of aldosterone is determined by the intensity of blood serum staining.
Patient preparation rules
venous blood
Standard preparation conditions (unless otherwise determined by the doctor):
2 weeks in advance Coordinate with the doctor the intake of: drugs from licorice root, diuretics, antihypertensive drugs, oral contraceptives.
For 3 days, meals without salt restriction. For 4 hours, withstand fasting, eliminate fatty foods. You can drink water. Be in an upright position (standing, sitting) for 2 hours. Sit at the manipulation table for 5 minutes. Notes:
attached.
ARS.pdf
You can add this study to your cart on this page
Clinical picture of aldosteroma - primary hyperaldosteronism
Clinical signs of primary hyperaldosteronism are represented by three main syndromes: cardiovascular (hypertensive), neuromuscular and renal.
Cardiovascular (hypertensive) syndrome of aldosteroma - primary hyperaldosteronism
Arterial hypertension is one of the most typical symptoms of primary hyperaldosteronism. It is observed in almost all patients with primary hyperaldosteronism, and in some cases it may even be the only clinical manifestation of this disease (Conn J. et al., 1964). Arterial hypertension is usually permanent. However, in some patients the increase in blood pressure takes the form of crises; Transient arterial hypertension is also possible.
Blood pressure levels range from moderately elevated numbers (150-160 and 90-100 mmHg) to very high (250-280 and 130-140 mmHg. The pathophysiological basis of such hypertension is sodium retention in tissues and hypervolemia, intimal edema, decreased vascular lumen, significant increase in peripheral resistance.In addition, the high sodium content in the walls of blood vessels and the depletion of cells in potassium increase the sensitivity of the vessels to the effects of pressor factors.
Neuromuscular syndrome of primary hyperaldosteronism
Disorders of the neuromuscular system in patients are caused mainly by hypokalemia, changes in the concentration gradients of extra- and intracellular potassium, potassium-sodium coefficient, intracellular acidosis, and ultimately - dystrophic changes in muscle and nervous tissues. Patients, as a rule, complain of pronounced muscle weakness, which is observed in 70% of cases. The degree of myasthenia gravis varies from moderate fatigue and fatigue to pseudoparalytic conditions. Myasthenia gravis can either be widespread or affect a specific muscle group, most often the lower extremities. Chvostek's paresthesias have been described (Weinberger M. et al., 1979)
Renal aldosteroma syndrome - primary hyperaldosteronism
Hypokalemia and hypernatremia are also the main cause of the development of kalipenic nephropathy, which is manifested by a decrease in the concentrating ability of the kidneys, polyuria, isohyposthenuria, nocturia, increased thirst and polydipsia.
Interference:
- Potassium-sparing diuretics, hyperkalemia, angiotensin, estrogens, laxatives with chronic abuse with the development of dehydration, diuretics, metoclopramide, oral contraceptives, thiazide diuretics, salt restriction, pregnancy, renovascular hypertension. Also see Aldosterone-Renin ratio.
- Beta blockers, central alpha 2 mimetics, non-steroidal anti-inflammatory drugs, ACE inhibitors, angiotensin receptor blockers, calcium channel blockers (dihydropyridine group), aminoglutethimide, etomidate, long-term heparin treatment, licorice, deoxycorticosterone, glucocorticoids, hypokalemia, renin inhibitors, excess salt , elderly age
Primary hyperaldosteronism (Conn's syndrome)
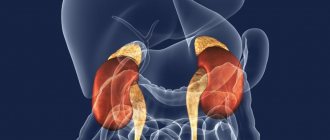
Fig.1. The location and blood supply of the adrenal gland is normal
Primary hyperaldosteronism (PHA) is a disease in which excess aldosterone production is autonomous, independent of the influence of various regulatory factors - in contrast to the secondary increase in aldosterone secretion that accompanies a number of diseases. Primary hyperaldosteronism is considered as an independent nosological form, while secondary hyperaldosteronism causes only a number of specific symptoms in diseases of the kidneys, liver and other organs of various etiologies and pathogenesis. There are no exact data on the frequency of PHA, since many patients do not come to the attention of endocrinologists. However, such patients make up a significant portion of those suffering from arterial hypertension.
Etiology and pathogenesis of aldosteroma - primary hyperaldosteronism
Morphologically, the substrate of primary hyperaldosteronism is an adrenal tumor, less commonly hyperplasia of the adrenal cortex. According to J.Conn (1955,1964), single adenomas (aldosteromas) occur in 70-90% of patients, multiple ones - in 10-15%, adrenal hyperplasia - 9%. In general, tumor lesions of the adrenal glands, as the cause of primary hyperaldosteronism, are observed in 85% of cases, and in 2-6% of patients they are malignant.
According to modern concepts, the prevalence of primary hyperaldosteronism (PHA) in patients with hypertension is 10-17% and up to 30% in secondary (symptomatic) hypertension. Aldosterone-producing adenoma is detected in 10-15% of all forms of PHA. It should be noted that in case of accidentally detected tumors, the incidence of aldosteroma is extremely low and does not exceed 1%, however, the largest number of unjustified adrenalectomies is associated with overdiagnosis of aldosteroma.
Primary hyperaldosteronism occurs mainly in adults. Aldosteroma in most cases is a single, clearly defined encapsulated tumor weighing 1-3 g, with a diameter of up to 3 cm. On a section, it is ocher-yellow, ocher-golden-yellow in color with a smooth surface.
Treatment of aldosteroma - primary hyperaldosteronism
Treatment of primary hyperaldosteronism caused by an aldosterone-secreting adenoma of the cortex of one of the adrenal glands is surgical. Medication methods are indicated for mild forms of the disease caused by bilateral idiopathic hyperplasia of the adrenal cortex, as well as during the period of preparing patients for surgery.
Surgical treatment of primary hyperaldosteronism caused by aldosteroma is the only radical treatment method and consists of removing the aldosteroma (partial with organ preservation or unilateral adrenalectomy).
Watch a video of operations for adrenal tumors performed by Professor K.V. Puchkov. You can visit the website “Video of operations of the best surgeons in the world.”
Patients, as a rule, do not require special preoperative preparation or hormone replacement therapy in the early postoperative period. The choice of surgical approach, operation, anesthesia and intensive care in patients with aldosteroma do not have any specific features.
In case of aldosteronism caused by diffuse nodular hyperplasia of the adrenal cortex, the indications for surgery have not yet been clearly developed and the existing opinions of surgeons are ambiguous.
The role of aldosterone antagonists in the treatment of cardiovascular diseases
Dear Vyacheslav Yurievich! Today we would like to talk to you about the role of aldosterone antagonists in modern cardiological practice and identify the patient population for whom the use of drugs in this group is most important.
The renin-angiotensin-aldosterone system (RAAS) plays an important role in the development and progression of cardiovascular diseases (CVD), and its importance is now generally recognized. Over time, new tissue and hemodynamic effects of its individual components and the final product of this chain, aldosterone, are determined. Aldosterone is a steroid hormone synthesized primarily in the adrenal cortex under the influence of angiotensin II. It is also present in the vascular wall, heart, brain and adipose tissue, which is responsible for its effects.
To understand the role of aldosterone, it is important to know that as a result of activation of aldosterone receptors in the distal tubules of the kidneys, the reabsorption of sodium and hydrogen ions increases in exchange for potassium ions excreted from the body, which causes antidiuretic effects, manifested by fluid retention in the body and an increase in blood pressure (BP) . Chronic activation of myocardial receptors is accompanied by the development of fibrosis and myocardial remodeling, which underlies the formation of chronic heart failure (CHF), which is the outcome of most CVDs. Also, hyperactivation of endothelial aldosterone receptors leads to remodeling of the vascular wall, media hypertrophy and endothelial hyperplasia. In addition, aldosterone activates the sympathetic division of the autonomic nervous system, increases free radical oxidation, which causes the development of inflammation, remodeling, apoptosis and fibrosis.
Thus, the prescription of aldosterone antagonists for various clinical conditions accompanied by symptoms of hyperaldosteronism is justified from a pathophysiological point of view; these drugs have long been successfully used in clinical practice.
As for patients who need to take aldosterone antagonists, these are primarily people suffering from CHF, arterial hypertension (AH), especially its resistant form.
These drugs are also used in the treatment of liver cirrhosis with edematous syndrome, nephrotic syndrome, hypokalemia and primary hyperaldosteronism. What aldosterone antagonists are used in modern cardiology?
The most widely used aldosterone antagonist is spironolactone, a structural analogue of aldosterone. This drug, called the BS-8109 molecule, was developed in the mid-1950s. Spironolactone as a potassium-sparing diuretic was used in patients with edema syndrome due to CHF and portal cirrhosis. It is the diuretic properties of high doses of Veroshpiron with simultaneous blockade of potassium and magnesium loss that have become the main indication for its use for a quarter of a century. These effects and the method of its use were described in detail in our paper with Academician N.M. Mukharlyamov, my teacher, a monograph on the treatment of CHF, published in 1985.
Then, in the 1980s, the presence of aldosterone receptors in the myocardium and vascular endothelium was proven. By the end of the twentieth century, aldosterone antagonists or, as they came to be called, mineralocorticoid receptor antagonists (MCRAs), began to be used as neurohormonal modulators in the long-term treatment of CHF. This was discussed in detail in our meeting with Academician Yu.N. Belenkov monograph on the rational treatment of CHF, published in 2000.
Already in the 1960s, spironolactone demonstrated its effectiveness in hypertension, but it became widespread in clinical practice as an antihypertensive agent only in the second decade of the 21st century.
Also used in cardiology is eplerenone, which is a chemical derivative of mexrenone, a metabolite of spironolactone. Spironolactone and eplerenone are competitive antagonists of mineralocorticoid receptors, but have varying degrees of selectivity for them.
There is another drug - canrenone, which is not registered in the Russian Federation.
Currently, the first non-steroidal aldosterone antagonist, Finnerenone, is undergoing the third phase of clinical trials. As we can see, interest in this class of drugs, despite the more than 60-year history of their use, is growing. What determines the effectiveness of spironolactone in the treatment of patients with CVD and what pharmacological characteristics does it have?
Spironolactone is a non-selective, competitive mineralocorticoid receptor antagonist. By blocking aldosterone receptors, it has a diuretic and natriuretic effect, while retaining potassium and magnesium ions in the body. Since a small amount of sodium is reabsorbed in the distal nephron, the diuretic effect of spironolactone is not very significant, but its diuretic effect is significantly enhanced when used with loop and thiazide diuretics.
Spironolactone is structurally similar to progesterone, and therefore it has the properties of a progesterone receptor agonist and a weak androgen and corticosteroid receptor antagonist, which can lead to such undesirable effects as gynecomastia, menstrual irregularities, decreased libido and hirsutism. However, it must be taken into account that adverse events are dose-dependent. Thus, in the large randomized clinical trial RALES, when treating patients with spironolactone in doses of 25–50 mg/day, the incidence of gynecomastia did not exceed 8.5%.
Spironolactone is a prodrug; its active metabolites, canrenoate and canrenone, are formed in the liver. The half-life of spironolactone is 13–24 hours, which is largely due to active metabolites that continue to act outside the therapeutic window. The time to reach maximum plasma concentration after morning administration is 2–6 hours. The drug is excreted primarily by the kidneys.
What evidence base exists for spironolactone in resistant hypertension and CHF?
Aldosterone antagonists, in particular spironolactone, block the negative effects of excessive activation of the RAAS at all stages of the cardiovascular continuum. At the same time, the benefits of using this drug for resistant hypertension and CHF are maximum.
When it comes to the management of patients suffering from hypertension, spironolactone is an important component in the treatment of resistant hypertension. Let me remind you that hypertension is considered resistant when it is not possible to achieve a decrease in office blood pressure <140/90 mmHg. Art. (according to 2021 recommendations - below 130/80 mm Hg for persons under 65 years of age) against the background of the use of recommended treatment tactics, which should include lifestyle modification measures and taking optimal doses of at least three drugs: a diuretic, an angiotensin-converting enzyme inhibitor ( ACE) or angiotensin receptor blocker and calcium channel blocker. If resistant hypertension is suspected, it is necessary to exclude secondary forms of hypertension and pseudo-resistance, the reasons for which may be low adherence to treatment, the “white coat” phenomenon, violation of the rules for measuring blood pressure, severe calcification of the brachial artery, the use of vasopressors or substances that promote sodium retention, and others.
According to the PATHWAY-2 study (Prevention And Treatment of Hypertension With Algorithm-based therapy number 2), spironolactone proved to be effective and safe in certain groups of patients with resistant hypertension, for example, sleep apnea syndrome, obesity, and chronic kidney disease. In this study, spironolactone, compared with bisoprolol and doxazosin, had the maximum hypotensive effect when added to a three-component combination of an ACE inhibitor (or angiotensin receptor blocker), a calcium antagonist and a diuretic in maximum doses.
Spironolactone has also played an important role in the treatment of heart failure for 40 years. It has been proven that hyperaldosteronemia negatively affects the prognosis and survival of patients with CHF due to the progression of CHF decompensation and increasing the risk of sudden death.
All patients suffering from CHF (in the absence of absolute contraindications) should receive ACE inhibitors to block the RAAS. However, it turned out that monotherapy with ACE inhibitors does not fully block the negative effects of the RAAS, which is due to the presence of ACE-independent pathways for the formation of angiotensin II (chymases and other enzymes). It is this effect of reducing the ability of ACE inhibitors to reduce aldosterone secretion, which we described back in the 1990s, that is called the “blockade slippage phenomenon.” Moreover, this phenomenon develops in patients regardless of the dose of ACE inhibitors and appears already by the third month of continuous treatment, which was first shown by our group in 1990. There is also evidence that with long-term use of ACE inhibitors in CHF, alternative pathways for stimulating aldosterone synthesis are activated, not associated with angiotensin II, but mediated by endothelin, antidiuretic hormone, corticotropin and histamine. The identification of these additional activators of aldosterone synthesis served to justify the advisability of using mineralocorticoid receptor inhibitors in combination with an ACE inhibitor (and beta-blockers) for a more complete neurohumoral blockade in the treatment of patients with CHF, which was confirmed by the results of randomized placebo-controlled studies.
The clinical validity of this hypothesis was confirmed in 1999 by the results of the double-blind, placebo-controlled RALES (Randomized ALdactone Evaluation Study) study. This study included patients with severe CHF (NYHA functional class III–IV) who received spironolactone 25–50 mg/day or placebo in addition to standard ACE inhibitor therapy at that time. , diuretics and cardiac glycosides (almost without β-blockers). The study was stopped early due to the apparent superiority of spironolactone over placebo. As a result of a three-year observation, it was shown that the use of spironolactone can significantly reduce the risk of death by 27%, the total number of hospitalizations by 18%, and the number of hospitalizations as a result of decompensated heart failure by 30%. Based on the results of the RALES study, spironolactone was included in European, American and Russian clinical guidelines for the treatment of patients with CHF.
Thus, aldosterone antagonists have long and widely entered clinical practice and have not given up their positions for many years, however, it is important for practicing physicians to remember that these drugs are often left “overboard”, despite their extensive evidence base.
In the US and Europe, for example, these drugs are prescribed to only a third of patients who need them. In Russia, during inpatient treatment, slightly more than half of patients with CHF and LVEF <40% take AMCR, but when moving to the outpatient stage of treatment, according to the EPOCHA study conducted in 2021, only 14% of patients take spironolactone. At the same time, not only do patients not take or stop taking aldosterone antagonists, but doctors also do not prescribe these drugs often enough. What place do aldosterone antagonists currently occupy in clinical guidelines?
In the 2021 European clinical guidelines for the management of patients with hypertension, an important role in the treatment of resistant hypertension is assigned to AMCR as the main “assistant” of the main antihypertensive therapy, including RAAS blockers + slow calcium channel blockers + diuretics. This document notes that fourth-line therapy at the third stage should include spironolactone at a dose of 25–50 mg/day. The main studies on the treatment of resistant hypertension were carried out with spironolactone. Emphasis is also placed on the need to monitor potassium levels and glomerular filtration rate (GFR) of the kidneys. In patients with resistant hypertension, spironolactone is prescribed when GFR is ≥45 ml/min/1.73 m2 and plasma potassium concentration is ≤4.5 mmol/L. The recommendations published by the Russian Society of Cardiology and approved by the scientific and practical council of the Ministry of Health of the Russian Federation at the beginning of 2021 also state that all patients with resistant hypertension are recommended to add spironolactone to their therapy in doses of 25–50 mg/day to achieve the target blood pressure level. However, the use of spironolactone is contraindicated in patients with GFR ≤30 ml/min/1.73 m2 and plasma potassium concentration ≥5 mmol/L due to the risk of hyperkalemia. In this case, it is recommended to use loop diuretics.
Regarding heart failure, the 2021 European guidelines for the diagnosis and treatment of acute and chronic heart failure indicate that spironolactone is recommended for all patients with NYHA functional class II–IV CHF (despite treatment with ACE inhibitors and beta-blockers) with reduced LVEF ≤ 35% to reduce mortality and hospitalization for heart failure. This drug should be prescribed with caution to patients with impaired renal function (creatinine >221 µmol/l or GFR <30 ml/min/1.73 m2), for which regular monitoring should be carried out depending on the clinical status of the patient, and potential drug interactions. The starting dose of spironolactone is 25 mg/day, the maintenance dose is 50 mg/day, the dose is recommended to be increased after 4–8 weeks of therapy. The recommendations also specifically indicate the need to inform the patient that this treatment is being carried out to improve his well-being, survival and prevent worsening of heart failure and reduce the number of hospitalizations; that symptomatic improvement while taking aldosterone antagonists does not occur immediately - it should take from several weeks to several months from the start of treatment; that it is necessary to avoid taking non-steroidal anti-inflammatory drugs not prescribed by a doctor and salt substitutes with high K+ content.
From my point of view, an accessible explanation to the patient of the mechanisms of action and the reasons for prescribing these drugs to him is a very important stage of treatment, helping to improve communication between the doctor and the patient and increase adherence to treatment.
In the joint recommendations of the Society of Specialists in Heart Failure (OSHF) - the Russian Society of Cardiology (RKO) and the Russian Scientific Medical Society of Therapists (RNSOT) from 2021, indications for the use of spironolactone (25-50 mg / day) are severe CHF III-IV class and cases of acute circulatory decompensation when the drug is used in high doses.
For CHF (starting from class II) and in patients who have suffered acute myocardial infarction, with left ventricular dysfunction, the use of AMCR (spironolactone or eplerenone) in doses of 25–50 mg/day is indicated. It was also noted that in the presence of an elevated creatinine level >130 µmol/l, a history of renal failure, a decrease in GFR <30 ml/min/1.73 m2, hyperkalemia (even moderate - >5.2 mmol/l), a combination of aldosterone antagonists with ACE inhibitors requires careful clinical and laboratory monitoring. It is necessary to monitor the level of potassium and serum creatinine and the calculation of GFR after 2 and 4 weeks, then after 2 and 3 months of treatment, and then once every six months, which minimizes the number of adverse reactions. What should a physician keep in mind when prescribing spironolactone to his patients?
When treating decompensation, it is impossible to effectively and safely carry out dehydration therapy without using high doses of spironolactone as a potassium- and magnesium-sparing diuretic.
With long-term therapy, only the use of the tactics of “triple neurohormonal blockade” actually prolongs the life of patients and improves its quality. The physician must explain the goals of therapy to his patients. This is the only way to influence adherence to therapy and increase the number of patients taking spironolactone. As already mentioned, now their share is unacceptably small - only 14%.
Finally, it must be remembered that one in three hypertensive patients fails to achieve their BP-lowering goals with the three main antihypertensive medications. The solution to the problem is the use of AMKR, and their effectiveness increases with increased salt consumption (the scourge of the Russian population) and non-reduction of blood pressure at night.
The quality of the drug taken also plays an important role. Thus, the first spironolactone to appear on the pharmaceutical market of the Russian Federation was Veroshpiron, a drug. Currently in Russia, Veroshpiron is a reference and non-interchangeable spironolactone, which we can recommend to our patients.
Thus, despite the emergence of new drugs that have the ability to block the effects of the RAAS or other mechanisms of hypotensive action, spironolactone not only has not lost its position, but continues to demonstrate effectiveness in various clinical situations.
Gratitude
The editors would like to thank Gedeon Richter Pharma LLC for their assistance in organizing and conducting this interview.
Decreased aldosterone levels
With aldosterone deficiency in the kidneys, sodium concentration decreases, potassium excretion slows down, and the mechanism of ion transport through tissues is disrupted. As a result, the blood supply to the brain and peripheral tissues is disrupted, the tone of smooth muscle muscles is reduced, and the vasomotor center is inhibited.
Hypoaldosteronism requires lifelong treatment; medication and limited potassium intake allow compensation for the disease.
Hypoaldosteronism is a complex of changes in the body caused by a decrease in the secretion of aldosterone. There are primary and secondary hypoaldosteronism.
Primary hypoaldosteronism is most often congenital in nature, its first manifestations are observed in infants. It is based on a hereditary disorder of aldosterone biosynthesis, in which sodium loss and arterial hypotension increase renin production.
The disease is manifested by electrolyte disturbances, dehydration, and vomiting. The primary form of hypoaldosteronism tends to spontaneously remit with age.
Secondary hypoaldosteronism, which manifests itself in adolescence or adulthood, is based on a defect in aldosterone biosynthesis associated with insufficient production of renin by the kidneys or reduced renin activity. This form of hypoaldosteronism often accompanies diabetes mellitus or chronic nephritis. The development of the disease can also be facilitated by long-term use of heparin, cyclosporine, indomethacin, angiotensin receptor blockers, and ACE inhibitors.
Symptoms of secondary hypoaldosteronism:
- weakness;
- intermittent fever;
- orthostatic hypotension;
- cardiac arrhythmia;
- bradycardia;
- fainting;
- decreased potency.
Sometimes hypoaldosteronism is asymptomatic, in which case it is usually an incidental diagnostic finding during examination for another reason.
There are also congenital isolated (primary isolated) and acquired hypoaldosteronism.