Cervical dysplasia - CIN - cervical intraepithelial neoplasia - SIL (squamous intraepithelial lesion) - a precancerous condition. This diagnosis is made to approximately 10 thousand women a year, while 6,000 patients ultimately die from cervical cancer. The reason is a late visit to a gynecologist, when the well-treatable stages of CIN1 and CIN2 turned into difficult-to-treat CIN3.
Consultation with a gynecologist, urologist - 1000 rubles, consultation on the results of ultrasound, tests - 500 rubles. (optional).
What is cervical dysplasia, causes
The content of the article
Cervical cancer does not begin suddenly; it is preceded by 3 precancerous stages of dysplasia, when several layers of cells of the squamous epithelium (lining skin) of the cervix undergo changes. Gradually, normal epithelial cells replace atypical - modified ones. They have a different structure, size and change their location. As a result, the epithelium is transformed from multilayered, easily renewed, into single-layered.
It has been established that the main cause of dysplasia is the human papillomavirus, or rather its oncogenic types - sexually transmitted serotypes 16 and 18. At the same time, dysplasia does not start out of nowhere - it is preceded by cervical erosion, which women often ignore, not wanting to treat. In other words, dysplasia is a complication of erosion. Untreated erosion turns into dysplasia in 90% of cases.
This is due to the fact that the virus freely infects immature germ squamous epithelial cells located in the erosion zone. Such zones are called transformation zones, therefore the most important stage in the treatment of erosion is the treatment (closure) of these zones using various methods. Modern clinics use laser and radio techniques. After treatment with a radioknife or laser, all affected cells are removed, closing the path for dysplasia
Prevention of dysplasia
- HPV is considered the main cause of dysplasia, so the most important thing is to try to prevent the virus from appearing in a woman’s body. Today, vaccination with Cervarix or Gardasil can protect against HPV. To give up smoking. According to statistics, cervical dysplasia and cancer are twice as common in women who smoke, and passive smoking also increases the risk.
- Proper balanced nutrition, including essential vitamins and minerals. You need to add more greens, fresh fruits and vegetables to your diet. Products containing vitamins B, A, C and E, foods with a high content of beta-carotene, and green tea are useful. Lemons, nuts, rose hips, wheat, salmon, squid, sorrel, and cereals are recommended.
- Regular consultations with a gynecologist, cytological examination.
- Use of barrier methods of contraception during casual sexual intercourse.
- Timely treatment of inflammatory gynecological diseases.
This article is posted for educational purposes only and does not constitute scientific material or professional medical advice.
Stages and symptoms of cervical dysplasia: CIN 1, CIN 2, CIN 3 - what is it?
Dysplasia is more common in women over 25 years of age, when the immune system is weakened due to changes in sexual partners, which forces the vaginal flora to constantly change, childbirth and other reasons. The peak incidence occurs at 35 years of age. At the same time, the risk of developing cancer still exists after age 65. English scientists from Keele University have proven that HPV, which enters the body at a young age, may not manifest itself for years or decades, becoming more active after menopause.
The disease is asymptomatic for a long time, being discovered by chance during a gynecological examination.
In rare cases, the following symptoms may appear in the precancer stage:
- vaginal discharge (spotting);
- discharge after sexual intercourse;
- intermenstrual bleeding;
- pain in the lower abdomen.
The absence of clear typical signs makes the pathology especially dangerous. Women who neglect preventive examinations by a gynecologist are at great risk.
The stages of dysplasia are abbreviated as CIN. To understand the essence of the process by stages, consider the table.
| Stage of cervical dysplasia CIN (Cervical Intraepithelial neoplasia) | Ongoing process | Cure prognosis |
| CIN 1 (CIN 1) - first stage of pathology, mild, initial degree | The changes are mild, covering less than a third of the thickness of the epithelium, measured from the basement membrane | Grade 1 dysplasia rarely leads to malignancy (malignancy). The disease goes away after treatment for HPV. Completely curable. |
| CIN 2 (CIN 2) - second stage of pathology, moderate severity | The structure of epithelial cells changes significantly and is well expressed. Changes affect half the layer thickness | Completely curable |
| CIN 3 (CIN 3) - third stage of pathology, severe | More than ⅔ of the squamous epithelial cells lining the cervix changes | Grade 3 dysplasia transforms into cancer in almost 100% of cases throughout the year. Difficult to treat, often not completely curable |
Dysplasia requires immediate treatment; without it, it easily changes stages, reaching stage CIN 3, which can already be considered cancer. A more accurate name is local cancer, “cancer in place,” i.e. still has metastasized, which leaves hope for a cure. The first stages of precancer SIN 1 and SIN 2 are completely curable with proper therapy.
Signs and symptoms
In 10-15% of cases of grade 2 cervical dysplasia, symptoms practically do not appear. The disease passes in a latent form and is diagnosed during a routine visit to the doctor. Obvious signs can appear only if atypical changes are accompanied by the influence of an infectious agent, viruses or fungi. In this case, the first signs of the development of the disease are similar to endocervicitis or colpitis:
- Itching and burning in the vaginal area.
- Copious discharge with an unpleasant odor and blood clots.
- Discharge that appears after sexual intercourse.
Pain is not typical for dysplasia. If the immune system is in a normal state, then after some time the signs of the inflammatory process will disappear. Against the background of gonorrhea, condylomatosis or chlamydia, grade 2 cervical dysplasia has more specific symptoms and treatment.
What do the terms CIN and SIL mean?
In medicine, the diagnosis of cervical dysplasia is called differently. To make the diagnosis clear throughout the world, a unified classification of the stages of the process was introduced. Dysplasia was originally designated as CIN, which stood for cervical intraepithelial neoplasia. More accessible is the development of a tumor within the epithelial layer.
When SIN develops into cervical cancer, the process takes a different turn - atypical cells grow inside the tissue, extending beyond the epithelium. The tumor also gives metastases, this CIN is different from cancer. In 2012, WHO introduced a different terminology - CIN was replaced by SIL - squamous intraepithelial lesion. The concept of neoplasia has changed to the more objective term “lesion.” There were only 2 degrees left - a mild degree of damage - LSIL (Low grade SIL) and a severe degree of damage - HSIL (High grade SIL). LSIL is equated to dysplasia 1 (CIN 1), and HSIL to dysplasia 2-3 (CIN 2 and 3). Many specialists still use the first classification, as it more accurately characterizes the scope of the process and allows you to choose the most gentle treatment.
Nutrition for mild dysplasia
The most important component for cervical neoplasia is dietary nutrition, which, in combination with therapeutic measures, significantly improves the prognosis for this pathology. Any disease occurs against the background of a reduced immune status. Therefore, to support immunity, the diet includes foods containing ascorbic acid, which helps stimulate metabolism, hematopoietic processes, and recovery. Black currants, kiwi, parsley, cabbage, citrus fruits, and walnuts are useful. You need to drink more decoctions of rose hips, dried fruits, herbs with an anti-inflammatory effect, add honey to drinks if there are no contraindications.
It is believed that homocysteine (an amino acid) aggravates dysplastic processes, and folic acid reduces the concentration of this substance. In addition, vitamin B9 improves hematopoiesis and promotes the restoration of epithelial tissue. Folic acid is sufficiently contained in cottage cheese, liver and beef, soy, lemons, beans, porcini mushrooms and Brussels sprouts, egg yolks, and hard cheeses.
According to medical research, beta-carotene reduces the risk of cervical cancer, is involved in cellular metabolism, and has an antiviral effect. There is a lot of vitamin A in orange-colored foods, natural butter, liver, egg yolks, and sea fish.
Tocopherol is a powerful antioxidant that is used to prevent the development of cancer against the background of cervical dysplasia, increases the concentration of red blood cells, helps with cardiovascular disorders, and slows down aging. The vitamin of youth is found in walnuts, almonds, brown rice, oils (corn, unrefined sunflower, wheat germ, soy).
If you have cervical neoplasia, you should not eat spicy and fried foods, smoked and pickled foods, processed and fast foods, foods rich in simple carbohydrates, dietary supplements, and alcohol. Optimal diet: cereals, nuts, dried fruits, vegetables, honey, decoctions, dairy products.
Examination for cervical dysplasia: how to identify CIN 1, CIN 2, CIN 3
Diagnosis of cervical dysplasia throughout the world is carried out according to the standards recommended by the World Health Organization. In Russia, good clinics use the following screening scheme for dysplasia:
- Examination by a gynecologist using a colposcope
(examination of the cervix under a gynecological microscope with high magnification). - Cytological smear - Pap test (taken by a gynecologist during an examination). The smear includes epithelial cells, which are then examined in the laboratory under a microscope. Atypical cells are identified: quantity, quality.
- Cervical biopsy
. This is an additional clarifying examination, carried out in case of poor smear results for cytology and colposcopy. - Blood for tumor markers
. If cancer is already present, this will be visible from the results of blood tests for oncology.
The first two examinations for syn1, syn2 and syn3 are included in the mandatory cancer prevention program in gynecology. Colposcopy and cytological smear should be performed at least once every three years, starting from the age of 25. This program is called cancer screening.
Diagnostics
Instrumental and laboratory research methods are placed at the forefront in the diagnosis of mild cervical dysplasia, due to the absence of pronounced specific manifestations. After interviewing the patient, collecting anamnesis, and studying the medical record (if available), the doctor examines the cervix with vaginal speculum. Visually, a specialist can detect atypical areas of the epithelium that have an unusual color, spots, and unevenness of the epithelial surface.
Colposcopy is an instrumental way of examining the cervix using a binocular optical device (colposcope), which magnifies the area being examined by 10 times or more. The usual visual examination is a simple colposcopy. During extended colposcopy, diagnostic tests are performed using acetic acid, Lugol's solution (Schiller test), and other reagents. The study is based on the reaction of affected areas of the epithelium to chemical solutions. The study is informative, painless, takes little time, and allows you to quickly identify characteristic changes in the cervix.
Ultrasonography of the pelvic organs is the most informative transvaginal examination; during pregnancy, diagnostics are carried out using an abdominal sensor. During the examination, foci of inflammation, condylomas, tumor-like formations are identified, and the condition of the uterus and its appendages is assessed. If necessary, blood flow in the reproductive organs is assessed (Doppler mode).
Pap smear (Papanicolaou test) is a method of liquid cytology of the cervix and cervical canal, a highly accurate test that allows you to detect precancerous changes. A special cytobrush is used to scrape the area under study and place the material on glass (1-3 glasses are used) in the form of a smear-imprint. The biomaterial on the glass is dried and fixed with a fixative. The drug prepared in this way is placed in a package, a direction is attached, and sent for laboratory testing. In order for the PAP test result to be correct, you need to prepare for the analysis according to the rules. It is recommended to abstain from sex two days before taking a smear; you cannot use vaginal tampons, medications (suppositories, gels, tablets), you cannot douche, or take a hot bath. During menstruation and inflammation, the test is not performed. A smear is taken either before an instrumental examination (including colposcopy) or two days after it.
Test results are interpreted by class:
- the first is a cytological norm;
- the second is a morphological change in cells associated with inflammation;
- third - single altered cells with abnormal nuclei and cytoplasm, suspicion of malignancy;
- fourth - the presence of cells with signs of malignancy;
- the fifth is malignant neoplasm.
The sensitivity of the cytological test is 65-90%. The higher the degree of neoplasia, the higher the accuracy of the study results.
To establish cervical dysplasia, a histological examination of a fragment of suspicious tissue obtained during a biopsy is required. The procedure is carried out during colposcopy, an optical device allows you to more accurately determine the area of tissue from which the biopsy is taken; sometimes fragments are taken from several sectors. The collection is not particularly difficult and usually does not require anesthesia. With careful tissue sampling, the patient feels short-term minor pain.
Unlike oncocytology, when taking biopsy material, deeper layers of the epithelium are affected. The biopsy is placed in a sterile tube with a solution, a direction is attached, and sent to the laboratory. The resulting tissue is stained in the laboratory and examined under a microscope. When stained, atypical cells do not change color or change slightly; normally, the cervical epithelium has a pale pink tint. With neoplasia, cells change the shape and number of nuclei. Mononuclear round cells become shapeless, enlarge, many small nuclei appear, and gradation disappears between the layers of the epithelial layer. Healthy squamous epithelium has several layers: basal-parabasal (deepest), intermediate, functional (upper).
The PCR test is necessary to identify papillomavirus, establish its strains, and assess the concentration of the pathogenic microorganism. A smear is taken from the mucous membrane of the neck, in which the DNA of the virus can be detected. The procedure is non-traumatic, does not cause pain, and takes a few minutes. It is advisable not to take antiviral and antibacterial drugs at least three days before the study, and also not to use personal hygiene products with an antibacterial effect, lubricants, vaginal suppositories and tablets. During menstruation and 2-3 days after it, the analysis is not taken. The treatment of grade 1 cervical dysplasia depends on whether HPV is detected, what the viral load is, and what types are detected.
Immunological analysis is carried out due to the high level of immune activity of cervical cells. This is due to the anatomical location of the organ, which is a kind of “border” between the vagina with its microflora and the uterus, which must remain absolutely clean. Cervical mucus is analyzed for the content of protein compounds (immunoglobulins, antibodies). An increase in the level of antibodies in the mucus indicates the presence of an inflammatory process. In a chronic course, the production of antibodies decreases, exhausted epithelial cells stop producing immunoglobulins, that is, they are deprived of protection.
Evaluation of biopsy results for SIN 1, 2 and 3
The diagnosis of dysplasia is made by the presence of atypical cells in a cytology smear and the identified loss of the possibility of normal maturation of stratified squamous epithelial cells due to increased proliferation (accelerated division) of cells.
Dysplasia first degree (LSIL, CIN 1)
In grade 1 dysplasia, HPV invades cells, gradually changing the structure of cells, causing acceleration of their growth. Moreover, this applies not only to erosion; a similar process leads to the formation of genital and flat condylomas. With strong cellular immunity, after removal of condylomas, the process is inhibited. Since the papillomavirus penetrates into the genome of cells, it is impossible to cure it, which is why erosion and papillomas are removed using different methods, trying not to leave affected cells.
Dysplasia second - third degree (HSIL, CIN 2-3)
The development of the dysplastic process directly depends on the patient’s immunity. And even with treatment started in these stages, the infection remains and progresses in 10% of women, which guarantees the development of cancer. At the same time, the speed of development of the process can be different and reach up to 15 years. For this reason, if a woman has been diagnosed with CIN 1 at least once, she will have to monitor the condition of her cervix throughout her life.
Cell changes in stages CIN 2-3 are only neoplastic in nature - i.e. they are completely transformed, and the boundaries of the process are expanded. The number of atypical cells prevails; they multiply rapidly, replacing the normal epithelial layer of the cervical glands and even the canal.
How to diagnose grade 2 dysplasia
Moderate cervical dysplasia does not have pronounced clinical signs, and therefore most often the diagnosis is made accidentally during a routine examination by a gynecologist.
The specialist examines all the woman’s complaints and conducts an examination in a gynecological chair. During the initial examination, the specialist may notice minor changes in the mucous membrane such as redness, shine around the circumference of the pharynx, changes in the structure of the epithelium, and the presence of spots.
The following additional research methods are used:
- Extended colposcopy
. The procedure involves examining the internal genital organs using a special magnifying device. The doctor examines the mucous membranes of the vagina and uterus. During colposcopy, tests with acetic acid and Lugol are performed to identify altered areas of tissue. Exposure to low concentrations of acetic acid helps reduce blood circulation, and Lugol changes the color of glycogen capsules. Healthy areas completely change color, but damaged areas do not.
- Cytological examination
. A smear is taken for analysis during a routine gynecological examination. If HPV is detected in a woman’s body, acanthosis (keratinized cells with a binuclear structure) will be observed in the smear. The analysis shows that cells affected by the virus lose their shape and significantly increase in size.
- Biopsy
. The diagnostic procedure involves obtaining a sample of materials for further histological examination. A biopsy is usually performed during a colposcopy. Tissue analysis gives doctors information about the condition of the cells and layers of the epithelium. This analysis allows you to determine the degree of tissue damage and the stage of dysplasia.
- PCR analysis
. This analysis allows you to detect the presence of HPV in the body and determine what load it creates. The study allows us to assess the risks of developing an oncological process in the cervix by identifying antique cells. PCR testing is prescribed for women over 30 years of age who are at risk of contracting HPV, as well as girls over 21 years of age who are also at risk.
If the main diagnostic methods did not detect changes, but the doctor still has doubts, then the woman may be prescribed a bacterioscopy. This analysis determines the type of pathogen. Additionally, the doctor can issue a referral for ELISA.
If moderate cervical dysplasia is associated with erosion and the doctor suspects the malignant nature of the changes, differential diagnostic methods can be practiced. They allow you to identify destruction in the mucous membranes and track accelerated tissue growth.
How to treat cervical dysplasia in different stages
How treatment will be carried out depends on the degree of dysplasia.
| Stage of cervical dysplasia | Diagnostics to confirm and monitor dynamics | Treatment Options | Forecast |
| Analysis result: CIN 1 | Cytology smear every 3 months. Colposcopy. HPV analysis - oncogenic types. Additional examinations for inflammation, hormonal disorders and genital infections. | Waiting tactics. Antiviral therapy. Stimulation of immunity. Treatment of all concomitant diseases. Removal of condylomas. If the CIN 1 test is poor for more than one and a half years, removal of the affected tissue is required. | Complete cure |
| Analysis result: CIN 2 | In-depth examination: biopsy, Schiller test, endocervical curettage | The following are prescribed: cryotherapy, PDT, cauterization with electric current, or more modern gentle but very effective techniques - laser therapy or radiotherapy; in case of significant damage, excision with a loop or conization of the cervix. For CIN 2 and 3, the above methods should be used; the uterus is removed only if it is ineffective. | Complete cure |
| Analysis result: CIN 3 | In-depth examination every 3 months: cervical biopsy, extended colposcopy, endocervical curettage | Laser therapy, radiotherapy, excision, conization of the cervix. If cervical cancer begins and treatment does not help, the uterus will have to be removed. | Depends on many factors: the state of the body, the degree of damage, previously and currently used treatment tactics, etc. |
For pregnant or nulliparous women, expectant management is possible for CIN 2 and 3, provided the coverage area is small. But throughout the entire period of pregnancy, you need to regularly take cytology tests and undergo colposcopic examination.
Cervical cancer: a preventable disease
Cervical cancer is merciless. More than 500,000 new cases of cervical cancer are registered annually around the world, and about 53% of women die. In our country, this cancer kills 21 women every day. We know a lot about this disease, because the cervix is an organ that is quite accessible to examination. Why are we still diagnosing things too late?
Cervical cancer
A disease with a well-studied and proven cause. In 2008, Harald zur Hausen won the Nobel Prize for proving the connection between HPV infection (human papillomavirus) and the development of cervical cancer. Back in 1983, he managed to discover the most aggressive type of virus - HPV-16. Over 34 years of research, which involved more than 10,000 patients, it was proven that 95% of cervical cancer cases are associated with one of the types - HPV-16 or HPV-18.
As always, a new idea captured hearts and minds. Thousands of doctors then rushed to look for HPV in millions of women, followed by monstrous attempts to get rid of the pathogen at any cost. In my memory, dozens of drugs came onto the market with the promise of “cure HPV forever.” Enthusiastic reviews gave way to bewilderment and disappointment. Each subsequent medicine became more expensive than the previous one, each was accompanied by evidence of effectiveness in the form of studies of varying degrees of homegrown. I can safely say that we have definitely achieved only one effect - we have created HPV hysteria in the space around us.
“HPV cure” has become so popular that I am no longer surprised by claims that someone was cured of HPV with cow pats or Allokin-alpha.
Time for the big scare
Now it is obvious to most specialists: HPV is highly contagious; most sexually active women with more than one partner encounter HPV at least once in their lives. HPV is an epitheliotropic virus. It lives in the thickness of the epithelial layer on the cervix, vaginal walls or on the skin of the external genitalia. Moreover, we often see the place of its “registration” through a colposcope, and the results of vital activity in the form of atypical cells end up in cytological smears.
Women who have been diagnosed with HPV often cry in my office. Their last hope is for a “magic pill” that will cure the evil virus. In fact, there is no reason for tears yet.
In most cases, HPV infection does not require any treatment at all, because the virus is spontaneously eliminated - it leaves the body on its own without any treatment along with the exfoliating cells of the stratified squamous epithelium.
If the HPV test is positive, but there are no colposcopic and cytological signs of damage, no treatment is required.
The senseless and merciless use of immunotherapy drugs for the latent form of HPV infection causes damage not only to the wallet, but also, possibly, to the body. Admittedly, our actions in relation to the immune system are suspiciously reminiscent of the pirouettes of a bull in a china shop. We can’t even proudly boast: “I cured Ivanova’s latent form of HPV!” Because it is impossible to prove why the virus left the body. Either he did it voluntarily, or he somehow got bored with our medicinal shamanism.
The younger the woman, the higher the likelihood of spontaneous elimination. Most experts consider it inappropriate to routinely test sexually active women under 25 years of age for HPV. However, these patients with latent forms of HPV require careful monitoring. We will have to repeat the examination once or twice a year to make sure that HPV has left the body. The average time for self-elimination of the virus is 1.5 years.
If the same type of HPV was detected three times over the course of 1.5–2 years, we can talk about persistence. Persistence can also be suspected if the viral load is high in women over 30 years of age. This in no way means that the patient has cervical cancer or its prestages, but, of course, indicates a significant risk and requires the same thing - careful monitoring.
Persistence of HPV without colposcopic and cytological signs of damage is not a reason for treatment.
And then, like Khoja Nasreddin: either the donkey dies or the sultan dies. Either HPV will leave the body, or we will still “catch” changes in cytology or colposcopy.
Why get tested?
Firstly, in order to identify a favorable group - women without HPV. They can be invited for screening less often (provided they have a monogamous sexual relationship); the risk of developing cervical cancer in this group is minimal.
Already in 2009, it was possible to prove that HPV-negative CIN (pre-stage cervical cancer) is impossible. If the results of a cytological examination indicate a precancerous condition of the cervix, and tests for HPV are negative, then someone is mistaken.
I often offer the mantra to my patients: “No HPV, no cervical cancer.” However, it must be remembered that the human factor has not been canceled. Errors when taking material for research, errors during storage and transportation, and errors during research can create a picture of false well-being. HPV testing is not the gold standard. Everything should be assessed in combination with cytology and colposcopy.
Who really needs HPV testing:
- patients with unclear results of cytological smears;
- after surgical treatment of precancerous diseases of the cervix - CIN;
- as a regular screening for patients over 25 years of age;
- with questionable results of colposcopy.
Cervical cancer develops very slowly. From the moment HPV enters the body to the development of cancer, years, and sometimes even decades, pass. At first, the activity of the virus is almost invisible, but as soon as it is integrated into the genome of the cells, we will see characteristic changes in cytological smears. Koilocytes ("empty" cells typical of HPV infection) and dikaryosis (various disorders in the cell nucleus, multinucleated cells) appear. This stage can last from 3 to 20 months.
Under unfavorable conditions, real cancer cells appear on the lower layers of the epithelial layer, where the most active cell division occurs. This is CIN I (mild dysplasia or grade 1 cervical intraepithelial neoplasia). As scary as it sounds, CIN I is not cancer; it develops many years before actual cancer.
In stage CIN I, the disease is reversible.
For young women and/or women planning pregnancy, we have the right to continue observation for 1.5 to 2 years. If the process is not going to regress, treatment is carried out. Drug therapy is ineffective and can be used either as an auxiliary method or not at all. And treatment is the complete removal of the lesion: excision (removal of the affected area) or conization (removal of a cone-shaped fragment of the cervix).
On average, CIN I turns into CIN II–III in 3–5 years (of course, the process will be much faster with concomitant HIV infection, chlamydia or gonorrhea). But there is still nothing irreparable at these stages. If we “caught” the patient at stages CIN II – CIN III, then wide excision of the affected areas is performed: excision or conization of the cervix.
A young woman with CIN I, having read horror stories on the Internet, sobs bitterly:
- Why are you crying so much? — I read that I will have cancer! I will die! - But you are already here. We would be worthless on a market day if we did not know how to identify and treat this stage. After all, this is exactly why you came to the gynecologist - so that you don’t miss CIN. We didn't miss it. Now let’s carefully remove everything and continue to observe. - Will I be able to give birth? - Necessarily. - When will it be possible to get pregnant? - You can start 6 weeks after surgery.
Wide excision of the affected areas with a loop of a radio wave apparatus is a simple procedure. We mostly do this on an outpatient basis under local anesthesia. The entire removed area is sent for histological examination.
If it's so simple, why are women still dying?
This is a cruel and valid question. Cervical cancer is always someone's fault. Although, of course, if a woman did not go to the gynecologist’s office for 10 years, only doing an ultrasound from time to time, anything could be grown.
Olga was 44 years old. I leafed through her outpatient card: gynecologist, gynecologist, gynecologist... Over the past 10 years, she gave birth to three children and had 4 abortions. There is not a single cytological smear in the card. In the mirrors - advanced cervical cancer, symptomatic treatment.
Elena, 32 years old. She gave birth to 2 children with an interval of 2 years, came for an appointment 4 months after the second birth. Cytological smears were taken twice during pregnancies, but probably very gently for fear of spotting. In the mirrors - cervical cancer, stage IIb - we will be treated.
Marina, 38 years old, cook. He undergoes regular medical examinations and shows his health certificate. In the mirrors - advanced cervical cancer, stage III, we will be treated, but the prognosis is very doubtful. I doubt she was examined in mirrors at all. Perhaps they took smears for gonorrhea and trichomoniasis without looking. The most annoying thing is that Olga was sure that everything was fine with her, since she was regularly examined.
Cervical cancer is a disease of the young. The peak incidence in our country occurs at the age of 30–35 years. The cervix is an easily accessible object for research, which makes each case of advanced cancer even worse. The disease is easily preventable by catching it at the CIN stage. And the woman will get married, and give birth to a child or three, and live a long and colorful life.
My youngest patient with invasive cervical cancer was 23 years old. A young man brought her by the hand to be examined for infection. The young man was bothered by the unpleasant smell of his beloved’s discharge. Wertheim's operation, radiation therapy, then relapse, chemotherapy. She died 2 years after diagnosis.
It is impossible not to take into account the human factor... Someone did not come to the appointment, someone did not take a cytological smear or collected the material well enough, someone did not examine single atypical cells due to pronounced inflammatory changes. There are many reasons for late diagnosis. It takes years from the introduction of HPV into the genome of epithelial cells to the onset of cancer, but invasive cancer grows and progresses very quickly.
Today, a new cervical screening strategy is being implemented everywhere in the Russian Federation - the use of liquid cytology with HPV testing. This significantly increases the chances of early diagnosis of cancer. It is this problem that gynecologists should deal with, and not “cauterizing erosions” and a merciless battle with HPV.
Let's set goals correctly. We strive to catch cancer in its pre-stages and neutralize it. “Cauterizing” everything that turns red does not help the diagnosis; on the contrary, it creates serious difficulties, masking a slowly smoldering process.
Hunting for CIN
The implementation of a simple algorithm guarantees timely diagnosis of changes in the cervix.
- Smears for oncocytology must be done for all women who are sexually active. You can do it annually, but not less than every 3–5 years. Women over 25 years of age should undergo HPV testing along with cytology.
- A “bad” cytology smear and/or detected HPV requires mandatory colposcopy. An unclear red spot on the cervix, even with “good” cytological smears and the absence of HPV, requires mandatory colposcopy.
- Abnormal colposcopy results require taking a biopsy from all suspicious areas, or, which is more correct and cheaper, performing a wide biopsy of the cervix.
After treatment for CIN, continued follow-up for at least 5 years is strongly recommended. Anything can happen—the disease can recur. If you don't lose sight of it for a couple of years, you can notice a relapse in time and prevent the development of invasive cancer.
Oksana Bogdashevskaya
Photos 1- thinkstockphotos.com, 2-5 - provided by the author
Where to get tested and treated for CIN 1, CIN 2, CIN 3 in St. Petersburg, prices
Treatment of all stages of precancer requires high-quality diagnosis and treatment using professional modern equipment. The Diana Clinic in St. Petersburg invites all women residents and guests of the city to undergo examination and treatment of dysplasia at any stage. The clinic’s gynecologists use new devices - a colposcope and a Fotek radio knife - this is the best equipment recommended by the Ministry of Health.
In our medical center you can take tests, undergo colposcopy, remove condylomas without pain and complications, cure erosion and dysplasia (laser, radio knife). We perform any gynecological low-traumatic operations, for example, conization of the cervix, excision with electric loops.
An appointment with a gynecologist costs only 1,000 rubles, an appointment based on test results costs 500 rubles. Appointment with an oncologist - 1000 rubles. Today this is practically the lowest and most reasonable price in St. Petersburg.
CIN 2 and pregnancy
Dysplasia of 1-2 degrees poses virtually no threat to the health of the pregnant woman and the fetus, but during pregnancy the disease may progress, which can affect the condition of the fetus. This is due to the fact that during pregnancy the level of immunity decreases, and the activity of atypical changes remains at the same level.
Due to a significant increase in estrogen levels, the cervix changes. The inner epithelial layer is shortened and turned outward. The progress of the disease may be affected by the acidic environment in the vagina or the penetration of the virus.
CIN 1 (mild dysplasia)
In CIN 1, pathological changes affect no more than 1/3 of the thickness of the epithelial layer from the basement membrane, which significantly complicates cytological diagnosis. Low grade dysplasia is characterized by:
- The cells are located correctly, the boundaries between them are distinct. The acini are preserved.
- Moderate proliferation (cell division), koilocytosis (cells with large nuclei) and dyskeratosis (impaired keratinization of the upper layers of the epithelium).
- Atypical cells are detected with signs of shallow structural changes in the cytoplasm and nucleus.
During initial treatment, mild dysplasia is detected in 80% of cases. CIN 1 is not dangerous, but in some cases it can progress.
In CIN I, regression of the pathological process is observed in 57% of cases, persistence in 32%, progression in 11%. Invasive cancer develops in 1% of cases within 5 years.
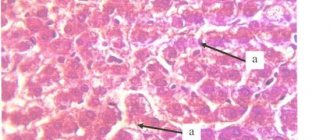
Rice. 5. Cytological examination. CIN-1 (mild dysplasia).
Pregnancy with severe dysplasia
For the formation and development of the fetus, grade 3 cervical dysplasia does not pose any particular danger. But hormonal surges during the gestational period can aggravate the pathological process, promote infection of organs, and this can already negatively affect the course of pregnancy. In addition, when passing through the birth canal during childbirth, the baby can become infected with HPV, other viruses or bacteria. In this regard, every pregnant woman with dysplasia is specially registered and carefully monitored. In this case, it is recommended to remove the neoplasia after childbirth.
Many women come to the gynecologist when they are already pregnant. Therefore, it is strongly recommended to plan your pregnancy and undergo standard diagnostics, so that if cervical neoplasia is detected, you can take professional measures and approach conception in a healthy state.
Treatment of severe dysplasia
Successful treatment of severe cervical neoplasia will allow establishing the exact cause of the disease and an individual approach that takes into account the patient’s age, concomitant diseases, and plans for further motherhood.
The purpose of treatment measures is:
- slowing down the dysplastic process;
- removal of atypical zones;
- elimination of inflammation;
- restoration of epithelial functions;
- restoration of hormonal balance;
- relapse prevention;
- prevention of malignant tissue degeneration.
Treatment of grade 3 dysplasia always begins with conservative measures, consisting of sanitation of the genital organs, the use of antibacterial agents, vitamins, immunostimulants, and dietary nutrition.
When HPV is detected, they act on the pathogen, but since there are no specific medications for papillomavirus yet, interferon preparations are used, which activate the immune defense in the form of the production of antibodies that attack the virus. Unfortunately, in many cases, interferon therapy and other conservative measures do not lead to the expected therapeutic effect. Therefore, for grade 3 cervical dysplasia, minimally invasive surgical methods are often used. The choice of technique depends on the rate of proliferation of atypia, the risk of malignancy of the process, and the presence of contraindications.
The simplest method is chemical cauterization of the mucous membrane, but in severe cases it is ineffective. The most common surgical method for eliminating cervical atypia is conization, which consists of a cone-shaped excision of the affected fragment of the cervix. The operation is performed in a day hospital under local or general anesthesia and takes up to 20-30 minutes, depending on the type of intervention. The procedure is not performed for confirmed cervical cancer, urogenital infections, pregnancy, or exacerbation of chronic diseases.
Moxibustion treatment
Conization is performed in the traditional way (using a scalpel), the loop method (electroconization), and using a laser. Laser vaporization (evaporation) is most in demand. When atypical cells are exposed to a laser beam, the affected area seems to disappear due to the evaporation of water from the tissue. During the manipulation, the doctor adjusts the power of the laser beam, which makes it possible to penetrate to different depths of the epithelium.
The advantages of laser therapy are:
- non-contact - during the operation the affected surface is not touched with instruments;
- control - the ability to control the depth of penetration of the beam;
- non-traumatic - vaporization does not affect healthy tissue due to the use of a colposcope and visualization, which virtually eliminates complications;
- minimal or no blood loss due to vascular coagulation performed during the operation;
- prevention of purulent complications - laser radiation has a detrimental effect on pathogenic microflora;
- rapid healing - laser radiation has not only a therapeutic effect on tissue, but also a stimulating effect, which activates healing and restorative processes, which leads to a short rehabilitation period;
- preservation of reproductive function - after laser vaporization there are no adhesions, scars, or narrowing of the canal. This treatment technique is preferable for patients who plan to have children in the future;
- painlessness - patients who have undergone vaporization do not feel pain or particular discomfort. There may be pain in the lower abdomen and more abundant discharge.
Conization of the cervix
Cervical dysplasia of the 3rd degree can be easily eliminated using radio wave destruction. The surgeon targets the atypical area with radio waves under the control of a colposcope. Under the influence of the wave, low-temperature steam is formed, which also performs the function of coagulation and disinfection. During the manipulation, a biopsy can be taken using a radio wave loop.
After the procedure, there are no scabs left, as after cryodestruction, against which scars could later form and infection could occur. Radio wave destruction is ideal for women planning pregnancy, since it practically does not injure the cervical mucosa and preserves the structure of the epithelium.
The procedure is carried out approximately 5-7 days of the cycle after the inflammation has been eliminated, duration – up to 20 minutes. The epithelium will be completely restored in a month and a half. In the first two weeks, sex, hot baths and other thermal procedures are not recommended, you should not do heavy physical work, lift weights, douche, or use tampons. You should definitely consult your doctor if you experience severe pain, heavy discharge (especially with an unpleasant odor), heavy bleeding, or febrile temperature. The first postoperative oncocytological smear is taken after a three-month period. Further, examinations are carried out every three months throughout the year. If the test results are negative, the patient is under clinical observation and undergoes preventive diagnostics as part of it.
Treatment should be accompanied by dietary nutrition, which must be followed after treatment procedures. The consumption of foods rich in ascorbic acid, folic acid, tocopherol, retinol, and microelements is required. It is recommended to consume more orange-colored vegetables and fruits, liver, seafood and dairy products, nuts, and vegetable oils. Alcohol, baked goods, fast foods, marinades, smoked foods, and fried foods should be excluded.
Causes
Doctors divide the causes that provoke the development of dysplasia into internal and external. The first include:
- Inflammatory processes in the reproductive organs.
- Endocrine diseases.
- Malfunctions in the immune system.
Acquired factors are considered:
- Diseases acquired through sexual contact.
- Long-term use of drugs that reduce immunity.
- Mechanical trauma to the cervix.
The most common pathogen is the 16th and 18th subtype of the papilloma virus. They are the ones who contribute 95% to the appearance of dysplasia. If there is papilloma in the body, decreased immunity, mechanical trauma or other auxiliary factors, the disease is highly likely to manifest itself.
The condition of the cervix can also worsen:
- Termination of pregnancy.
- Hormonal imbalances.
- Chronic infections.
- Frequent change of sexual partners.
- Childbirth at an early age.
Also risk factors that provoke the disease are the use of tobacco products, vitamin deficiency, genetic predisposition and use of hormonal contraceptives.
How the disease develops
HPV infection in the human body can occur transiently, latently and with a pronounced clinical picture. Its course depends on the state of the immune system. The most unfavorable is the persistent course. With the persistence of highly oncogenic HPV types, intraepithelial neoplasia (CIN) develops even with a normal cytological picture within 2 years. The most dangerous are HPV type 16. The risk of developing intraepithelial neoplasia ranges from 40 to 50%.
HPV primarily infects cells that are in the stage of active division, which are located in the basal (lowest) epithelial layer. As the cells mature, they move outward, from where they are easily removed and enter the environment, becoming a source of infection. During this time, the infection can resolve itself or proceed latently (the most dangerous condition). Dysplasia occurs without involving the surface layer and connective tissue base (stroma) in the process.
The transition from dysplasia to cancer occurs over many years. However, the slow-burning process can be resisted. It is necessary to consult a gynecologist more often and carefully follow all his recommendations.
Rice. 2. Quite a long time passes from the initial infection to the development of cervical cancer. As the symptoms of the lesion increase, more and more atypical cells (lilac color) appear in the smears. In CIN 3, malignant cells are located within the epithelial layer. In case of cervical cancer, the stroma and the superficial layer are involved in the pathological process.
Classification
There are many classifications of precancerous diseases of the cervix. The classification proposed by Richart in 1965 has become widespread, according to which cervical intraepithelial neoplasia (CIN) is divided into 3 grades - CIN 1 (mild dysplasia), CIN 2 (moderate) and CIN 3 (severe or intraepithelial cancer). CIN is changes in the epithelial layer, where normal cells are replaced by cells of varying degrees of atypia, but without changes in the stroma. The degrees of dysplasia differ in the intensity of proliferation and the severity of atypia of surface epithelial cells.
Cells containing HPV with an activated genome begin to change (structurally transform). They are called koilocytes (known as halo cells). The nucleus of such cells gradually becomes enormous in size and differs in color. Detection of koilocytes during cytological examination is a marker of possible cervical precancer. Koilocytes are detected in 10 - 15% of cases with herpes and cytomegalovirus. Koilocytes are detected using oncocytology or biopsy.
Rice. 4. In the photo on the left is CIN 1, on the right is CIN 3 (Fig. 1. c).