General information
Duodeno-gastric reflux (syn. reflux gastritis , biliary reflux , alkaline gastritis , biliary gastritis ) is a pathological process of retrograde flow of bile contents of the duodenal intestine into the stomach, which can be accompanied by clinical symptoms, histological signs and endoscopic changes of reactive (chemical) gastritis.
The term "refluxus" means "reverse flow". Under physiological conditions, bile from the duodenum should not enter the anatomically overlying parts of the digestive canal, therefore the bile reflex is considered a pathological phenomenon. DGR occurs as a result of excessive flow of bile from the duodenum due to insufficiency of the pylorus, which acts as a barrier to the retrograde flow of bile or due to a violation (reduction) of anterograde peristalsis of the stomach and duodenum. Modern scientific research indicates an increase in the number of diseases caused by the presence of pathological duodenogastric reflux in patients. At the same time, the high prevalence of GHD (in 46-52% of cases) and the frequent combination with chronic gastritis , functional dyspepsia , peptic , GERD , stomach cancer , Barrett's esophagus , sphincter of Oddi dysfunction , duodenostasis , postcholecystectomy syndrome , etc. complicates their course and therapy. GHD is quite common after surgery (in 16% of cases after cholecystectomy and in almost 55% of cases after surgery for duodenal ulcers).
In addition, duodenal reflux can cause the development of metaplasia of the esophageal epithelium, severe esophagitis and squamous cell carcinoma of the esophagus against the background of metaplasia. It should be noted that gastroduodenal reflux in its “pure” form (positioned as an isolated diagnosis) is relatively rare (10-15%) and is mainly diagnosed against the background of other diseases. That is, in most cases, GHD is a syndrome accompanying a number of diseases of the upper gastrointestinal tract.
GHD occurs due to excessive flow of bile from the duodenum due to insufficiency of the pylorus, which acts as a barrier to the retrograde flow of bile or due to a violation (reduction) of anterograde peristalsis of the stomach and duodenum.
Thus, duodenal pathological reflux complicates the course of various organic/functional diseases of the gastrointestinal tract, which necessitates its timely diagnosis, correct clinical interpretation and adequate drug correction.
Advantages of treatment of duodeno-gastric reflux at the Swiss University Hospital
- Our Center is equipped with modern equipment produced by leading European and American companies, which allows us to carry out the most complex diagnostic and therapeutic procedures with high accuracy and efficiency.
- The clinic employs specialists of the highest and first categories who have extensive experience; each of them is fluent in all techniques in their specialization.
- Our specialists have performed more than 600 surgical interventions related to duodenal obstruction.
- Patients who have concomitant diseases of the abdominal cavity and pelvis and require surgical treatment can undergo simultaneous surgery in our clinic. During one intervention, you can get rid of 3-4 pathologies (for example, kidney cysts, ovarian cysts, nephroptosis, fibroids and a number of other diseases).
Pathogenesis
The pathogenetic mechanisms of development of GDR are based on:
- failure of the sphincter apparatus, which allows the contents of the duodenal intestine to freely reach the stomach through the pyloric/lower esophageal sphincters;
- antroduodenal dysmotility (disorder of coordination between the pyloric/antral parts of the stomach and duodenal intestine), which leads to disruption of control over the direction of flow of duodenal contents;
- elimination of the antireflux barrier after surgery (partial gastrectomy ).
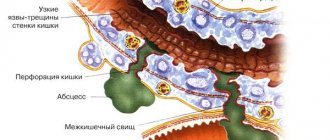
With the development of pathological GHD due to dysfunction of the sphincters, bile retrogradely, as part of the refluxate, enters from the duodenum into the higher located stomach. Components of duodenal contents, represented by bile acids, lysolecithin and trypsin , have an aggressive damaging effect on the gastric mucosa. Taurine conjugated bile acids and lysolecithin have the most pronounced effect, especially at acidic pH, which determines their synergy with hydrochloric acid in the development of gastritis . Trypsin and non-conjugated bile acids have a pronounced toxic effect at slightly alkaline and neutral pH, while the toxicity of non-conjugated bile acids is provided predominantly by ionized forms that can easily penetrate the coolant.
Long-term exposure of the coolant to bile acids contained in bile causes necrobiotic and dystrophic changes in the surface epithelium and leads to the condition of reflux gastritis (gastritis C).
In the presence of Helicobacter pylori, the damaging effect of the refluxant on the coolant is enhanced. The formation of DGR contributes to disruption of the motility of various parts of the gastrointestinal tract and the function of the sphincters, which leads to disruption of the digestive conveyor, has a negative effect on membrane/cavity digestion and absorption of food ingredients, and changes the water balance. The aggressive influence initially manifests itself in the form of increasing atrophy, dysplasia and metaplasia of the coolant, which form the risk of developing gastrocarcinogenesis. The gradual aggressive effect of bile with pancreatic juice contributes to the fact that superficial gastritis progresses and mucosal erosions transform into erosive and ulcerative lesions of the coolant.
Causes
The main reasons for the formation of DGR include:
- Congenital/acquired functional deficiency (weakening of the closing function) of the pyloric sphincter.
- Hyperkinetic type (with increased motility) of duodenal peristalsis.
- Inconsistency (discoordination) of the physiological cycles of relaxation/contraction of both the stomach and the DP-gut (migrating motor complex).
- Duodenal hypertension (increased pressure in the lumen of the duodenum), caused by splanchnoptosis (prolapse of internal organs), lumbar lordosis , hernias /malignant neoplasms.
- Long-term inflammation of the duodenum (chronic duodenitis , duodenal ulcer , gastroduodenitis ).
- Lack/absence of hormones ( gastrin ).
- Helminthic infestation (giardiasis).
- Anomalies in the development of the duodenal intestine.
Risk factors for developing duodenogastric reflux include:
- irregular food intake and poor quality nutrition (overeating, dry food, fatty and spicy foods that cause hypersecretion of bile);
- smoking and alcohol abuse;
- old age (after 60 years);
- long-term use of antispasmodics and NSAIDs;
- operations for resection of part of the stomach, cholecystectomy (removal of the gallbladder), anastomosis of the intestine and stomach;
- biliary dyskinesia , cholecystitis ;
- pancreatitis;
- diabetes mellitus , obesity .
Symptoms
Symptoms of duodeno-gastric reflux are not specific. As a rule, the disease manifests itself with a predominance of dyspeptic symptoms - nausea, heartburn, air/sour belching, bitterness in the mouth and vomiting bile. Periodically appearing pain in the upper abdomen, intensifying after eating, is cramping in nature and can be provoked by stressful situations, physical activity, or appear after surgery for gastrectomy, cholecystectomy, and with developed duodenal obstruction. Since GHD in its “pure” form is rare and is diagnosed mainly against the background of other gastrointestinal diseases, especially gastroduodenal pathology, the clinical symptoms of reflux are influenced by the symptoms of the underlying disease, which to a certain extent masks the symptoms of GHD.
conclusions
1. The results of the study showed the following: GHD leads to inflammation, foveal hyperplasia, interstitial edema, fibroproliferation and ridge arborization.
2. H. pylori
leads to an increase in inflammation, manifested in the form of an increase in the activity and severity of inflammation, foveal hyperplasia, and the number of lymphoid follicles of mild and moderate severity.
3. GHD in children may have clinical manifestations in the form of pain and a painless course. With a pain syndrome, as with a painless course, changes in the morphological picture are noted equally, therefore it is incorrect to judge the severity of morphological changes by the severity of pain.
4. DGR leads to the development of certain morphological manifestations, which does not allow it to be regarded as a physiological process.
There is no conflict of interest.
Tests and diagnostics
The diagnosis is established on the basis of clinical symptoms and instrumental research methods, among which the most effective are:
- Daily pH-metry - allows you to assess the height of reflux and the profile of intragastric pH.
- Ultrasound diagnostics (echography with water load): with GHD, the retrograde movement of gas and liquid bubbles (corresponding to the reflux of duodenal contents into the stomach) from the pylorus to the body of the stomach is periodically recorded on echograms.
- Transillumination hemomotodynamic monitoring. The difference in motor wave amplitude in the antrum of the stomach and the duodenal bulb is used as a GDR parameter.
- Fibrogastroduodenoscopy (swelling of the coolant, focal hyperemia, pyloric dehiscence).
- X-ray of the stomach (regurgitation of barium from the duodenum into the stomach is noted).
- Fiberoptic spectrophotometry.
If bile reflux is suspected, differential diagnosis is made with acid gastroesophageal reflux and peptic ulcers of the stomach.
Diet
Diet for bile in the stomach
- Efficacy: therapeutic effect after 10 days
- Timing: constantly
- Cost of products: 1400-1500 rubles. in Week
Nutrition correction is a mandatory element of complex therapy. A diet is prescribed for bile in the stomach. Dietary nutrition is aimed at normalizing the motility of the gastroduodenal organs. The main nutritional requirements for the patient are: small frequent meals, adherence to a meal regimen, exclusion from the diet of spicy and salty foods, canned food, marinades, fatty, smoked and fried foods and dishes, wholemeal bread that reduce the rate of gastric emptying. The consumption of various vegetables and legumes rich in fiber (radishes, legumes, turnips, radishes, asparagus) and fruits with rough skin (gooseberries, grapes, dates, currants), as well as coarse cereals (pearl barley, barley, millet, corn) is limited. Limit the consumption of sugar, honey and jam, chocolate. The diet should be based on low-fat boiled, easily digestible foods: light soups, porridges, chicken meat without rough crust, boiled fish and vegetables/vegetable purees, fruit/oatmeal jelly.
Patients with GHD should avoid physical activity and heavy lifting after eating, which increases intra-abdominal pressure. It is equally important to prevent flatulence / constipation . However, since GHD occurs predominantly against the background of other gastrointestinal diseases, a diet for the underlying disease may be prescribed, for example, Diet No. 5 , Diet for gastric ulcer , Diet for gastritis , Diet for gastroduodenitis , etc.
Prevention
Prevention of GHD consists of:
- Timely treatment of gastrointestinal diseases (especially gastroduodenal pathology).
- Correction of body weight.
- Maintaining the correct diet to ensure physiologically normal gastrointestinal motility.
- Quitting smoking and alcohol abuse.
- Normalization of physical activity and psycho-emotional sphere. Elimination of factors that provoke reflux (lifting weights, exercises with strong abdominal tension, avoiding being in a horizontal position after eating, working in an inclined position).
- Exclusion/avoidance of long-term use of medications that worsen bile rheology and gallbladder motility (antibiotics, expectorants, sedatives, NSAIDs, estrogens, antispasmodics, β-blockers, hypnotics, calcium channel blockers).
Drug treatment
The list of medications includes:
- antibiotics for diagnosed H. pylori infection;
- antisecretory drugs for the form with high acidity;
- antacids to relieve heartburn;
- if indicated - antispasmodic and enzyme preparations, vitamins, reparation stimulants, sedatives and herbal remedies.
Complex treatment of the disease continues for several weeks. If symptoms are severe, it is recommended to begin therapy in a hospital followed by continuation on an outpatient basis.
List of sources
- Zvyagintseva T.D., Chernobay A.I. Functional disorders of the motor-evacuation function of the digestive tract and their pathogenetic correction // News of medicine and pharmacy. – 2009.– No. 294. pp. 7–11.
- Zvyagintseva T.D., Chernobay A.I. Duodenogastric reflux in the practice of a gastroenterologist: obvious dangers and hidden threats // Medical newspaper “Health of Ukraine”. 2012.—No. 1. P.11.
- Trukhan D.I., Filimonov S.N. Differential diagnosis of the main gastroenterological syndromes and symptoms. M.: Practical Medicine, 2021. 168 p.
- Trukhan D.I. Rational pharmacotherapy in gastroenterology // Directory of a polyclinic doctor. 2012. No. 10. pp. 18–24.
- Bagnenko G.F., Nazarov E.V., Kabanov M.Yu. Methods of pharmacological correction of motor-evacuation disorders of the stomach and duodenum. // Rus. honey. magazine. Diseases of the digestive system. –2004. – T. 1. – P. 19-23.
Indications for hospitalization of patients with GERD
- esophagitis grades C, D without complications or Barrett's esophagus (hospitalization of the patient to the therapeutic, gastroenterological departments of the district health care organization (hereinafter - RHO), city health care organization (hereinafter - GOZ), regional health care organization (hereinafter - OHO));
- esophagitis with complications (bleeding, penetration, stenosis) (hospitalization of the patient to the surgical department of the ROZ, GOZ, OZ);
- GERD with a course resistant to treatment and the need to clarify the diagnosis (hospitalization of the patient to the gastroenterology department of the state health department or public health unit).