1.General information
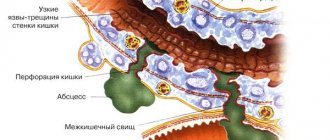
An ulcer is a long-term non-healing inflamed wound surface on the epidermal (external, skin) or mucous membrane. It should be immediately clarified that the concepts “ulcer” and “erosion”, often confused and even used as synonyms, are not the same thing. Unlike erosion or a superficial scratch, an ulcer penetrates into the deep, base layers of the corroded surface, which leads to the irreversible loss of one or another volume of tissue, and consequently to losses in its functionality. Healing of ulcers occurs by partial or complete replacement of the defect with connective tissue (“healed ulcer”).
The old Russian verb “pierce” means to make a hole, break through, pierce, pierce; The Latin word “perforate” has the same meaning, which has many derivatives both in the world of technology and in medicine.
Thus, a perforated (perforated) ulcer is an ulcer through and through, an ulcer with a violation of the tightness and the formation of a “hole”. The term “perforated ulcer” is used only in gastroenterology and implies an aggressive ulcer of the stomach or duodenum - as their walls become thinner, they can eventually break through; in every tenth case, the effusion of contents into the abdominal cavity is also accompanied by massive bleeding. In general, perforation of a gastroduodenal ulcer is one of the most dangerous and severe outcomes of peptic ulcer disease, creating an immediate threat to the patient’s life.
Considering the prevalence of ulcerative-inflammatory diseases of the gastrointestinal tract (several million people suffer from them in Russia alone), there is no need to talk for long about the severity and relevance of the problem of perforated ulcers. Today, one of the main tasks of gastroenterology remains the development not so much of diagnostic and emergency surgical protocols (see below), but of methods for accurately assessing the type of course and dynamics of peptic ulcer disease, as well as reliable prediction and reliable prevention of its perforated variants.
A must read! Help with treatment and hospitalization!
Perforated ulcer of the stomach and duodenum
Scope of diagnostic and treatment assistance at the prehospital stage:
1. The most important task of a doctor who suspects a perforation of a stomach or duodenal ulcer is to organize the promptest possible hospitalization of the patient in the surgical department.
2. Basis for the diagnosis of a perforated ulcer with a typical clinical picture:
a) acute onset; b) “dagger pain” in the stomach; c) pronounced signs of irritation of the peritoneum in the initial period due to exposure to aggressive chemical factors; d) disappearance of hepatic dullness.
3. If the patient’s condition is serious and there are signs of shock, infusion therapy is carried out, vasopressors are administered, and oxygen is inhaled.
4. It is not recommended to administer narcotic analgesics, which can obscure the clinical manifestations of the disease and disorient the hospital surgeon.
Diagnostic protocol in a surgical hospital:
1. In the emergency department, a patient with a suspected perforated ulcer should be examined by a doctor first.
2. Body thermometry is performed, the number of leukocytes in the blood and the necessary laboratory tests are determined (blood type, Rh factor, blood glucose, etc.).
3. In all cases, an ECG is recorded to exclude the abdominal form of myocardial infarction.
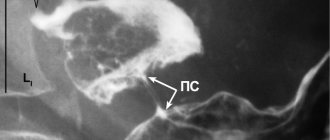
4. A plain radiography of the abdominal cavity is performed to detect free gas. If the patient's condition allows, the study is carried out in a vertical position; if not, in a later position.
5. In addition to patients with a confirmed diagnosis of a perforated gastroduodenal ulcer, patients with questionable clinical symptoms are subject to hospitalization in the surgical department.
6. In the surgical department, the diagnosis must be completed and the diagnosis of a perforated ulcer confirmed or rejected. Laparoscopy can be used for this. If it is impossible to perform it for one reason or another, it is necessary to resort to diagnostic mid-median laparotomy.
In the surgical department, the patient should be explained the seriousness of the disease, the need for immediate surgical intervention, encouraged, reassured, and obtained consent for the operation. In this case, it is often necessary to tactfully and at the same time persistently convince the patient that there is no other way out of the current situation.
Indications for surgical intervention. The diagnosis of a perforated gastroduodenal ulcer is an absolute indication for emergency surgery. This also applies to covered perforation.
Conservative treatment has to be carried out in those extremely rare cases when the patient categorically refuses surgery. Therapy according to the Taylor method is as follows. Under local anesthesia
A thick probe is inserted into the stomach with a 1% dicaine solution, through which it is emptied of its contents. After removing the thick probe, a thin gastric probe is passed transnasally and connected to a device for continuous aspiration, which is carried out over several days. The patient is placed in the Fowler position. Place an ice pack on your stomach. Correction of water and electrolyte balance, complete parenteral nutrition, detoxification therapy are carried out and massive doses of antibiotics are prescribed for 7-10 days. Before removing the probe, water-soluble contrast is injected through it and X-rays are used to ensure that it does not flow beyond the contours of the stomach or duodenum. Meanwhile, even if the perforation zone of a gastroduodenal ulcer is delimited, the likelihood of the formation of local abscesses in the abdominal cavity is very high. Therefore, this method can be recommended in the most extreme cases, since if it is ineffective, time favorable for surgical intervention will be lost, and the patient will be doomed, despite his belated consent to the operation.
Preoperative preparation. Before surgery, the patient must have a tube inserted into the stomach and its contents aspirated. The bladder is catheterized. The surgical field is hygienically prepared. In the case of a serious condition of the patient caused by diffuse purulent peritonitis, intensive therapy is prescribed and carried out together with the anesthesiologist for 1-2 hours (for more details, see Chapter III).
Anesthesia. The operation is performed under combined endotracheal anesthesia. It is possible to use epidural anesthesia after correction of hypovolemia. In exceptional cases, suturing of the perforation is carried out under local anesthesia.
Access. An upper midline laparotomy is used. In the case of a covered perforated ulcer, with an erroneous incision in the right iliac region, a large tampon is inserted into this wound to drain the abdominal cavity for the entire period of the operation and a superomedial laparotomy is performed. The median wound of the anterior abdominal wall is sutured first at the final stage of the intervention.
Features of surgical intervention. How can perforation of the stomach or duodenum be detected during intraoperative exploration of the abdominal cavity? Quite often, immediately after incision of the peritoneum, a small amount of air comes out of the wound with a characteristic hissing sound. The fluid in the abdominal cavity is usually yellow-green, cloudy, mixed with mucus, and may contain pieces of food. Exudate is evacuated by suction, crumbly food masses are removed with tampons. If the perforation is not immediately detected, the stomach should be pulled to the left, after which the pylorus and duodenum become visible to a sufficient extent. In this case, on the hyperemic anterior wall of the stomach or duodenum, it is possible to identify a whitish, infiltrated area with a diameter of 1 to 3 cm, with a round or oval hole in the middle, with clear, as if stamped, edges, most often about 5 mm in diameter.
It is much more difficult to detect perforation if the ulcer is located low, on the duodenum, or, conversely, high, on the lesser curvature or on the posterior wall of the stomach. It is not easy to navigate when the surgeon encounters pronounced perigastritis, periduodenitis and extensive adhesions. In such cases, identifying the location of the perforation is facilitated by the methodical nature and sequence of the examination.
First, you need to carefully palpate areas that are difficult to examine, moving along the lesser curvature from the cardia to the descending branch of the duodenum. You should palpate not only the lesser curvature of the stomach, but also both of its walls, trying to enclose them between the thumb and index finger. The ulcer area is defined as a dense, rigid infiltration of the gastrointestinal wall.
Secondly, after the surgeon has found the infiltrate, but has not seen the perforation, you should grab this area with your fingers and try to carefully squeeze out the contents of the stomach or duodenum. In this case, only one drop of content may be released. Having detected inflammatory changes and crepitus in the retroperitoneal space, it is necessary to mobilize the duodenum according to Kocher in order to examine its posterior wall.
Third, when searching for the site of perforation, one should take into account the direction from which the effusion is coming. So, if it comes from the omental (Winslov) foramen, the perforation should be looked for on the posterior wall of the stomach, access to which opens after a wide dissection of the gastrocolic ligament. Every operating surgeon should not forget that
You may encounter cases where two ulcers perforate at the same time: on the anterior and posterior walls of the stomach. In the later stages after perforation, massive deposits of fibrin and accumulations of purulent exudate are found in a variety of places. In such cases, all parts of the abdominal cavity should be systematically examined and sanitized. To do this, the exudate is evacuated by suction, fibrin deposits are removed if possible (with tweezers and a wet swab), and its various parts are repeatedly washed with antiseptic solutions. Without fail, these manipulations must be performed in the subhepatic, right and left subphrenic spaces, lateral canals, and pelvic cavity. After evacuation of pus and initial washing of these areas, it is advisable to insert tampons into them for the period of intervention aimed at eliminating the main pathological process. After its completion, it is necessary to complete the sanitation of the abdominal cavity. The tampons introduced at the first stage of the operation are removed and all affected parts are re-treated. Leaving pus and fibrin films can lead to the formation of abscesses or the persistence and progression of peritonitis. If the surgeon, due to the “neglectedness” of the process, cannot fully sanitize the abdominal cavity during the primary surgical intervention, he should plan to perform a repeat sanitization operation (programmed relaparotomy after 24-48 hours).
After detecting a perforation, the surgeon must decide: whether to perform a gastric resection, suturing the perforation, or excising the ulcer followed by pyloroplasty and vagotomy?
Choosing a method of operation. The type and amount of benefits are determined strictly individually depending on the type of ulcer, the time elapsed since perforation, the severity of peritonitis, the patient’s age, the nature and severity of concomitant pathology, and the technical capabilities of the operating team. There are palliative operations (suturing of a perforated ulcer) and radical (resection of the stomach, excision of an ulcer with vagotomy, etc.). When choosing a method of surgical intervention, it should be borne in mind that the main goal of the operation is to save the patient’s life. Therefore, most patients are indicated for suturing of a perforated ulcer. This operation can be performed by any surgeon; in extreme cases, it can be performed under local anesthesia.
Suturing a perforated ulcer is indicated in the presence of diffuse peritonitis (usually when the perforation is more than 6 hours old), a high degree of surgical risk (severe concomitant diseases, old age), in young patients with a “fresh” ulcer without visual signs of a chronic process and an ulcer history, in the case of perforation of stress symptomatic ulcers.
“Youthful” ulcers after their suturing and antiulcer drug treatment tend to heal and have a disease-free course in 90% of cases. When determining the scope of surgery for perforated gastric ulcers, it should be borne in mind that they, especially in elderly patients, may be malignant. Therefore, whenever possible, gastric resection is advisable. If this is not possible, a biopsy must be taken.
The perforation in the stomach wall is “closed” with two rows of interrupted seromuscular sutures. Each of them is applied in a longitudinal direction to the axis of the stomach (intestines). In this case, a number of sutures are located in the transverse direction, which avoids narrowing of the lumen of the organ.
Perforated ulcers of the pyloroduodenal zone are preferably sutured with a single-row synthetic suture without capturing the mucosa, in the transverse direction, so as not to cause a narrowing of the lumen. If the walls of the ulcer in the circumference of the perforated hole are motionless, loose and applied sutures begin to cut through when tied, they can be reinforced by suturing a strand of the omentum or gastrocolic ligament on the leg.
Sometimes, when cutting sutures, it is necessary to use Polikarpov’s method, who suggested not tightening the edges of the ulcer with sutures, but freely plugging the perforated hole with a strand of omentum on the stem. Using a long thread, this strand is passed into the lumen of the stomach through a perforated hole, and then fixed with the same thread passed through the wall of the stomach back to the serous surface. When tying the ends of the thread, the gland seals the hole tightly. After this, around the ulcer and slightly away from it, the omentum is additionally fixed from the outside with separate sutures.
Retroperitoneal perforations are identified by the presence of air and bile impregnation in the paraduodenal tissue. To suture such an ulcer, preliminary mobilization of the duodenum according to Kocher is necessary. After suturing the perforated ulcer, the tissue is drained from the lumbotomy approach.
If, when an ulcer is perforated, a weakened patient also has pyloric stenosis, suturing the perforated hole must be supplemented with posterior gastroenteroanastomosis. As the experience of surgeons has shown, in this case it is also necessary to perform a vagotomy (from this it is clear that such an intervention cannot be considered optimal; in such situations it is better to perform excision of the ulcer with pyloroplasty (see below).
The final stage of surgery for a perforated ulcer of the stomach or duodenum should be a thorough toilet of the abdominal cavity. The more thoroughly the remnants of gastroduodenal contents and exudate were removed, the easier the postoperative period proceeds and the less opportunity there is for the formation of abscesses in the abdominal cavity.
If at the time of the operation there was a large amount of contents in the abdominal cavity, then, despite careful toileting, it is advisable to drain the abdominal cavity.
Endovideosurgical intervention. With appropriate equipment and qualifications of doctors, laparoscopic suturing of a perforated ulcer is possible. Detection of diffuse peritonitis, inflammatory infiltrate or signs of intra-abdominal abscess is an indication for switching to laparotomy.
The duodenal stump is sutured with a purse-string suture. An anastomosis is performed between the gastric stump and a loop of jejunum, passed behind the transverse colon through a “window” into the mesocolon.
Gastric resection is indicated in cases of chronic, callous gastric ulcers (especially if their malignancy is suspected), as well as in cases of decompensated pyloroduodenal stenosis. This operation is possible under the following conditions: 1) the absence of diffuse fibrinous-purulent peritonitis, which develops 6-12 hours after perforation; 2) the patient’s age is less than 60-65 years and the absence of severe concomitant diseases; 3) sufficient qualifications of the surgeon and the availability of conditions to perform this technically complex operation.
Resection is carried out, as a rule, according to the Billroth II method, as modified by Hoffmeister-Finsterer, and in particularly favorable conditions - according to the Billroth I method. For low duodenal ulcers, technical difficulties in processing the duodenal stump, it is advisable to perform an anastomosis according to Roux. Unimpeded evacuation of the contents of the duodenum avoids the insolvency of its stump. The technique of gastric resection is described in detail in special manuals and monographs. Here I just want to mention that it is preferable to apply a gastroenteroanastomosis with a single-row serous-muscular intranodular suture (Fig. 9.5), for good comparison and tissue regeneration. This avoids the development of anastomositis.
Excision of a perforated ulcer with pyloroplasty and vagotomy. Indicated for perforated ulcer of the anterior wall of the duodenal bulb without significant inflammatory infiltrate. The operation is performed under the same conditions as gastrectomy.
The operation is as follows. Two holders are placed on the edges of the duodenal ulcer so that they can stretch the intestine in the transverse direction. The ulcer is excised within healthy tissues along with the pylorus, in the form of a diamond, the length of which is directed along the axis of the stomach and duodenum. By pulling the holders, the defect in the duodenum is sutured in the transverse direction with a one- or two-layer suture, thus performing pyloroplasty according to Heineke-Mikulich. When perforation is combined with stenosis of the gastric outlet, the most adequate drainage will be provided by Finney pyloroplasty.
After sanitation of the abdominal cavity, vagotomy is performed. In conditions of emergency surgery, preference should be given to the most technically simple method - truncal vagotomy.
When perforation and bleeding are combined, a more reliable remedy is excision of the bleeding ulcer (or gastrectomy).
Pyloroantrumectomy with truncal vagotomy. Indicated for patients with duodenostasis (sharply dilated and atonic duodenum) or in the case of a combined form of peptic ulcer, when perforation of the duodenal ulcer and chronic gastric ulcer are detected.
Selective proximal vagotomy with suturing of a perforated ulcer is performed in young and middle-aged patients in the absence of peritonitis and gross cicatricial deformation of the pylorus and duodenum. This operation has limited use in emergency surgery.
Completing the operation. Carry out thorough sanitation and, if necessary, drainage of the abdominal cavity. In some situations, it is rational to install two tubes: one for nutrition (it is inserted into the jejunum), the other into the stomach for decompression.
Postoperative period. The experience of many surgeons convincingly shows the benefits of active management of patients after surgery. It includes rapid activation of the patient, breathing and therapeutic exercises and early, nutritious nutrition, which prevents the development of complications and accelerates regeneration processes.
Of the postoperative complications, bronchopneumonia is in first place in terms of frequency of occurrence, purulent complications are in second place, and disturbances in the evacuation of food from the stomach are in third place.
Subdiaphragmatic, subhepatic, interintestinal and Douglas pouch abscesses are complications often associated with insufficiently thorough toileting of the abdominal cavity during surgery. The clinical picture and diagnosis of these abscesses have been described in detail previously. We only emphasize that it is necessary to pay attention to the appearance of abdominal pain, persistent paresis of the gastrointestinal tract and control the nature of the temperature curve, pulse rate, and changes in the leukocyte formula.
Peritonitis that occurs in the postoperative period is usually associated with failure of the sutures after suturing the perforation or resection of the stomach and requires urgent reoperation. It should be noted that although the failure of the sutures is accompanied by repeated release of gas into the free abdominal cavity, its detection during X-ray examination at this stage loses its significance, since after laparotomy air is detected in the abdominal cavity for more than 10 days.
A more valuable diagnostic technique is to give the patient 1-2 sips of water-soluble contrast. If it extends beyond the gastrointestinal tract, it indicates failure of the sutures at the site of suturing a gastroduodenal ulcer or gastroenteroanastomosis.
It is impossible to ascertain the failure of the sutures of the duodenal stump in this way, since during resection using the Hoffmeister-Finsterer method, the contrast agent from the stomach does not enter the duodenal stump. In such cases, the presence of incompetence of the sutures of the duodenal stump will be indicated by a sharp pain syndrome, peritonitis and an increase in the amount of free gas when re-examined after 40-60 minutes.
Impaired gastric emptying in the postoperative period is manifested by regurgitation and vomiting. It may be due to the functional state of the gastrointestinal tract or be of a mechanical nature. For diagnostic and therapeutic purposes, in these cases, the introduction of a thin probe into the stomach and evacuation of its contents is indicated. At the same time, an active fight against postoperative intestinal paresis should be waged. The patient should be on parenteral nutrition and receive sufficient fluids, proteins and electrolytes.
If, after 5-7 days of conservative treatment, despite the elimination of intestinal paresis, the symptoms of stagnation in the stomach do not decrease, it is necessary to perform a gastroscopy to exclude a mechanical obstruction and decide on a repeat operation.
Mechanical reasons may be the following: 1) when suturing an ulcer: a) narrowing of the pyloric area - as a defect in the surgical technique, b) pronounced perigastritis and periduodenitis; 2) during resection of the stomach: a) narrowing of the anastomosis due to swelling of the walls and subsequent scarring, b) narrowing of the anastomosis due to inflammation and scarring of the mesentery of the transverse colon, c) flow of contents into the afferent loop with compression of the efferent loop, d) improper fixation of the gastric stump in the window mesentery of the transverse colon.
Outcomes. The main causes of mortality in perforated gastroduodenal ulcers are peritonitis, postoperative pneumonia and severe concomitant diseases. An unfavorable outcome is most often a consequence of the patient’s late seeking of medical help and untimely diagnosis. In recent years, in most medical institutions, mortality during surgical treatment of perforated ulcers of the stomach and duodenum has decreased and amounts to 5-7%. Long-term results depend not only on the type of operation, but also on the correctness of the chosen surgical tactics.
2. Reasons
With peptic ulcers of the stomach and/or duodenum, a certain seasonal dependence is most often observed, and most perforations occur in spring/autumn. It is also known that cases of perforated ulcers increase significantly during periods of socio-economic upheaval and military operations. In general, insufficient and unhealthy nutrition, especially in combination with chronic stress, is one of the main triggers of ulcerative perforation. There is no direct and clear dependence on age; patients include children and very elderly people, but statistically the age range of 25-50 years is considered to be the most risky.
The main risk factors include anything that sharply and quickly (or simultaneously) increases the pressure inside the stomach: blunt abdominal trauma, overeating, physical activity, drinking alcohol (especially fizzy drinks).
Visit our Gastroenterology page
Preparing for surgery
The patient must undergo endoscopic diagnostics as prescribed by the doctor, as well as standard preoperative preparation, which includes:
- clinical and biochemical blood tests;
- blood tests for HIV, syphilis, hepatitis B and C;
- coagulogram;
- general urine analysis;
- fluorography;
- ECG.
With the results of the examination, you need to visit a therapist, who, in the absence of contraindications, signs permission for the operation. After this, you need to consult with an anesthesiologist and surgeon.
3. Symptoms and diagnosis
In the clinic of a perforated ulcer, there are three stages, the names of which speak for themselves:
- abdominal shock;
- imaginary well-being;
- purulent diffuse peritonitis.
Each of these phases takes, on average, about six hours.
The most characteristic symptom of the initial stage is a sharp and very intense pain, often radiating to neighboring areas or the back. It is this type of pain syndrome that the well-known expression “dagger pain” refers to, and it, like a real sudden stab in the stomach, is accompanied by a powerful psycho-emotional shock. In most cases, the patient takes a forced fetal or other similar position, tries not to move (or rather, cannot), breathes shallowly and often, his eyes “sink,” his face acquires an earthy-pale hue and a characteristic motionless, suffering-panic expression. Bradycardia and a decrease in blood pressure, caused by a reflex reaction to damage to intra-abdominal tissues and receptors by the gushing acid of the gastric juice, are also quite typical.
Subsequently, the color of the facial skin, breathing, heart rate and blood pressure are somewhat normalized. At this stage, as a rule, precious time is lost: often the patient has to literally beg consent for a life-saving operation. Subjective improvement is not without reason called “imaginary well-being” - in fact, this is already a fatal risk, since in the next phase (repeated vomiting, dehydration, sharp worsening of the general condition, tachycardia and tachypnea, significant bloating) to provide assistance, even the most urgent and qualified, in many cases it is already too late.
An experienced doctor confidently assumes the diagnosis even with an external examination, palpation and percussion: there are a number of fairly informative criteria regarding muscle status, zones and nature of pain, etc.
However, much depends on the specific location of the perforation and the dynamics of symptoms. In some cases, the situation develops according to an atypical scenario; in particular, the clinical picture may resemble symptoms of acute appendicitis, myocardial infarction, pulmonary pathology - in other words, differentiation and clarification are required. In addition to the physical examination, laboratory tests, an X-ray examination (usually with a contrast agent, the detection of which outside the stomach and duodenum is one hundred percent proof of perforation), and urgent fibrogastroduodenoscopy are prescribed. In some diagnostically difficult cases, laparoscopic examination is used.
About our clinic Chistye Prudy metro station Medintercom page!
Rehabilitation after surgery
Rehabilitation should include three main aspects:
- early patient activation;
- therapeutic and breathing exercises;
- special diet.
All this prevents complications and accelerates tissue restoration processes.
On the first day after surgery, passive and active movements of the legs are allowed. From the very first day you need to do breathing exercises. If there are no contraindications, you can get out of bed already on the 2-3rd day.
If recovery goes well, the stitches will be removed on the 8th day. Usually after 2 weeks the patient is already discharged from the hospital if there are no complications and rehabilitation is going well.
4.Treatment
Perforation of an ulcer is an absolute and unambiguous indication for emergency surgery. The techniques used (suturing, resection, etc.), antiseptic measures, postoperative treatment and rehabilitation strategies may be different, since the characteristics of a perforated ulcer vary widely and, in addition, the scale and stage of the process at the time of intervention is of key importance.
An important task is the prevention of complications - pneumonia, purulent inflammation, peristalsis disorders, etc.
It remains to add that even the constant skill of the domestic school of emergency surgery (and only the surgeons themselves truly know that in order to save a patient’s life in the operating room, only the surgeons themselves truly know), a perforated ulcer is characterized by a significant mortality rate (today this is 6-8%). The prognosis depends critically on the timeliness of seeking help and its provision, on the accuracy of diagnosis and the choice of the optimal surgical plan.
Main indications for surgery:
- ineffectiveness of drug treatment, that is, non-healing of the ulcer, two times a year or more - relapses of ulcerations, early relapses after taking medications;
- severe ulcerative pain that limits the ability to work and does not go away despite drug therapy;
- complicated ulcer – bleeding, perforation, narrowing of the pylorus.
Indications for gastrectomy:
- multiple ulcers, of which one is perforated and the other is bleeding;
- extensive callous gastric ulcers;
- simultaneously a stomach and duodenal ulcer.
Diet after surgery for peptic ulcer
In the postoperative period, you need to follow a very strict diet. If the operation was not severe and without complications, then from the second day you can drink water - 0.5 cups per day with teaspoons. From the third day you can drink 0.5 liters, in addition to water, strong tea and broth are added. From the fourth day you can drink 4 glasses a day, which must be divided into 8-12 doses. As food you can eat jelly, raw eggs, yogurt, slimy soups, sour cream.
From the fifth day, depending on the patient’s condition, you can consume liquid food in unlimited quantities. Grinded soups, cottage cheese, semolina porridge are allowed. From the seventh day you can include well-ground boiled meat in your diet. From approximately the 9th day, the patient switches to diet No. 1a, that is, the anti-ulcer table, with the exception of dishes that are prepared with whole milk. Meals should be fractional - 7 times a day in very small portions.
Contraindications for surgery
Absolute contraindications:
- hemorrhagic shock;
- heart diseases with severe circulatory failure;
- purulent peritonitis;
- numerous operations on the abdominal organs;
- lung diseases with respiratory failure;
- blood clotting disorder.
Relative contraindications:
- local diffuse peritonitis;
- diaphragm hernia;
- severe obesity;
- advanced gastrointestinal cancer;
- contraindications to general anesthesia.
Prevention of recurrence of the disease
First of all, you need to exclude factors that cause peptic ulcer:
- alcohol consumption;
- stress;
- smoking;
- heavy physical activity;
- improper diet, eating fried, spicy foods, smoked foods, fast food;
- non-compliance with diet.
To prevent ulcers you need:
- sleep at least 6-8 hours a day;
- minimize the consumption of foods that irritate the gastric mucosa - fatty, smoked, fried;
- chew food well;
- eat up to 6 times a day;
- eat chopped food, cereals, jelly, omelettes, vegetables, steamed meat;
- See a doctor immediately if you have stomach pain;
- eliminate alcohol and smoking;
- protect yourself from stress;
- reduce coffee consumption to a minimum;
- eat boiled, baked, steamed food with a minimum of spices.
You need to visit a doctor for preventive examinations once a year. Also, for prevention, all patients are prescribed courses of antiulcer medications in the summer and spring.