December 14, 2021 Overactive bladder (hyperreflex, OAB or OAB) is a form of neurogenic bladder (NUB) in which a person has problems with voluntary conscious control of urination. This form of NMP is more common than the hyporeflex form. The main symptom is frequent urination, which may be accompanied by an increase in urine volume. OAB is a serious problem, as its prevalence is comparable to hypertension, chronic bronchitis, asthma and heart disease.
Main causes of the disease
There are two main types of GMF:
- With increased detrusor tone (with neurological pathology);
- Ideopathic detrusor instability (various causes).
However, there is no doubt that other health problems or medications you are taking can also cause symptoms of hyperactivity. To find out the exact cause of the disease, you should make an appointment with a specialist who, with the help of examinations and tests, can prescribe appropriate treatment.
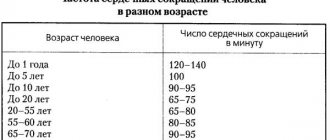
In a normal bladder condition, a person should urinate no more than eight times. In this case, the daily amount of fluid released is about two liters. But in the case of the development of various pathologies, these parameters can change. In the case of an overactive organ, trips to the toilet become more frequent, but the volume of discharge does not change. But the size of each portion becomes different. As a rule, the impetus for the development of OAB is given by increased conductivity of impulses in those muscles that are located around it. As a result, even slight irritation of the organ’s receptors provokes muscle contraction and the desire to empty the bladder. This condition occurs as a result of neurogenic or non-neurogenic factors. The first include:
- Pathologies of the brain of the head or back, the list includes multiple sclerosis, Alzheimer's and Parkinson's diseases, various neoplasms and encephalitis. The cause of an overactive bladder can be alcoholic, diabetic neuropathy.
- Injuries and damage to the spinal cord and brain - these can be compression ruptures, results of surgery and stroke.
- Birth defects affecting the spinal cord.
- Congenital pathologies of the bladder.
Non-neurogenic factors include age, diseases developing in the genitourinary area, anatomical features and sensory disorders, in which changes in hormonal levels and the sensitivity of bladder receptors are observed against the background of atrophy of the mucous layer. Those who suffer from depression, fibromyalgia, irritable bowel syndrome and attention disorders are often prone to developing an overactive organ. The development of the pathological condition is accompanied by a number of unpleasant phenomena; the symptoms of OAB and treatment are closely related:
- Sleep may become worse.
- Quite often, infectious processes begin to develop in the urinary tract.
- Pollakiuria – increased frequency of urination – may be observed.
- Nocturia, in which urination occurs at night.
- The urge to urinate becomes urgent, in other words, urgent. This urge can last for several seconds or minutes.
- Optional but possible symptoms include urge urinary incontinence.
Important. The main problem is that these symptoms can occur in a patient regardless of the time of day or place. Accordingly, there is a noticeable deterioration in his quality of life.
Diagnostics: how it goes, what procedures are performed
Diagnosis of overactive bladder syndrome begins with informing the doctor about the patient’s complaints and medical history. One of the key elements of diagnosis is the analysis of the number of urinations during the day and at night. Monitoring is carried out using the patient's diary, in which it is necessary to enter data on urination for three days.
A diagnosis of pathology in the bladder is made if the patient urinates more than 8 times a day, with uncontrollable urges occurring at least twice a day. The doctor also prescribes laboratory tests, which include the following studies to determine the causes of the pathological condition:
- bacteriological tests to detect the presence of infection in the genitourinary system;
- cystoscopy and urethroscopy;
- Ultrasound, which examines the kidneys, bladder, and prostate gland.
Through these procedures, during an outpatient examination, the doctor identifies various pathologies of the genitourinary system that arise along with the symptoms that characterize an overactive bladder. In order to fully confirm the diagnosis and prescribe appropriate treatment, a urodynamic analysis with fullness cystometry is performed. That is, the Doctor records an increase in detrusor pressure during urgency when the bladder is full.
It is also necessary to inform the specialist about the medications you are taking, since some of them may worsen the symptoms of incontinence.
It is necessary to come for diagnostics with a slightly full bladder, since this way a more detailed ultrasound examination can be carried out, on the basis of which effective treatment will be prescribed. It is also recommended that you first fill out a urination diary for three days, which will allow the doctor to get a complete picture of the patient’s medical history. The following data must be entered into the diary: volume of urine, muscle tension during urination, degree of leakage and intolerance of urge, volume of fluid drunk.
Causes of OAB in women
Overactive bladder is often more common in women than in men. This is due both to objective physiological reasons and to health problems, which are also typical for men. Some of the problems that cause hyperactivity are:
- Weak pelvic muscles. A woman's pelvic floor muscles support her uterus and bladder. The stress of pregnancy and childbirth sometimes stretches them and makes them weak. In addition, the anatomy of the vagina changes (prolapse appears), a cystocele develops;
- Diuretic drugs. They are also called diuretics and are often prescribed for high blood pressure. They help the body get rid of salt and water, so the bladder quickly fills and incontinence may even occur;
- Aging and menopause. Your bladder changes after menopause. Doctors aren't sure whether this is due to a lack of estrogen, which has receptors in the bladder, or simply due to the natural aging process. Most likely, each of the factors plays a role;
Treatment: modern techniques
Several treatment approaches have been developed. The chosen technique depends on how severe the symptoms are and the stage of the disease.
For mild symptoms, exercises can be used as prevention and treatment to train the bladder muscles so that the patient can control urge and urination. The main goal of such exercises is to go to the toilet less often due to the fact that the muscles will be able to hold an increased amount of urine. The training includes two stages: going to the toilet if necessary in the morning and practicing urinary control throughout the day.
At the first stage of treatment, the patient learns to control urges and tries to visit the toilet at increased intervals. So, if previously the patient went to the toilet every half hour, the time gradually increases to 45 minutes or an hour. If you have a strong and uncontrollable urge to urinate when your bladder is empty, you can perform Kegel exercises by contracting your muscles. It is necessary to gradually increase the intervals between urinations. The norm is to visit the toilet 4-5 times during the day and once at night.
OAB in men
Overactive bladder, according to various sources, occurs in 15-16 percent of men, and symptoms of the disease more often appear with age.
One of the most common causes of OAB symptoms in men is an enlarged prostate. The prostate may simply increase in size as you age, or it may be a sign of a serious disease, such as prostate cancer. If the prostate becomes large enough, it interferes with the flow of urine from the urethra. In addition, hyperactivity occurs due to a number of other factors:
- Urinary tract infections;
- Prostate and bladder stones;
- Uncontrolled diabetes;
- Poor nutrition and sedentary lifestyle;
- Taking certain types of medications (caffeine, diuretics;)
- Neurological conditions such as Parkinson's disease, etc.
Symptoms of OAB can affect every aspect of a person's life. People usually perceive this problem as personal, so they often do not seek medical help until the last minute. The doctors at our clinic understand the sensitivity of this problem and will provide the most comfortable treatment possible. Fortunately, there are several effective treatments available.
Which doctor should I contact?
For treatment of a disease such as overactive bladder, it is necessary to contact a urologist who can conduct qualified diagnostics and establish a competent diagnosis, taking into account the causes and symptoms of the disease that the patient has. It is wrong to contact a gynecologist with this disease, since this specialist can only indirectly treat the pathology, but will not be able to prescribe competent treatment.
It is often necessary to initially visit a therapist, who will refer you to a specialist who treats a specific problem. Patients can undergo examination at the JSC Meditsina clinic in Moscow, where qualified specialists work to help cope with problems of varying severity. On the clinic’s website, visitors can get acquainted with the doctors who see them, their certificates and specialization.
OAB in children
The problem of OAB is not related to the age category, and children quite often outgrow this condition upon reaching seven years of age. If we are talking about incontinence or excessively frequent urinary processes in a child under three years old, this phenomenon should be treated as completely normal and not a problem.
Let's consider what factors can provoke an overactive bladder in children:
- Development of infectious processes in the urinary tract.
- Presence of neurological diseases.
- Development of acute or chronic constipation.
- The occurrence of stressful situations, especially if they are associated with the urination process.
- Inability to go to the toilet for a long time.
- Overactive bladder syndrome occurs when the capacity of the organ is not large enough.
- Presence of foods containing caffeine in the diet. This applies to chocolate, sweet carbonated waters and tea.
- Structural changes affecting the organs of the urinary system.
An allergic reaction to certain foods and irritation of the organ lining can have a negative impact. According to foreign statistics, after a child turns five years old, cases of OAB in this age category decrease, this figure reaches about 15%. As children grow older, they acquire the ability to respond in a timely manner to signals sent by the body indicating the need to go to the toilet.
Symptoms
The main symptoms of the disease include the following conditions:
- an urgent urge to go to the toilet that a person cannot control. This symptom of the disease manifests itself as an urgent and suddenly appearing need to visit the toilet without preliminary urges, that is, the desire increases instantly, and not gradually. During the day, the frequency of such urges can reach 8 times or more. Conditions are also possible when various sounds, such as the babbling of liquid, provoke urges and uncontrolled urination;
- frequent urination, even if the bladder is almost empty;
- imperative incontinence, that is, uncontrollable leakage of urine that the patient is unable to contain;
- a feeling of incomplete emptying of the bladder, even after urinating completely. Moreover, the total volume of urine per day does not exceed the norm for an adult, approximately 1.5-2 liters;
- nocturia, that is, frequent night trips to the toilet (two or more). This sign is an alarm bell if observed every night, and can cause more serious pathologies.
Are you experiencing symptoms of an overactive bladder?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Diagnosis and treatment
The first step in any treatment method is diagnosis by a qualified physician. He will conduct a short survey about the person's urinary tract and any medical interventions or procedures he has had. A physical examination will then be performed. Typically, these examinations include:
- General urological (examination, tests, ultrasound);
- Special methods (X-ray, urethrocystoscopy, urodynamic diagnostics);
The doctor will also likely take a urine sample for testing. In addition, a cough test will likely be performed. All of these methods are designed to determine the exact cause of the disease and prescribe the correct treatment for overactive bladder.
However, before diagnosing OAB, the doctor must exclude the possibility of other diseases accompanied by similar symptoms. The list of such pathologies includes bladder neoplasms, infection of the urinary system, urolithiasis, diabetes, interstitial cystitis and impaired functionality of the pelvic muscles. The mandatory stages of the examination include:
- Conducting a general analysis of urine, including sediment microscopy.
- Measuring the volume of residual urine, especially in the presence of neurological pathologies or in cases where the patient has undergone surgery to eliminate incontinence.
- For three days, you are required to keep a diary of urination, which takes into account the volume of fluid drunk and excreted, and the number of visits to the toilet.
- If there are traces of blood in the urine, suspicion of neoplasms in the bladder, or the presence of foreign bodies, cystoscopy is recommended.
- In case of neurogenic urinary disorders, a complex of urodynamic studies is necessary, since they make it possible to assess both the functionality of the lower tracts of the system and the risk of negative effects on the kidneys with the selection of the most effective therapy.
- If OAB is diagnosed in a female patient, a consultation with a gynecologist and examination on a chair is required, which makes it possible to identify prolapse of the pelvic organs and atrophic changes.
As for the treatment of overactive bladder, it consists of successive stages from simple to more complex. But drug therapy remains the main way to eliminate OAB, regardless of the form of the pathology. Drugs for overactive bladder prescribed by specialists include M-anticholinergics, tricyclic antidepressants and myotropic antispasmodics. Typically, medication courses are carried out in parallel with behavioral therapy and neuromodulation. With tibial neurostimulation, the tibial nerve is treated using a thin needle electrode, the procedure is carried out in an outpatient clinic once a week, the course lasts three months. Then a maintenance course is required at intervals of 30 days throughout the year.
If there is no positive result from drug therapy, they proceed to tests using cold water and Lidocaine, which makes it possible to identify the form of OAB. Then they determine how to treat overactive bladder in women and men. The effectiveness of the use of botulinum toxin has also been proven, which serves as a blocker of acetylcholine release and promotes relaxation of smooth muscles located in the walls of the organ. As a result, urgency incontinence disappears, the frequency of urination and the urge to urinate decrease. The duration of the positive effect of such injections, in which the drug is injected into certain areas of the bladder, lasts from 6 to 9 months, then it may be necessary to repeat the course of treatment for overactive bladder in men and women. How to treat overactive bladder with surgery? Surgical intervention becomes necessary extremely rarely, and the bladder is replaced with a piece of the large or small intestine. It is also possible to perform a myectomy, when the volume of the bladder is increased.
Our clinic provides diagnostics by qualified doctors at an affordable cost, as well as the prescription of effective treatment for men and women, which will help to forget about the unpleasant problem forever.
| Code | Name | Price |
| 03.00 | Initial appointment with a urologist (candidate of medical sciences) | 2,000 rub. |
| 03.04 | Repeated appointment with a urologist (candidate of medical sciences) | 1,200 rub. |
| 03.60 | Initial appointment with a urologist (MD) | 5,000 rub. |
| 03.61 | Repeated appointment with a urologist (MD) | 3,000 rub. |
| All prices of the men's and women's health clinic | ||
Overactive bladder. Drug therapy
Lecture transcript
XXV All-Russian Educational Internet Session for doctors
Total duration: 24:23
00:00
Oksana Mikhailovna Drapkina, Secretary of the Interdepartmental Scientific Council on Therapy of the Russian Academy of Medical Sciences, Doctor of Medical Sciences, Professor:
— We're moving on to the next section. From hepatology we move to urology. Professor Shkolnikov Maxim Evgenievich: “Overactive bladder. Drug therapy."
Maxim Evgenievich Shkolnikov, professor:
— Good afternoon, dear colleagues! Today we return once again to the common topic of overactive bladder.
You can see on this slide: according to epidemiological studies, overactive bladder occurs in 10% to 15% of the world's population. With age, its frequency increases.
The problem of overactive bladder itself arises and disrupts the function of the lower urinary tract, namely the urine storage phase. All the symptoms that occur in this situation occur when urine accumulates in the bladder. It is very important that at this point low pressure is maintained in the bladder so that it can accumulate a sufficient amount of urine. When this does not happen, this condition may occur.
According to modern terminology, the leading symptom of an overactive bladder is urgency. It consists of a feeling of a sudden, irresistible urge to urinate, which is difficult to restrain. Often this symptom is also accompanied by frequent urination, as well as urinary incontinence.
It is believed that the basis of an overactive bladder is detrusor overactivity. This, in turn, is already a urodynamic concept. It consists of involuntary contraction of the detrusor during the urine storage phase.
The main mechanism of contraction of detrusor smooth muscles is associated with the presence of muscarinic receptors, the activation of which leads to contraction of smooth myocytes. The main contractile function is performed by M3 receptors, which lead to contraction, but M2 receptors also play a certain role. They block the relaxation mechanism of smooth myocytes activated by β3 adrenergic receptors.
02:39
Today they talk about the involvement of other structures of the bladder wall, which can also lead to the occurrence of certain symptoms of an overactive bladder.
Urothelium. You can see on this slide: it contains a huge number of different receptors that respond to chemical and physical stimuli. It can also release a number of neurotransmitters (acetylcholine, nitric oxide, ATP), which influences and modulates the activity of detrusor smooth muscle cells and can also lead to activation of peripheral nerve fibers. They, in turn, can lead to the emergence of that very symptom of urgency.
In addition, a certain role is assigned to interstitial cells located in the suburothelial space. They have certain electrical properties and contain a number of receptors, the activation of which can lead to the generation of an electrical signal, its amplification and transmission to sensory fibers, which is perceived by the central nervous system as a desire to urinate.
This slide summarizes a huge number of medications. These are data from the International Consultation on Urinary Continence. They are based on the principles of evidence-based medicine. You see, the only drugs that are clearly proven to be effective for bladder symptoms are the (single class) antimuscarinics.
There are also drugs such as Oxybutynin and Propiverine, which have mixed effects. Their antimuscarinic effect is combined with a direct antispasmodic effect.
Another drug with I A level of evidence. This is Desmopressin, which is a vasopressin analogue.
All other groups of drugs, namely β-blockers, β-adrenergic agonists, NSAIDs, have not yet acquired a sufficient evidence base for us to clearly and confidently recommend them for the treatment of patients with symptoms of overactive bladder.
05:17
So, today we can purchase the following antimuscarinic drugs in Russian pharmacies.
Oxybutynin. Surely all specialists who deal with the problem of overactive bladder know the drug. It has been on the market since approximately the 1960s. A very old drug. Used as a means of comparison for new developments. But, looking ahead, I will say that this is the most toxic of all drugs existing on the market today.
Trospium chloride. It is also a fairly old drug, but has proven itself to be highly effective. Looking ahead, I will say that it has quite a few unusual, unique features that make it possible to distinguish it from the entire group of antimuscarinics.
Tolterodine. Today, it exists on the Russian market exclusively in generic form.
Solifenacin. New drug (relatively new). He also performed well. We are awaiting new data regarding the effectiveness of this drug in different patients.
Despite the fact that M3 receptors are the main ones in the mechanism of bladder contraction, they are in the minority compared to M2 receptors in the detrusor wall. This is approximately 2:3. There is evidence that conditions such as diabetes mellitus, neurological diseases, infrarenal obstruction, and age-related changes cause M2 receptors to increase even more than M3 receptors.
What is the ideal antimuscarinic drug? Firstly, it must have maximum tropism for the M2 and M3 receptors. It should have maximum uroselectivity, that is, it should exert its effect exclusively on the lower urinary tract, because everyone knows: muscarinic receptors are also located in other smooth muscle organs, as well as the salivary glands and the brain. Exposure to them can cause a number of practically unacceptable side effects.
The drug should not affect other medications, so as not to change their pharmacokinetics and pharmacodynamics.
Finally, the drug must be easy to use. Ideally, once a day, so that, as they say, drink and forget.
08:35
Among the drugs on the market regarding their tropism to muscarinic receptors, you see that trospium chloride (or spasmex) has the maximum tropism to all types of muscarinic receptors.
If we talk directly about M3 and M2 receptors, then all drugs can be divided into three main groups. These are equivalent drugs: with the same tropism for M2 and M3. Relatively selective M3 drugs. Superselective M3 drugs.
Trospium chloride and tolterodine are relatively equivalent drugs. You see that equivalent tropism is when their ratio is one. For trospium chloride it is 1.3, for tolterodine it is 3.2.
Solifenacin and oxybutynin are relatively selective drugs.
Finally, darifenacin, which is not yet on the market (in the research phase), belongs to the superselective M3 receptors.
To date, debate has not subsided about whether M3 selectivity is an advantage or, on the contrary, a disadvantage, because, unfortunately, direct comparative studies do not yet exist.
The next point by which antimuscarinic drugs can be compared. Their chemical structure. You see that most of them, and one might say almost all of them with the exception of trospium chloride, are amine derivatives and have three nitrogen bonds. This is in contrast to trospium chloride, which has four bonds and a charged nitrogen atom.
Such physicochemical properties of the drug allow trospium chloride, unlike other drugs, to practically not penetrate into the central nervous system. Moreover, there is evidence that there is a special glycoprotein in barrier cells. This is a molecule that actively removes trospium chloride from the central nervous system.
10:58.
Take a look. This slide shows: the physicochemical properties of trospium chloride lead to the fact that it has extremely high hydrophilicity and low lipophilicity. Accordingly, it does not penetrate the blood-brain barrier.
If the drug does not cross the blood-brain barrier, it has a significantly better side effect profile. Especially related to the effect on the central nervous system. This is especially important in children, as well as in elderly patients who have a number of concomitant diseases that affect brain function. For example, encephalopathy, strokes. Such patients can take a large number of other drugs that already affect the central nervous system.
Low penetration through the blood-brain barrier is a definite advantage of trospium chloride compared to other agents.
How else can the available antimuscarinics be compared?
You can see in this table that trospium chloride, unlike oxybutynin, tolterodine, and solifenacin, is practically not metabolized in the liver. It does not have metabolites with anticholinergic effects, which are usually associated with most side effects. Due to this, it naturally does not affect the pharmacokinetics of other drugs that patients can take in parallel with antimuscarinics.
Another interesting point. Trospium chloride, unlike other drugs, is excreted in almost unchanged form by the kidneys in the urine. This allows it to have a certain local effect, which is very important.
It is believed that acetylcholine is not only released from nerve fibers, but it is also released from the urothelium in response to its stretch. It activates muscarinic receptors located in urothelial cells. They release adenosine-3 phosphoric acid. It activates adrenergic receptors on sensory fibers and causes a feeling of urgency.
Being in the urine, trospium chloride is able to block muscarinic receptors of the urothelium, thus disrupting one of the components, one of the links in the pathogenesis of overactive bladder (compared to other drugs that do not penetrate into the urine, but act exclusively in the blood serum).
14:00
The high effectiveness of these drugs is known. On average, antimuscarinics are thought to relieve symptoms in 77% of patients. I will not repeat or provide comparative tables. I will only show data from 2009 and 2010. This is data from a study of trospium chloride, which clearly shows how the use of the drug changes the structure of urgency.
If at the beginning of treatment moderate and strong urgency predominates, then as a result of using the drug, patients report either mild urgency or it disappears altogether.
This slide presents data from our department. We used the drug in patients with various types of overactive bladder. This is idiopathic active bladder and its combination with benign prostatic hyperplasia.
Also, you know, there is an overactive bladder without detrusor overactivity. This is a very complex category of patients with an unclear mechanism of symptoms. Also in patients with neurogenic detrusor hyperactivity as a result of spinal diseases and Parkinson's disease.
The drug showed itself well in the form of a decrease in the number of urinations per day, an increase in the volume of urination, which was confirmed by urodynamic data in the form of an increase in cystometric capacity.
However, I repeat that the results were significant in all groups, with the exception of overactive bladder without detrusor overactivity. This is apparently due to the fact that the symptoms are not associated with muscarinic mechanisms, but with some other mechanisms: purinergic or adrenergic.
What is very important?
The effect of trospium chloride, according to our data, can persist for quite a long time. This slide shows that over the course of 2 years, those patients who remained under our observation (17 patients out of 47) maintained a good effect in the form of a decrease in the number of urinations and urgency. It was not only not inferior to the initial data obtained after three months, but even surpassed it in a number of cases.
16:45
Another interesting data. Today, trospium chloride is available in pharmacies in doses of 5 and 15 mg. In Europe it still exists in a dose of 30 mg. Finally, starting this summer it will be sold in our pharmacies. Patients will be able to purchase trospium at a dose of 30 mg per tablet.
If you look at these charts, they reflect a survey study of over 3,000 doctors. These are general practitioners, urologists and gynecologists (unfortunately, gynecologists did not fit on this slide). You see that most general practitioners prefer an initial dose of 30 mg per day, while urologists are more adventurous in their choice and use (a quarter of urologists use) a dose of 45 mg per day.
What is good about the drug? The drug is very easy to titrate. Its dose can be either reduced or increased depending on the desired effect and the severity of side effects. If general practitioners used the maximum dosage of mainly 60 mg per day, then urologists absolutely painlessly increase this dosage to 90 mg per day.
There are scientific studies that confirm the complete safety of the drug at such a high dosage.
Typically, general practitioners prefer to prescribe the drug once or twice a day, while specialists prescribe it two or three times a day.
At the bottom of the slide, please note, there is very interesting data. If the drug trospium chloride is prescribed in a single dosage of 45 mg, then its concentration level is almost the same as that of long-acting tolteradine. This suggests that the drug does not need any new form that would allow it to be released slowly to reduce side effects and eliminate the drug from having peak concentrations and fluctuations.
Despite the presence of a certain choice and abundance of drugs, in my opinion, I consider the drug trospium chloride to be the most optimal from the point of view of treating patients with overactive bladder due to its certain properties.
No penetration through the blood-brain barrier, no central side effects, no metabolism in the liver and cross-reaction with other drugs, local action on the urothelium, the possibility of flexible selection of the optimal dosage from 15 to 90 mg per day.
The drug begins to act fairly quickly - from 3 to 7 days. If there is no effect after a week, there is no need to wait and force the patient to suffer with the existing symptoms. You can select other means.
Finally, the pharmacokinetics of the drug allows it to be used not only three times a day, as recommended, but it can be used 1 and 2 times a day, which does not affect its fluctuations in serum concentration and allows achieving a good clinical effect.
Thank you.
20:45
Oksana Drapkina: Thank you very much. Have questions.
Maxim Shkolnikov: So, a question.
What are the first symptoms of an overactive bladder in women? What diseases should be used for differential diagnosis?
Very good question. I would not divide the questions into first and second. There is a single main symptom - urgency (the occurrence of a sudden strong urge that a person cannot tolerate).
Of course, this symptom can also occur with other obvious urological diseases: bladder stone, cystitis, prostate adenoma. When you have ruled out all of these obvious urological conditions and found no cause that could explain the presence of these symptoms, this is the patient who can be diagnosed with overactive bladder.
Second question.
How long do patients with an overactive bladder have to take antimuscarinic drugs?
This is also a relevant question, since we are forced to say that drugs work as long as you take them. Once patients stop taking antimuscarinics, unfortunately, symptoms tend to return.
International recommendations recommend extending the course of treatment for about three months. The patient can then stop taking it and evaluate their symptoms. If symptoms don't return, great. We helped, we cured. If symptoms return, unfortunately, patients are forced to take these drugs again.
22:29
Oksana Drapkina: You also have a very interesting question. Can I read it so people can hear?
Maxim Shkolnikov: Of course.
Oksana Drapkina: Are the concepts of “overactive bladder syndrome” and “irritable bowel syndrome” essentially equivalent?
Maxim Shkolnikov: Also a good question. I believe that these conditions are truly equivalent: in both cases, patients are forced to visit the toilet frequently. In one case, to urinate. In another case - to empty the rectum. Already from this point of view they are equivalent.
But even if we consider the pathogenetic mechanisms, then, in my opinion, everything is similar here, too, because an overactive bladder can also be called an irritable bladder, despite the fact that we do not have any visible obvious reasons that could lead to this condition. The same as with IBS.
Valentin Fadeev: In veterinary practice, due to a certain structure, let’s say, combined in a number of animals (birds, in my opinion), this would be something uniform pathogenetically.
Oksana Drapkina: Interesting idea!
Valentin Fadeev: Use in animals? For dogs, to go for walks with them less often!
Oksana Drapkina: Maxim Evgenievich, everything you are telling us about today. You see how useful it is for us to communicate! All of Russia is watching us now. I think the different topics we are discussing today raise different questions. Before this I had irritable bowel syndrome. Now I have overactive bladder syndrome. These questions arise on their own. This is the power of internal diseases!
Contraindications for illness
When treating the syndrome it is necessary:
- stop eating citrus fruits, pineapples, chocolate, sweets, spicy and sour foods, dairy products, since these products cause irritation to the mucous membrane of the genitourinary system;
- avoid excessive consumption of water and any liquid in general; excessive reduction of the daily water intake is also contraindicated;
- Minimize the consumption of alcohol and energy drinks.
By following these recommendations, you can cope with hyperactivity syndrome, reduce pain to a minimum and increase the effectiveness of drug treatment.
Clinical observation No. 5
A 28-year-old patient complained of difficulty urinating, periodically arising in response to a full bladder, headaches, flushing of the skin of the face and neck, profuse sweating, accompanied by a rise in blood pressure up to 180/100 mmHg. Art.
From the anamnesis it is known that in January 2015 the man received a spinal cord injury at the level of the C4–C5 vertebrae with a spinal cord contusion. He was operated on and underwent spinal fusion of C4–C6. Since February 2015, the patient’s condition allowed him to begin active rehabilitation. Since April 2015, there has been a significant improvement in his condition; he was able to stand without support. In the first 2 months. After surgical treatment, the patient had cystostomy drainage. Then the feeling of the urge to urinate returned to him, and involuntary urination in small portions, of an urgent nature, was restored. The cystostomy fistula was healed and the patient began using a condom. Since May 2021, the condition has worsened and the above symptoms have appeared. During a neurological examination, the level of damage to the nervous system was determined as motor from the level of the C4 segment, sensory - from the C5 segment, reflexes 4+ in all tests on all extremities. Clonus from the hands is greater than from the feet. Muscle tone was assessed as spasticity of 2 points on the Ashforth scale in the legs, 3 points in the arms. ASIA Score: C. Can rise from a chair with minimal support. It takes time to initiate walking. Can sit without support. Walking is spastic. Signs of severe autonomic dysreflexia to cold and bladder overflow.
The urine analysis showed no signs of inflammation or bacterial contamination. According to ultrasonography, there are no structural changes in the urinary tract. The average volume of residual urine is 200 ml. During neurourological examination: bright bulbocavernous and anal reflexes. Urination in small portions is frequent and urgent, initiated by irritation of the skin of the anterior abdominal wall in the area of the bladder. Episodes of headaches with skin hyperemia and high blood pressure (up to 180/100 mm Hg with a base blood pressure of 110/70 mm Hg) occur 1–2 times a day. These symptoms are regarded as autonomic dysreflexia, the main characteristic of which is a rise in blood pressure by 20 mmHg. Art. from the baseline value in response to triggers, in this case the trigger was bladder overflow. According to a urodynamic study, the patient has phase detrusor hyperactivity with a maximum detrusor pressure of 79 cmH2O. Art. The maximum pressure at the leak point was 69 cmH2O. Art.
In order to relieve neurogenic detrusor overactivity, the patient was prescribed fesoterodine (Toviaz®) on an ongoing basis at a dosage of 8 mg/day, with transfer to periodic catheterization of the bladder. At a follow-up examination a month later, the patient's episodes of autonomic dysreflexia associated with bladder overflow disappeared. He noted a significant improvement in his quality of life. Control urodynamic study after 3 months. showed a significant reduction in maximum detrusor pressure and detrusor pressure at the leak point.
This clinical example showed the possibility of m-anticholinergic in relieving neurogenic detrusor hyperactivity and autonomic dysreflexia. Autonomic dysreflexia occurs at a high level of spinal cord injury, above the Th6 segment [13]. It has extremely negative consequences for the patient’s quality of life and significantly worsens his comorbid background. Today, research is underway on the use of fesoterodine to relieve autonomic dysreflexia and alleviate suffering in the most difficult patients - disabled people with spinal cord injury [14].
What are the features of the treatment of mixed urinary incontinence?
Firstly, in this case, additional diagnostics are needed to confirm (or exclude) the mixed form. The basis of additional examination is a comprehensive urodynamic study (CUDI)
, which allows you to find out which of the two types of incontinence is more pronounced. Depending on the results of KUDI, treatment will begin with the form of incontinence that is more pronounced. Only if the patient’s stress form predominates, then the first stage is implantation of a suburethral sling. And after the operation, treatment for OAB begins.
Pathogenesis
Most authors associate the pathogenesis of the disease with ischemic changes in the detrusor that occur due to atherosclerosis or bladder outlet obstruction. When the blood circulation in the detrusor is impaired, postsynaptic denervation occurs and subsequent structural changes occur in the intercellular junction of myocytes. The above-described structural changes are one of the main reasons for the formation of detrusor hyperactivity, which is manifested by frequent and urgent urination.
A long-term and detailed study of the structure of the mucous membrane of the bladder led to the conclusion that even minor changes and formations affect the regulatory function of the bladder.
Advantages of treatment at the clinic of JSC "Medicine"
Treatment in the hospital of the clinic of JSC "Medicine" takes place in comfortable conditions - patients are provided with rooms with all amenities.
The competitive advantage that the clinic has is cooperation with insurance companies. The modern clinic provides medical services at the highest professional level, providing effective treatment for patients even with complex forms of the disease.
Treatment and diagnostics are carried out by qualified specialists of our clinic using modern equipment, using effective medications, in order to completely relieve patients from pain and discomfort.