Indeed, certain types of ovarian cysts regenerate on their own, but no one can give an absolute guarantee to such a process, since it is unknown how the pathology will behave under the influence of certain factors.
But a functional cyst is quite capable of negatively influencing the function of reproductive and even nearby organs and causing serious complications at a certain stage of development. Therefore, contacting a gynecologist and at least dynamic monitoring of the tumor is mandatory for patients with any type of pathology.
Classification of cysts of the female reproductive system is carried out regarding their location and contents. There are several types of ovarian cysts.
Causes
The etiology of a functional ovarian cyst is not precisely known. It is believed that the main role in this mechanism belongs to hormonal changes that can occur against the background of:
- pathologies of the endocrine glands;
- taking hormone-containing and certain other medications;
- inflammation of the genitourinary and other body systems;
- pituitary diseases;
- frequent abortions;
- absence of pregnancy during childbearing age;
- premenopause and menopause.
The risk of developing a functional ovarian cyst is higher in women of reproductive age, but older women are often diagnosed with functional formations.
Treatment at the Yusupov Hospital
Specialists at the Yusupov Hospital provide patients with high-quality medical services that meet international standards. Treatment of ovarian cysts in women at the Yusupov multidisciplinary hospital is carried out with the participation of oncologists who regularly improve their qualifications and improve their existing skills.
During the appointment, oncologists at the Yusupov Hospital tell the patient who has been diagnosed with an ovarian cyst what types there are and what treatment is most appropriate. When developing a treatment plan, specialists choose the most gentle methods that are highly effective.
Modern medications in combination with minimally invasive techniques used at the Yusupov Hospital help preserve women’s reproductive health. If you have been diagnosed with a serous ovarian cyst or other types, make an appointment with an oncologist by calling the Yusupov Hospital.
Symptoms
Functional ovarian cysts are usually small in size up to 1.5 cm, rarely the formation reaches 5 cm or more. At the beginning of its formation and at first the functional neoplasms do not manifest themselves in any way, so the woman is not aware of the condition of her affected ovary. Sometimes unexpressed manifestations are possible as long as there are no complications.
A gynecologist may suspect a functional ovarian cyst based on the following signs:
- feeling of heaviness in the lower abdomen;
- nagging pain;
- cyclical disorders;
- metrorrhagia not associated with menstruation.
Symptoms become more intense with physical overload, during and after sex. This may cause nausea, weakness, soreness and breast enlargement. If a functional ovarian cyst has reached a large size, then the woman’s abdomen enlarges.
Contact us for qualified help
Do not self-medicate. At the first symptoms of the disease, consult a doctor.
Types of ovarian cysts
Depending on the location, left-sided, right-sided and bilateral ovarian cysts are distinguished. Neoplasms can be single-chamber or multi-chamber. Cysts up to 2.5 cm in size are considered small, more than 5 cm - large.
A retention cyst is a formation that looks like a tumor. Formed as a result of fluid accumulation. There are the following types:
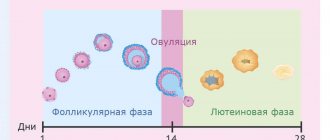
- Follicular. The most common type of retention cyst. The most common cause of its development is hormonal imbalance.
- Luteal (corpus luteum cyst). The corpus luteum is an endocrine gland that produces progesterone. In this way, the body prepares for pregnancy.
- Endometrioid. The cyst cavity is filled with menstrual blood. Occurs against the background of endometriosis.
- Thecalyuteinic. Among the reasons for its formation are excess hCG during hydatidiform mole and the presence of choriocarcinoma. Thecal lutein cysts are most often bilateral.
- Paraovarian. Originates from the tissues of the epididymis. Localized between the ovary and fallopian tube. Paraovarian cysts are most often single-chamber.
Follicular and luteal cysts are considered functional. They are formed as a result of a violation of the release of the egg from the follicle. These types of cysts are prone to self-resorption. This process takes about 1-3 menstrual cycles. However, functional cysts do not always go away on their own. Supervision by an experienced physician is required throughout the entire period.
When hemorrhage occurs, the functional cyst fills with blood or blood clots. During this period, the risk of tumor rupture increases.
In addition to cysts, doctors identify true benign tumors - cystomas. Unlike cysts, these formations have the ability to transform into cancerous tumors. Tissue growth also occurs in them. The following types of cysts are distinguished:
- Cystadenoma. Formed from epidermal tissue. Depending on the nature of the contents, it can be serous, mucinous, serous-papillary.
- Dermoid cyst. It is a teratoid tumor. It is a capsule containing various tissues. Occurs due to a violation of embryonic development. Dermoid cysts are characterized by slow growth. The danger of this type of formation lies in the fact that until a certain point it cannot be determined during a gynecological examination or even an ultrasound examination. According to statistics, dermoid cysts are usually detected in adolescence. This is due to hormonal changes in the body.
Diagnostics
Most often, a woman learns about the presence of a functional ovarian cyst when visiting a gynecologist for a routine examination or for another reason. To confirm the diagnosis, the doctor prescribes transvaginal ultrasonography. Since cystic formations occur only on one side, ultrasound diagnostics determines a functional cyst of only the left ovary or only the right. To exclude inflammation, blood and a smear are taken from the patient for examination. A pregnancy test is required. To exclude a cancerous tumor, testing for a tumor marker (CA-125) is done.
Complicated functional ovarian cysts require more detailed diagnosis:
- diagnostic laparoscopy will reveal torsion of the cystic pedicle, rupture of the capsule and at the same time eliminate these complications, as well as remove the formation itself;
- puncture of the posterior vaginal fornix is performed if there is a suspicion of the presence of abdominal fluid or blood in the peritoneum;
- CT, MRI, and radiography are necessary to differentiate a functional cyst from other neoplasms.
After laparoscopic diagnosis, a fragment of biomaterial is sent for morphological examination.
What is an ovarian cyst?
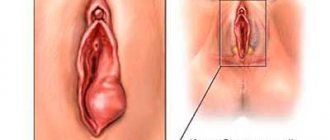
As a rule, the term “ovarian cyst” refers to a formation in the ovary that has a capsule and contents.
The fluid in the cyst can be very varied: very watery, or dense, viscous. Tumors of various origins and structures develop in the ovaries; in this regard, the ovaries occupy one of the first places among other human organs.
Figure 1. Diagram of an ovarian cyst
Treatment methods for functional cysts
As a rule, a thin-walled functional ovarian cyst of a small size (up to 1 cm) without signs of malignancy resolves on its own within two to three months. In this case, treatment is not required; a wait-and-see approach is used, in which the pathology is monitored using ultrasound diagnostics. For inflammation and other health problems, a woman is treated conservatively. Hormonal (COC) and anti-inflammatory drugs are prescribed. The treatment is carried out under ultrasound control, its goal is to prevent growth and complications or reduce the size of the formation.
If the pathological formation does not disappear within three or more menstrual cycles, the patient complains of pain, then the doctor decides on surgical treatment. Surgical treatment aims not only to remove the functional cyst, but also to preserve the integrity of the ovary, as well as reproductive health.
Surgical treatment is carried out using minimally invasive technologies:
- puncture with aspiration;
- laparoscopy of ovarian cyst.
A functional ovarian cyst is punctured with a special needle, which is inserted using a puncture attachment on a transvaginal ultrasound probe. The liquid is aspirated (pumped out) and sent for cytological examination. Instead, ethyl alcohol (10-15 ml) is injected, which has a sclerosing effect. With this treatment, the best results are observed in patients of reproductive age.
Laparoscopy of cyst
Surgical treatment is indicated for ineffective conservative treatment, complicated course of the disease, and space-occupying formations on the ovaries. After mandatory diagnostics confirming the diagnosis, the patient undergoes preoperative preparation before surgical treatment. You need to do an FLG, an ECG, take a vaginal smear for microflora, blood and urine tests, and consult an anesthesiologist.
The laparoscopic technique is most suitable for cystectomy. The patient receives anesthesia. The gynecologist surgeon makes several small holes on the abdominal wall for inserting endoscopic instruments and a miniature camera through them, with the help of which the doctor controls the entire surgical process. Carbon dioxide is supplied to the abdominal cavity to improve visibility of the surgical field. The doctor cuts the capsule of the tumor, removes it with micro-instruments; if it is voluminous, then first the contents are aspirated, part of which is sent for laboratory testing. The incisions are sutured, leaving almost invisible marks in their place.
The operation lasts no more than 50 minutes, the woman is transferred to the ward, after 2-3 days she can go home if the outcome of the intervention is successful.
Ovarian cancer treatment
Treatment of patients with ovarian cancer has traditionally included initial staging, followed by aggressive cytoreductive surgery in combination with intraperitoneal cisplatin. In early stages (1 and 2), total hysterectomy and bilateral salpingo-oophorectomy are used (or unilateral if a woman of childbearing age wishes to preserve her fertility, although this approach is controversial).
For patients with advanced tumors (stages 3 and 4), cytoreductive intervention is recommended, which involves partial removal of the tumor lesions; This operation is aimed not only at improving the quality of life of patients, but also at reducing the likelihood of intestinal obstruction and eliminating the metabolic effects of the tumor. Optimal cytoreductive intervention involves the removal of all tumor implants larger than 2 cm; with suboptimal, the transverse size of the remaining tumor nodes exceeds 2 cm. Successful cytoreductive surgery increases the effectiveness of chemotherapy and leads to increased survival.
Patients with stage 1a or 1b ovarian tumors may require only elective surgery without subsequent chemotherapy, while more advanced stages require postoperative chemotherapy with cisplatin (the most effective drug for ovarian cancer). Despite the fact that the positive response to platinum therapy reaches 60-80%, about 80-90% of women with the third stage of the disease and about 97% with the fourth stage die within 5 years.
In patients receiving treatment for ovarian cancer, the most effective method of monitoring is measurement of serum CA-125 levels and physical examination. Repeat laparotomy remains the most accurate method for assessing the effectiveness of chemotherapy, but it produces many false-negative results and does not lead to an increase in survival. CT is used to look for a macroscopic lesion and avoids repeat biopsy. If residual tumor tissue is detected using diagnostic methods, the patient may be prescribed additional treatment; however, radiation methods show a large number of false negative results.
Doctor's opinion
In advanced cases, with severe complications, oophorectomy is performed according to indications, when the ovary is removed along with the formation, although this is rare in the functional type.
Rehabilitation after laparoscopy takes only 2–3 weeks. All this time, the patient is observed by the attending physician, control ultrasound diagnostics, anti-inflammatory and symptomatic therapy are carried out. The patient must follow medical recommendations, avoid physical activity and exercise, do not take a hot bath, refuse other thermal procedures, avoid sex for a while, and adhere to the recommended diet. Control ultrasonography should be performed 2 months after surgical treatment. — Butunov Alexey Andreevich Obstetrician-gynecologist, laparoscopist surgeon, oncologist. Doctor of the highest category.
Malignant cystic ovarian tumors
Radiation diagnostic methods, such as ultrasound or MRI, are not intended to determine the histological type of tumor. However, with their help it is possible to differentiate benign and malignant neoplasms with varying degrees of certainty and determine further tactics for patient management. Detection of radiation signs of malignant tumor growth should direct the attending physician (gynecologist, oncologist) to further actively determine the nature of the cyst (surgery with biopsy, laparoscopy). In unclear and contradictory cases, it is useful to re-interpret the MRI of the pelvis, as a result of which you can get a second independent opinion from an experienced radiologist.
Get an MRI of the ovaries in St. Petersburg
Complications
Functional cysts account for 90% of all ovarian tumor formations, of which 80% are follicular. Most of them undergo reverse development, but some reach significant sizes, which leads to overstretching of the cystic membrane, increasing the risk of such complications:
- leg torsion;
- capsule rupture;
- leakage of contents into the peritoneum, which can cause peritonitis;
- hemorrhage;
- menstrual irregularities.
The most dangerous is torsion of the leg, which can lead to rupture of the membrane, leakage of fluid and hemorrhage into the peritoneum.
This causes severe symptoms: febrile temperature up to 40 degrees, dyspeptic disorders, severe pain in the abdomen, tension in the anterior abdominal wall. This condition requires urgent professional help and is subject to further long-term treatment.
Leg torsion is the most dangerous complication
Inflammation of the appendages (salpingoophoritis) and tubo-ovarian abscess
Tubo-ovarian abscess usually occurs as a complication of an ascending (from the vagina to the cervix and fallopian tubes) chlamydial or gonorrheal infection. CT and MRI reveal a complex cystic formation of the ovary with a thick wall and lack of vascularization. Thickening of the endometrium or hydrosalpinx makes the diagnosis of tubo-ovarian abscess more likely.
An axial contrast-enhanced CT scan reveals a complex cystic formation on the left, resembling an abscess, with a thick wall accumulating contrast and gas inclusions inside.
On a CT scan in the sagittal plane (left), it can be seen that the ovarian vein approaches the mass, confirming its nature (arrow). On the coronal tomogram (right), the anatomical relationships of the mass and the uterus can be assessed. A gas bubble is visualized in the uterine cavity, which suggests an infectious onset here, with subsequent spread of infection through the fallopian tube to the ovary.
Prevention
There are no specific preventive measures to prevent the formation of a functional ovarian cyst. The main task of women facing this disease is to increase immunity, regularly visit a gynecologist for preventive purposes, lead a healthy lifestyle, and get rid of bad habits.
Other useful tips:
- control body weight;
- have a protected sex life;
- try to eliminate the stress factor;
- limit heavy physical activity;
- promptly treat inflammatory and infectious diseases of the genitourinary system.