Pharmacodynamics
Antifungal agent. A triazole derivative exhibits an antifungal effect by blocking the biosynthesis of ergosterol in the cell membrane of fungi. The “target” for the action of the drug is the enzyme 14-α-demethylase.
14-α-demethylase is part of a group of enzymes known collectively as cytochrome P450. All enzymes of the cytochrome P450 group contain hematinic iron-containing pigment. Fluconazole binds to the iron atom of the hematin group and inactivates 14-α-demethylase, which leads to disruption of ergosterol synthesis and accumulation of lanosterol and other sterols. Their inclusion in the membrane instead of ergosterol significantly disrupts the structure and function of the fungal cell membrane.
A decrease in ergosterol synthesis, as well as the accumulation of 14α-methylsterols, destroys the tightly packed acyl chains of fungal membrane phospholipids. Destabilization of the fungal membrane leads to dysfunction of membrane enzymes, including those involved in the electron transport chain, and ultimately to cell death.
Used for systemic mycoses: candidiasis, cryptococcosis, blastomycosis, histoplasmosis, coccidioidomycosis, as well as dermatomycosis. The relatively low toxic profile and high penetration into the cerebrospinal fluid make fluconazole the drug of choice for systemic candidiasis and cryptococcal meningitis. Because of complications associated with intrathecal amphotericin B, fluconazole is the first-line drug for coccidioidal meningitis. Although fluconazole is active against the causative agents of blastomycosis, histoplasmosis, and sporotrichosis, it is inferior in effectiveness against the causative agents of these infections to itraconazole. Fluconazole is not effective against aspergillosis.
Pharmacokinetics
After oral administration, fluconazole is well absorbed; food intake does not affect the rate of absorption of fluconazole, its bioavailability is 90%.
The time of maximum concentration after oral administration, on an empty stomach, 150 mg of the drug is 0.5-1.5 hours and is 90% of the plasma concentration when administered intravenously at a dose of 2.5-3.5 mg/l. The half-life of fluconazole is 30 hours. Communication with plasma proteins is 11-12%. Plasma concentration is directly dependent on dose. 90% level of equilibrium concentration is achieved by 4-5 days of treatment with the drug (when taken 1 time / day).
Administration of a “loading” dose (on the first day), 2 times higher than the usual daily dose, allows one to achieve a concentration level corresponding to 90% of the equilibrium concentration by the second day.
Fluconazole penetrates well into all biological fluids of the body. The concentration of the active substance in breast milk, joint fluid, saliva, sputum and peritoneal fluid is similar to that in blood plasma. Constant values in vaginal secretions are achieved 8 hours after oral administration and are maintained at this level for at least 24 hours.
The pharmacokinetics of fluconazole depends significantly on the functional state of the kidneys, and there is an inverse relationship between the half-life and creatinine clearance. After hemodialysis for 3 hours, the concentration of fluconazole in plasma decreases by 50%.
Indications for use
Indications for the use of Fluconazole capsules are:
- Cryptococcal infection, including specific damage to the membranes of the brain (cryptococcal meningitis) in patients with immunodeficiency or with a normal state of functional immune activity.
- A severe form of candidiasis with generalization of the infectious process and damage to a significant amount of tissue (mucous membranes of various organs, skin, peritoneum, endocardium, eyes, respiratory and urinary tracts). In most cases, the infection develops against the background of a pronounced decrease in the functional activity of the immune system during malignant neoplasms, treatment with cytostatics, immunosuppressants, as well as in patients who have been in the intensive care unit for a long time.
- Localized candidiasis, developing on the mucous membranes of the oral cavity and upper digestive tract, on the structures of the urogenital tract - the drug in dosage form for systemic use is used in case of insufficient effectiveness of ointment or cream for topical use.
- Dermatomycosis, which is localized on the skin of the feet, torso, and groin area.
- Pityriasis (multi-colored) lichen.
- Fungal infection of the nail plates (onychomycosis).
- Deep endemic mycoses, which may include paracoccidioidomycosis, coccidioidomycosis, histoplasmosis in patients with normal functional immune activity.
The drug is also used to prevent the development of fungal infections in patients with normal or impaired immunity.
Features of the chronic form of candidiasis
The causative agent of vaginal candidiasis is a fungus of the genus Candida, which belongs to the opportunistic microflora. The microorganism lives on the skin and mucous membranes of almost every person, and its growth and activity are suppressed by the immune system. Any malfunction of the immune system disrupts the balance of microflora and leads to the activation of pathogenic bacteria and fungi. In this situation, acute candidiasis develops, characterized by severe, vivid symptoms and requiring immediate treatment under the supervision of a physician. If you self-medicate or let the disease take its course, it becomes chronic, which is much more difficult to combat.
Chronic recurrent candidiasis is characterized by periodic exacerbations, which are repeated 4 or more times during the year. A fungal disease occurs in 2–3% of women of reproductive age. If relapses occur no more than 4–5 times a year, it means that the infection develops passively, does not cause serious complications and is more effectively amenable to drug therapy. But when the symptoms of thrush bother you every month, it is better not to hesitate to visit a doctor, because such a course of a chronic disease indicates the progression of severe inflammatory processes in the organs of the genitourinary system.
Directions for use and dosage
Fluconazole capsules are intended for oral administration. They should not be chewed and should be taken with sufficient liquid. The dosage and regimen of use of the drug depend on medical indications:
- Cryptococcal meningitis in adults and children over 15 years of age - on the first day the drug is prescribed at a dosage of 400 mg per day, then switched to a maintenance dose of 200 mg per day.
- Prevention of exacerbation of cryptococcal meningitis in patients with severe immunodeficiency, in particular against the background of AIDS - after completion of the course of primary therapy aimed at maximizing the destruction of the causative agent of the disease, the drug is prescribed in a daily dosage of 200 mg.
- Generalized candidiasis - in the first days, 400 mg per day is prescribed, then switch to 200 mg per day. If there is no sufficient therapeutic effect, switch again to a dose of 400 mg.
- Candidiasis localized on the mucous membrane of the oral cavity and esophagus - 150 mg once a day for 14 to 28 days (depending on the speed of achieving a therapeutic result).
- Vaginal candidiasis in women (thrush) - 150 mg once, to prevent exacerbation, the drug is repeated after 1 month. Sometimes, if there is insufficient effectiveness and a chronic course of this form of candidiasis, the doctor sets the dosage and regimen of use, including the duration of the course of therapy, individually.
- Prevention of candidiasis of various localizations - the dosage is set by the doctor individually, it can vary from 50 to 400 mg per day.
- Pityriasis versicolor – 300 mg per day once a week for 3 weeks, this regimen can be adjusted by the attending physician if necessary.
- Dermatomycosis, including lesions of the skin of the feet - 150 mg once a week for 3-4 weeks.
- Onychomycosis – 150 mg once a week, the course of treatment continues until the nail plate is completely replaced, and can be repeated if necessary.
- Deep endemic mycoses - the dosage of the drug varies from 200 to 400 mg per day, the duration of the course of therapy can reach 24 months.
The regimen for using Fluconazole capsules in children has certain similarities with adults. An important condition is to avoid exceeding the dose of 400 mg per day. In most cases, the regimen of use, dosage and duration of therapy are determined individually by the doctor.
Symptoms
The usual form of the disease and the chronic form of thrush are similar in their manifestations, but the latter is characterized by regularity and more vivid symptoms.
Signs of chronic thrush in women:
- itching in the vaginal and genital area, ranging from mild to unbearable;
- a burning sensation in the vagina, which intensifies during urination and sexual intercourse;
- the presence of swelling and redness at the site of the lesion;
- whitish, curd-like discharge, which becomes more abundant before menstruation, but in some cases there may be no vaginal mucus with an unpleasant odor;
- the appearance of microcracks on the genitals, causing pain and discomfort;
- dryness outside and inside the genitourinary system.
Contraindications for use
Medical contraindications for taking Fluconazole capsules are pathological and physiological processes in the patient’s body, which include:
- Simultaneous use of the drug terfinadine, astemizole, as well as other drugs that lead to prolongation of the QT interval on the electrocardiogram (especially when using Fluconazole capsules in a daily dosage exceeding 400 mg).
- Children up to 4 years old.
- Individual intolerance to the main active ingredient or additional substances of this medication.
The drug is used with caution in case of concomitant liver or renal failure, the appearance of a skin rash in patients with generalized systemic fungal infections, simultaneous use of the drug in a daily dosage of less than 400 mg with terfenadine, chronic alcoholism, in the case of the use of drugs that have a hepatotoxic effect, and also in patients with a high risk of developing arrhythmia (disturbance in the rhythm and frequency of heart contractions) against the background of organic heart pathology, electrolyte imbalance in the body. The drug is also used with caution in pregnant women. Before prescribing Fluconazole capsules, the doctor makes sure that the patient has no contraindications.
Side effects
Side effects are possible when using the drug Fluconazole
- From the immune system: hypersensitivity (cross with all azoles), other anaphylactic, anaphylactoid and allergic reactions (including Stevens-Johnson syndrome, toxic epidermal necrolysis, urticaria).
- From the nervous system: headache, dizziness, peripheral neuropathy, paresthesia, excessive fatigue, rarely - convulsions.
- From the digestive system: loss of appetite, dryness of the oral mucosa, changes in taste, abdominal pain, vomiting, nausea, diarrhea, flatulence, rarely - impaired liver function (jaundice, hepatitis, hepatonecrosis, hyperbilirubinemia, increased activity of alanine aminotransferase, aspartate aminotransferase, increased alkaline phosphatase activity, hepatocellular necrosis), including severe.
- From the hematopoietic organs: rarely - leukopenia, thrombocytopenia (bleeding, petechiae), neutropenia, agranulocytosis.
- From the cardiovascular system: increased duration of the QT interval, ventricular fibrillation/flutter, torsades de pointes.
- Metabolism: hypercholesterolemia, hypertriglyceridemia, hypokalemia, hyperglycemia.
- From the musculoskeletal system: myalgia.
- Other: weakness, asthenia, peripheral edema, neutropenia, itching, pulmonary edema, fever, excessive sweating, vertigo.
Use during pregnancy and lactation
There have been no adequate and controlled studies of the use of fluconazole in pregnant women. Several cases of multiple congenital defects have been described in newborns whose mothers received high-dose fluconazole therapy (400-800 mg/day) for most or all of the first trimester. The following developmental disorders were noted: brachycephaly, impaired development of the facial part of the skull, impaired formation of the cranial vault, cleft palate, curvature of the femurs, thinning and elongation of the ribs, arthrogryposis and congenital heart defects. Currently, there is no evidence of a connection between the listed congenital anomalies and the use of low doses of fluconazole (150 mg once for the treatment of vulvovaginal candidiasis) in the first trimester of pregnancy.
During pregnancy, the use of fluconazole should be avoided, except in cases of severe and potentially life-threatening fungal infections when the expected benefit of treatment to the mother outweighs the possible risk to the fetus. Women of childbearing age should use contraception.
Since the concentration of fluconazole in breast milk and plasma is the same, the use of the drug during breastfeeding is contraindicated.
Experience with the use of mycoflucan (fluconazole) for the treatment of vulvovaginal candidiasis
The infection of humans by yeast-like fungi of the genus Candida was first described in 1839 by B. Gantenbeg. He was able to detect fungal pseudomycelium in the form of whitish-yellow films in buccal ulcers. However, the existence of such a disease dates back to the 4th century BC. e. mentioned by Hippocrates. In 1849, identical fungi were discovered in vaginal infections. In 1880, Zops named the microorganisms that cause simultaneous lesions of the oral and vaginal mucosa Monilia albicans. The term “Candida” was adopted in 1939 by the III International Congress of Microbiologists, and in 1954 this term was confirmed by the VIII International Congress of Botanists.
Despite the more than 150-year history of studying candida vegetation in the reproductive tract of women, a number of unresolved issues still remain in the pathogenesis and treatment of this disease.
Candida albicans is a dimorphic commensal that lives in the genital tract and gastrointestinal tract, and is the etiological agent of vulvovaginal candidiasis in 85–90% of cases. Candidiasis lesions can also be caused by Candida glabrata and Candida tropicalis, in more rare cases - Candida guillermondii, Candida krusei, Saccharomyces cerevisiae.
The interest of obstetricians and gynecologists in the problem of candidiasis is due to the significant share of this pathology in the structure of gynecological diseases.
According to numerous publications, 75% of women of childbearing age experience episodes of fungal vulvovaginitis, but recurrent forms of the disease occur in only 5% of cases [1, 2].
Recent studies indicate that vaginal cells have autonomous immunocompetence and can function independently of systemic immune responses. The vaginal mucosa contains a large number of epithelial cells, dendritic-like Langerhans cells, macrophages and T-lymphocytes. Cellular immunity is provided by mononuclear cells and T-lymphocytes, which carry out the main protective function of the body during systemic candidiasis and mucosal candidiasis.
According to V.P. Prilepskaya [3], with vaginal candidiasis, the pathological focus is most often localized in the superficial layers of the vaginal epithelium. At this level, the infection can persist for a long time due to the fact that a dynamic balance is established between fungi, which cannot penetrate into the deeper layers of the mucous membrane, and the macroorganism, which inhibits their penetration, but is not able to completely eliminate the pathogen. Violation of this balance leads either to an exacerbation of the disease, or to recovery or remission.
As a study of patients with recurrent forms of vulvovaginal candidiasis showed, special strains of Candida albicans that are prone to persistence can contribute to the occurrence of relapses [4, 5]. In addition, frequent relapses may be due to disorders of the local immunity of the vaginal mucosa [6].
Biological factors predisposing to recurrence of the disease should also include a decrease in the amount of vaginal exudate, which promotes yeast colonization [7].
There are 3 clinical forms of genital candidiasis:
- asymptomatic colonization;
- acute urogenital candidiasis;
- chronic (recurrent) urogenital candidiasis.
Asymptomatic colonization of the vagina by Candida albicans occurs in 15-20% of young, non-pregnant and premenopausal women. Yeast-like fungi are present in the vagina in small quantities (<103 MOU/ml) and are represented by pseudomycelia. To colonize the vagina, it is enough to introduce only 102 MOU/ml of Candida albicans cells into it. With candidiasis, there are no complaints or clear clinical picture. In crops, budding forms of yeast fungi are found in small quantities in the absence of pseudomycelium.
The acute form of the disease is characterized by typical clinical symptoms, its duration does not exceed 1-2 months.
The recurrent form of the disease is diagnosed if the patient has 4 or more clinically significant episodes of candidal infection per year. Previously, the leading place in its genesis was assigned to infection of the genital tract by Candida species of non-albicans [1]. However, according to V. E. Malikov et al. (2002), this explanation of the chronicity of the process is not sufficiently substantiated. To a greater extent, it is due to incorrect treatment tactics for patients, which is carried out without taking into account sensitivity to antimycotics, and the prescription of antimycotics according to the generally accepted scheme [8].
The use of immunological methods made it possible to identify 3 categories of women with recurrent candidiasis. It has been established that cell-mediated immune responses of Th1 and Th2 types correlate with resistance and susceptibility to the development of mucosal candidiasis.
Type I immune response - type Th1, accompanied by the production of interleukin-2, γ-interferon, interleukin-12 (stimulating macrophages and polymorphonuclear cells), as well as IgA antibodies, is the dominant vaginal reaction, ensuring the maintenance of asymptomatic colonization of candida. Type II immune response - Th2 type with the production of interleukin-4, interleukin-5, interleukin-10, IgE antibodies, histamine and prostaglandin E2 - becomes dominant in cases where, under the influence of endogenous or exogenous factors, the number of Candida albicans increases. In type III immune response, the Th2 type turns off the Th1 type response and stimulates the development of a delayed-type hypersensitivity reaction.
Despite the creation and introduction into clinical practice of a large number of local and a number of systemic antifungal drugs, the treatment of vulvovaginal candidiasis is a rather complex task. At the same time, the most difficult problem to solve is the selection of therapy for patients with emerging fungal resistance to various antimycotic agents. This is largely due to the natural resistance of certain Candida species to the antifungal drugs used in clinical practice.
Most topical drugs have a primarily fungistatic effect, which largely contributes to the development of resistance to antifungals. Modern systemic oral antimycotics belonging to the azole class are selective inhibitors of the synthesis of ergosterol, the main component of the cell membrane of fungi, i.e., they have a fungicidal effect. In order for inhibitors of ergosterol synthesis to begin to act, they must penetrate inside the fungal cell, accumulate in sufficient concentration, move to the microsomes on which the target enzyme is located, and communicate with this enzyme [8].
The advantage of using the drug micoflucan (fluconazole), produced in India, belonging to the class of bis-triazoles, is determined primarily by the fact that, unlike ketoconazole, which, in addition to antimycotic properties, has a moderate antiandrogenic effect and affects a number of other metabolic processes, mycoflucan does not affect metabolic profile.
The purpose of this work was to evaluate the effectiveness of a single dose of micoflucan 150 mg orally for the treatment of vulvovaginal candidiasis.
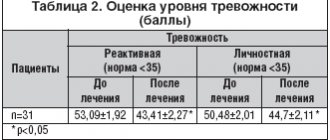
An open study was conducted in which micoflucan in capsules of 150 mg was prescribed to 31 women aged 20 to 55 years (mean age 31.8±0.4 years, mean body weight 63±0.6 kg). The study included patients whose diagnosis of vulvovaginal candidiasis was confirmed microscopically (mycoscopy of Gram-stained smears). In cases of ineffective therapy, a second dose of micoflucan was prescribed, followed by microscopic monitoring of vaginal smears after 10 days.
All patients complained of a feeling of discomfort, itching of the external genitalia, moderate or heavy curdled vaginal discharge. The diagnosis of vaginal candidiasis was made for the first time in 20 women; 11 patients had a history of several episodes of thrush, for which they had previously received courses of oral therapy with nizoral or local treatment with clotrimazole, Klion, pimafucin, and gyno-travogen. The duration of the disease ranged from 1 to 6 years. 20 women suffered from inflammatory processes of the genital organs for a long time, for which they were given multiple courses of antibiotic therapy. 10 patients had symptoms of cervicitis and/or ectopia of the cervix, 1 had vulvar candylomas, 2 patients suffered from diabetes mellitus.
Cure was stated when the clinical symptoms of the disease disappeared, improvement - with a significant weakening of the subjective and objective signs of the disease, and lack of effect - when the symptoms of the disease remained or worsened.
Control clinical and microscopic examinations were carried out 10 days after taking the drug. Based on the results of a control laboratory study of vaginal smears, treatment was assessed as effective in the absence of fungal spores and mycelium and as ineffective when the latter were detected by microscopy of Gram-stained smears.
The results of the study showed that after a single dose of 150 mg of mycoflucan, the majority of patients (61.3%) showed an improvement in the clinical symptoms of the disease on the second or third day of therapy. After 10 days, the symptoms of the disease (itching, profuse leucorrhoea, hyperemia and swelling of the vaginal mucosa) disappeared in 29 (93.5%) of 31 women. In 2 women, one of whom suffered from diabetes mellitus, and the other from HPV infection (human papillomavirus), clinical manifestations of vaginitis persisted. During control microscopy of smears, fungi were again detected in both patients, and therefore they were prescribed a second course of treatment with mycoflucan. After repeated administration of the drug, a therapeutic effect was achieved.
Thus, according to microscopy of smears performed 10 days after taking the drug, the mycological effectiveness of treatment with mycoflucan was 93.5%. After repeated administration of mycoflucan, mycological effectiveness was achieved in 100% of cases. Tolerance to the drug was 100%. No adverse reactions were noted.
The study revealed the high effectiveness of a single oral dose of 150 mg of mycoflucan in the treatment of episodes of vulvovaginal candidiasis and clinically confirmed the unique pharmacological properties of the drug.
The data obtained are consistent with the results of other authors, who noted clinical cure and mycological elimination of the pathogen in 90.5–92.1% of patients [9, 10]. The study made it possible to establish a clear connection between the effectiveness of treatment and the presence in the patient's history of factors predisposing to candidiasis, among which, from our point of view, special importance should be given to the formation of a relative immunodeficiency state. More often, such situations arise when there is simultaneous contamination of sexually transmitted pathogens. In our case, we did not obtain an effect in a patient infected with human papillomavirus types 16 and 18, who had previously received various antifungal treatments many times. According to S.I. Rogovskaya [10], the clinical manifestation of human papillomavirus infection is accompanied by changes in systemic and local immunity, which is manifested in an increase in the production of tumor necrosis factor and a decrease in interleukin-10 by epithelial cells, a decrease in the induction of γ-interferon and an increase in the content of interferon in the peripheral blood, as well as in changes in cellular immunity, which contributed to the persistence of vaginal candidiasis. The lack of effect from a single dose of micoflucan in a 55-year-old patient with severe diabetes mellitus, who did not receive adequate treatment aimed at maintaining a state of euglycemia, can be interpreted in two ways. Increased glucose content in urine and vaginal epithelial cells in severe diabetes, as well as dystrophy of the latter, can serve as predisposing factors for the introduction and proliferation of fungi [1]. According to Sobel et al. [11], diabetes and menopause are predisposing factors for the growth in the reproductive tract of these women of fungi of the species C. glabrata, which are initially resistant to fluconazole. According to V. E. Malikov et al. [8], there are 2 types of clinical course of chronic vulvovaginal candidiasis. One of the types involves true (non-microbiological) resistance. This means chronic recurrent candidiasis as a syndrome that develops against the background of defects in the immune system and a sensitization profile to fungal antigens. The only causative agent of this syndrome is Candida albicans.
The second type can be conditionally characterized by false resistance. It is caused by infection with a fungus other than Candida albicans, but treated according to the standard traditional regimen, without taking into account the etiology of the infection. According to Czaika et al. (2000), fluconazole therapy in doses less than 800 mg/day does not exceed adaptation barriers for C. glabrata [12].
It should be noted that there are no adverse reactions when taking micoflucan and its high compliance, which significantly increases adherence to treatment. The lack of effect of 6.5% from a single dose of 150 mg of mycoflucan apparently dictates the need for individual selection of antimycotics, taking into account the species selection of Candida strains and predisposing factors for the development of candidiasis. Thus, 150 mg of mycoflucan in the form of 1 tablet. for oral administration can be considered an effective treatment for episodes of vulvovaginal candidiasis.
Literature
- Prilepskaya V.N., Bayramova G.R. Vaginal candidiasis: etiopathogenesis, clinical picture, diagnosis, principles of therapy // Contraception and women's health. - 2002. - No. 1. — P. 3-8.
- Geiner AM. Foxman V. Risk factors in vulvo-vaginal candidiasis: a case control study among college students // Epidemiology -1996;7:182-7.
- Prilepskaya V.P. Vulvovaginal candidiasis: modern methods of treatment // Practical gynecology. - M., 2001. - P. 177-189.
- Vazquez JA, Sobel JD, Demitriou R, Vaishampayan J, Lynch M, Zervos MJ Karyotyping of Candida Albicans isolates obtained longitudinally in women with recurrent vulvovaginal candidiasis. J Infect Dis 1994;170:1566-9.
- Spinillo A, Carratta L, Pizzolli G, et all Recurrent vaginal candidiasis: result of a cochort study of sexual transmission and intestinal reservoir // J Reprod Med 1992;37:343-7.
- Fidel PJ Jr, Sobel JD Immunopathogenesis of recurrent vulvovaginal candidiasis. Clin Microbiol Rev 1996;9;335-48.
- Hilton E., Ch and rase karan V., Rindos P., Iscnberg HD Association of recurrent Candidas vaginitis with inheritance of Lewis blood group antigens. J Infect Dis 1995; 172:1616-9.
- Malikov V. E., Zharikova N. E., Romanovskaya T. A., Rasskazov D. N. Etiology of vaginal candidiasis and the problem of resistance to antifungals // Contraception and women's health. - 2002. - No. 1. - pp. 9-16.
- Ankirskaya A. S., Muravyova V. V., Demidova E. M., Karpova O. Yu., Zaidieva Ya. Z., Fursova S. A. Diflucan 150: experience in the treatment and prevention of vaginal candidiasis // Bulletin of Dermatology and Venereology . - 1998. - No. 3. - S. - 65–67.
- Rogovskaya S.N., Prilepskaya V.N., Bayramova G.R. Experience of using Diflucan in the treatment of genital candidiasis // Bulletin of Dermatology and Venereology. - 1997. - No. 1. — P. 100-101.
- Sobel J., Faro S., Forse R. et al. Vulvovaginal candidiasis: Epidemiologic, diagnostic, and therapeutic considerations // Am.J.Obstet.Gynecol.- 1998.-Vol. 178.-P. 203—211
- Rogovskaya S.I. Human papillomavirus infection of the lower genitalia: clinical picture, diagnosis, treatment // Dissertation... doc. honey. Sci. — 2003.
- Czaika Vertal antifungal susceptibility testing in chronically recurrent vaginal candidosis as basis for effection therapy // Mycoses 2002-Vol. 43/Suppl 2- p 45-50.
V. P. Smetnik , Doctor of Medical Sciences, Professor L. A. Marchenko , Doctor of Medical Sciences G. E. Chernukha , Doctor of Medical Sciences Scientific Center of Obstetrics, Gynecology and Perinatology of the Russian Academy of Medical Sciences, Moscow
special instructions
Treatment with fluconazole may be initiated pending the results of cultures and other laboratory tests, but therapy should be adjusted accordingly once the results of these tests are available.
During treatment, it is necessary to monitor blood counts, kidney and liver function. If renal and liver dysfunction occurs, you should stop taking the drug.
Treatment must be continued until clinical and hematological remission occurs (an exception is acute vaginal candidiasis). Premature cessation of treatment leads to relapses.
People with AIDS are more likely to develop severe skin reactions when taking many drugs. In cases where a rash develops in patients with a superficial fungal infection and is assessed as definitely related to fluconazole, the drug should be discontinued. If a rash occurs in patients with invasive/systemic fungal infections, they should be closely monitored and fluconazole should be discontinued if bullous changes or erythema multiforme occur.
In rare cases, the use of fluconazole has been accompanied by toxic changes in the liver, including death, mainly in patients with serious concomitant diseases. In the case of hepatotoxic effects associated with fluconazole, there was no obvious dependence on the total daily dose, duration of therapy, gender and age of the patient. The hepatotoxic effects of fluconazole were usually reversible; its signs disappeared after cessation of therapy. If clinical signs of liver damage that may be associated with fluconazole appear, the drug should be discontinued.
Treatment regimen for chronic candidiasis
To destroy a fungal infection, local and systemic antifungal drugs are prescribed:
- tablets, capsules;
- ointments, creams, suppositories.
A comprehensive treatment regimen necessarily includes drugs from the group of immunomodulators, which help restore the immune system and improve its functioning. After antifungal therapy is completed, it is necessary to normalize the vaginal microflora by introducing beneficial bacteria into it. These microorganisms will inhibit the growth and reproduction of the fungal infection and prevent the disease from reoccurring.
To restore the balance of microflora, the following can be used:
- suppositories with bifidobacteria;
- suppositories with lactobacilli.
In the second case, treatment should be carried out under the constant supervision of a gynecologist, because improper use of suppositories with lactobacilli can cause an exacerbation of recurrent thrush.
If, after complex drug therapy, chronic candidiasis does not go away completely, additional physiotherapeutic procedures are prescribed, such as:
- laser therapy;
- magnetic therapy;
- electrophoresis;
- mud baths and wraps.
The procedures will help strengthen both general and local immunity, suppress the activity of bacteria and fungi, and reduce the number of episodes of relapse to a minimum.
With frequent exacerbations, it is important not only drug treatment of chronic candidiasis, but also adherence to the rules of a healthy lifestyle. In order for it to stop bothering you, you need to balance your diet, get rid of bad habits, eliminate stress factors, engage in moderate physical activity, and take care of your personal hygiene.
You can find out how much it costs to treat chronic candidiasis at the Healthy Family medical clinic by calling +7 (495) 185 93 07 or ordering a call back. After receiving your request, our administrators will contact you and answer all your questions.