Non-menstrual bleeding from the genitals is a sign of uterine bleeding. This pathology is a dangerous symptom of gynecological diseases.
Appointment with a gynecologist - 1000 rubles. Comprehensive pelvic ultrasound - 1000 rubles. Appointment based on ultrasound or test results - 500 rubles (optional)
You cannot hope that the bleeding will stop on its own: due to blood loss, anemia will begin, and the cause of the discharge will become chronic. The result will be infertility, purulent inflammation, atrophy of the tissues of the uterus and adjacent organs, cancerous tumors and other dangerous pathologies.
Symptoms of uterine bleeding
The content of the article
Any discharge of blood from the vagina other than normal menstrual flow is considered bleeding.
In this case, two menstrual disorders are distinguished:
- Menorrhagia , which is heavy uterine bleeding that occurs at regular intervals (during menstruation);
- Metrorrhagia is irregular bleeding.
Pathological (disease-related) discharge can be distinguished from physiological discharge by several criteria. Characteristic symptoms of bleeding:
- Rich color due to blood admixture: blood red, scarlet, burgundy;
- Duration: bleeding begins outside the menstrual period (metrorrhagia) or menstruation lasts longer than normal - from 5 days (menorrhagia);
- Consistency: discharge may contain blood without impurities, blood with mucus impurities or inclusion of dark burgundy or burgundy-gray clots;
- Smell: not typical of menstrual discharge - during uterine bleeding, the discharge smells like blood, spoiled fish, meat, etc.
The volume of discharge in menorrhagia and metrorrhagia is also different:
- During menstruation (menorrhagia), the discharge is very heavy - about 80 ml per day (hygienic products have to be changed more often than after 2-3 hours);
- Outside of menstruation (metrorrhagia), the volume of excretion varies - blood smears (in common parlance - daub), drips or continuously flows.
- With persistent menopause, even a drop of blood is pathological.
Uterine bleeding is accompanied by symptoms of diseases associated with blood loss. The woman suffers from: dizziness, weakness, flickering spots in the eyes, ringing in the ears, shortness of breath, increased heartbeat. Gradually the symptoms intensify, fainting is possible. At the same time, pathology makes itself known - the cause of bleeding. Most often, abdominal pain begins, temperature rises, etc.
How to assess the intensity of bleeding
At an appointment with a gynecologist, it is very difficult to determine the amount of blood lost per day, so some gynecologists focus on filling and changing hygiene products. One pad contains approximately 5 ml, and one pad contains from 5 to 15 ml, depending on the absorption strength. Based on this, more than 16 tampons or 6 to 16 blood-soaked tampons indicates 80 ml of wasted blood. There is a subjective scale for assessing the intensity of release:
- Minor discharge. A few spots on the female's smear at the end of the day correspond to a daily blood loss of 5-6 g.
- Very light. The hygiene product is changed 1-2 times a day, which is equivalent to the loss of 6-9 g of blood.
- Lungs. A feminine sanitary pad or regular tampon is changed 3-4 times a day. This blood loss corresponds to 8-13 g per day.
- Moderate. If a tampon or (normal) tampon is changed every 4-5 hours, we can talk about blood loss of 12-15 g per day.
- Strong. Super hygienic products must be replaced after 3 hours. This is 15-18 g of blood per day.
- They are very strong. Super absorbent tampons and pads get wet within an hour. This condition requires urgent medical attention; blood loss cannot be counted. This is a clear sign of menorrhagia.
It is important to consider that the intensity of blood loss during menarche varies and depends on the day of the cycle: in the first days the discharge will be moderate, and in subsequent days it will be light and barely noticeable. The normal amount of blood released is considered to be 250 ml, which corresponds to one glass. Anything is considered a possible menorrhagia.
Causes of menorrhagia and metrorrhagia
Uterine bleeding is a symptom of diseases of the uterus, ovaries and pregnancy pathologies.
Causes of bleeding outside of pregnancy:
- Injuries received during gynecological procedures - examinations, abortions, diagnostic curettages, removal of tumors, etc.;
- Cervical erosion, which is an ulcer at the entrance to the organ;
- Hormonal disorders resulting from the growth of polyps, endometrium - the mucous membrane of the uterus, etc.;
- Inflammation of the uterus, ovaries;
- Chronic STIs;
- Cancerous tumors of the uterus, fibroids, ovarian cysts.
Causes of bleeding during pregnancy and after childbirth
Bleeding during pregnancy, even a slight one, indicates the onset of a miscarriage, ectopic pregnancy, frozen pregnancy, or premature birth.
The causes of such complications during pregnancy are pathologies of the uterus, cervix, hormonal disorders, fetal diseases (genetic, leading to miscarriage, or infectious).
After childbirth, bleeding is associated with postpartum complications - ruptures, injuries, uterine inversion.
Causes of bleeding during menopause
After the extinction of sexual function - during menopause - the hormonal background of a woman changes. On this basis, diseases associated with a lack of certain hormones develop. This includes various tumors, polyps, cysts, endometrial growths, uterine prolapse, etc. A symptom of all these pathologies is discharge mixed with blood.
Causes of sudden and severe bleeding
- Uterine trauma
. Such injuries can be caused by rough sex, especially rape, criminal surgical abortions (they are done through acquaintances in underground conditions, when gynecologists refuse to operate due to timing or contraindications), etc. - Miscarriage
. If a woman has lost her child and does not go to the clinic, severe uterine bleeding is possible. - Polyp torsion, cyst rupture, tube rupture during ectopic pregnancy. All these conditions are also accompanied by severe uterine bleeding.
Juvenile metrorrhagia
Juvenile metrorrhagia occurs in adolescence and is usually due to the following reasons:
- imbalance of hormones due to psycho-emotional stress, infectious diseases, significant physical activity, PCOS.
- disorders in the hemostatic system (for example, thrombocytopenia)
- development of space-occupying formations (for example, ovarian cysts).
It is necessary to differentiate between juvenile bleeding and menstruation when the cycle has not yet been established.
First aid for uterine bleeding
It is impossible to cure the pathology on your own, as well as to identify the cause of this condition. Therefore, you need to contact a gynecologist and undergo a series of studies: tests and ultrasound.
In case of severe bleeding, when the blood flows without stopping, you need to call an ambulance. Before the doctors arrive, you need to provide first aid to the patient. It consists of the following actions, you can:
- Lay the patient on a flat surface, placing a pillow under her feet - they should be approximately 20 - 30 cm above body level;
- Apply a cold object (for example, a bottle of cold water) to the lower abdomen;
- The patient should be given sweet drinks.
If you are pregnant, you should call an ambulance in any case.
How does the menstrual cycle work?
To understand why metrorrhagia is a pathology, you should study the menstrual cycle and all the changes that occur during this period.
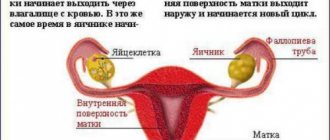
Menstruation is the first phase of the menstrual cycle. It is called follicular, because during this period the follicle with the egg inside begins to mature. During this time, the levels of various hormones, especially estrogen, increase.
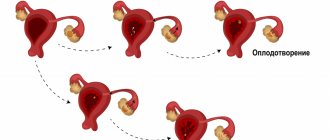
The follicular phase ends, giving way to ovulation, approximately in the middle of the cycle. The onset of ovulation is promoted by the hormones estradiol and luteinizing hormone. On this day, the egg leaves the follicle and moves through the fallopian tubes to the uterus. Fertilization occurs in the removed tube.
The second phase of the cycle is the luteal phase (corpus luteum phase). It occurs after ovulation and characterizes the period of development of the corpus luteum, which appears at the site of the egg in the ovary. The corpus luteum actively produces progesterone (pregnancy hormone). During the luteal phase, the body actively prepares for a possible pregnancy. The endometrium of the uterus thickens. This period lasts on average 13 days.
If fertilization does not occur, the egg dies. The brain receives the command, the corpus luteum dies. The inner layer of the uterus is shed and discharge begins. The corpus luteum leaves the body along with them.
Diagnosis of the causes of menorrhagia and metrorrhagia
The gynecologist determines the cause of bleeding based on test results and ultrasound.
- A gynecological examination in a chair will show whether there is prolapse of the genital organs, neoplasms or erosion on the cervix. During pregnancy, cervical insufficiency is clearly visible. Also, already at this stage, injuries from the spiral, after sexual intercourse, etc. are visible;
- Colposcopy. A gynecologist conducts an examination with a device equipped with magnifying glasses. Using a colposcope, internal pathologies of the cervix are identified, and the nature and stage of erosion is determined.
- An ultrasound of the uterus will determine whether there are injuries, neoplasms, or inflammation of the female internal organs.
- Smears for microflora and cytology show STI infections (STDs), precancerous conditions, and cancer.
- A blood test for hormones will determine whether there is a hormonal imbalance.
If this is not enough, you will have to undergo an MRI (tomography) to obtain images of the organs in 3D format at high magnification.
Prevention
Since metrorrhagia can appear in children, health-improving and strengthening activities should be carried out at an early age. It is important to treat all diseases, especially of the genital organs, and also to prevent abortions.
During pregnancy, prevention should begin in the first trimester. In general, a woman should lead an active lifestyle, get proper rest and establish a work routine.
To restore the menstrual cycle, therapy with oral estrogen-progestin contraceptives is prescribed. The treatment regimen is as follows:
- 5-25 days the first three cycles;
- 16-25 days three more cycles;
- progestin drugs on days 16 to 25 for 4-6 months.
Hormonal therapy with contraceptives helps not only to get rid of metrorrhagia, but also to prevent unplanned pregnancy. Contraceptives will be an excellent prevention of hormonal imbalance, infertility (anovulatory), breast cancer and adenocarcinoma.
Treatment of bleeding in menorrhagia and metrorrhagia
First of all, the gynecologist stops the bleeding. Pregnant women are prescribed drugs that relax the uterus and hormones that stop a miscarriage. The rest of the women are prescribed various hemostatic drugs, hemoglobin-supporting drips are placed, and in severe cases a blood transfusion is required.
At the same time, the disease itself is being treated. Depending on the cause, antibiotics and hormones may be taken. If neoplasms or erosion are detected, surgery is performed to remove polyps or fibroids, cauterize the erosion, curettage the uterus, etc. The list of possible measures is endless.
It is important to understand that only a timely visit to a gynecologist, high-quality diagnosis and effective treatment will help stop bleeding and get rid of the disease. Advanced pathologies accompanied by bleeding lead to removal of the uterus, infertility and severe purulent inflammation, since blood and lack of air in the uterus are an ideal environment for the development of putrefactive bacteria.
Treatment of bleeding during pregnancy
Bleeding during pregnancy is dangerous - it is a sign of an ectopic pregnancy, the onset of a miscarriage or early labor. If you notice discharge, especially accompanied by nagging pain (abdomen, lower back), you need to call an ambulance. You need to lie down until the ambulance arrives. You can take a No-shpa tablet, which relieves uterine spasms.
Treatment for bleeding during pregnancy depends on the cause:
- Ectopic pregnancy .
Pregnancy outside the uterus is a common occurrence, and only an obstetrician-gynecologist can distinguish it from normal. Severe bleeding with an ectopic is a sign of rupture of the organ where the fetus has taken root. In this case, an urgent operation is performed. - Miscarriage or premature birth
. At first a slight spotting appears, after a while the discharge intensifies. This occurs when the cervix opens and the fetus comes out.
With timely treatment, pregnancy can be saved. The gynecologist will prescribe hormonal medications and vitamins that relax the uterus. If a miscarriage occurs, the uterus is curetted. If this is not done, the remaining placenta will fester, resulting in blood poisoning.
Treatment of bleeding after childbirth or surgery
Discharge after pregnancy should last no longer than 2 weeks. Symptoms such as abdominal pain and an unpleasant smell of discharge indicate that inflammation of the uterus has begun. If you have such symptoms, contact your gynecologist. The doctor will take swabs for infections and perform an ultrasound of the pelvis.
Pathological uterine bleeding after childbirth is a sign of inflammation, non-healing wounds, incomplete passage of the placenta and other complications after pregnancy. Treatment in this case also depends on the cause. Strong antibiotics are often needed. Therapeutic curettage may be required. With timely help, problems go away and the body recovers. Advanced pathology guarantees peritonitis - purulent inflammation of the uterus and peritoneum.
Treatment of bleeding during menopause
The first stage of menopause lasts up to 2 years. During this period, scanty discharge, similar to menstruation, is not dangerous. Heavy bleeding or blood after the onset of persistent menopause is a consequence of tumors, prolapse of internal organs and other processes associated with the aging of the body.
The gynecologist will prescribe blood tests for coagulation and tumor markers (indicating cancer), and conduct an ultrasound of the pelvis. If tumors are found, a biopsy will be required.
To treat bleeding during menopause, a modern technique is often used - hormone therapy, and tumors are removed. If everything is really bad, the uterus is removed. After menopause, it is quite possible to live without this organ.
Metrorrhagia during perimenopause
Perimenopause includes both the period of perimenopause and menopause itself, as well as several years after its onset. Bleeding during this period may have the following causes:
- Hormone imbalance
- Hyperplastic changes in the endometrium
- Uterine fibroids
- Disorders of the hemostasis system
- Endocrine pathologies
During premenopause, ovarian function declines with an increase in the number of anovulatory cycles. A decrease in progesterone production, absence or insufficient function of the corpus luteum causes excess estrogen production and the development of hyperplastic processes in the endometrium.
In the postmenopausal period, one of the most common causes of bleeding is endometrial cancer, which requires immediate consultation with a doctor to identify the causes of metrorrhagia. Since this symptom appears at an early stage, timely diagnosis allows for effective treatment.
If you have any questions related to metrorrhagia, you can ask the doctors at Nova Clinic. You can make an appointment with a doctor by calling the number listed on the website or using the booking button.
Is it possible to cure uterine bleeding with folk remedies?
Uterine bleeding is a symptom of a huge variety of diseases and requires especially careful attention due to the likelihood of serious consequences for life and health. Any discharge of blood from the vagina that is not associated with normal menstruation should be taken as a reason for an urgent visit to a gynecologist.
Having noticed signs of uterine bleeding, many women try to treat themselves, resorting to traditional medicine, which can lead to tragic consequences. Folk remedies against uterine bleeding, such as infusions of nettle, viburnum, horsetail and shepherd's purse, do demonstrate some effectiveness, but are used only as an addition to the main therapy after consultation with the attending physician.
Complications of menorrhagia
Menorrhagia is often not diagnosed on time, while potential complications can occur at any time and ruin a woman's social and emotional life. The main complications include:
- Anemic syndrome. Develops due to excess blood loss and decreased hemoglobin concentration. General health worsens, chronic fatigue and pale skin appear. Hair may fall out.
- Acute blood loss syndrome. The amount of blood released becomes too large, the volume of circulating blood drops to a critically low level, which is a threat to life.
- Very rarely, death due to multiple organ failure due to anemic syndrome or a blood clotting disorder with chronic abnormal uterine bleeding that occurs on a regular basis.
GYNECOLOGICAL COMPLICATIONS IN WOMEN WITH INCREASED BLEEDING
Rice. 2.
Blood clot formation
Fibrin clot formation
At this stage, a network-like covering of the blood clot is formed - a fibrin clot (blood clot), formed through the interaction of 13 plasma clotting factors, numbered in Roman numerals from I to XIII (Fig. 3).
Deficiency of any of these proteins can result in delayed or incomplete clot formation and subsequent resumption of bleeding when the clot forms temporarily, requiring reinforcement with a fibrin clot. Rice.
3. Fibrin clot formation
Problems with increased bleeding in women
Bleeding problems can be inherited or acquired during a woman's life. Acquired increased bleeding can be caused by certain types of medications, treatments, malignant diseases and autoimmune disorders. Let us dwell on hereditary problems, which most often cause bleeding problems in women.
von Willebrand disease
Von Willebrand disease (VWD) is reported to be the most common cause of excessive bleeding in humans.
Rice.
4. Inheritance of von Willebrand disease
The presence of von Willebrand disease (VWD) is caused by a gene passed from parent to child. The abnormal von Willebrand disease gene is located on one of the regular chromosomes, not on the sex chromosome (like hemophilia), and therefore VWD occurs with equal intensity in both men and women. Often, an accurate family history can help a doctor diagnose the condition. Sometimes an abnormal gene may manifest itself for the first time in a patient when neither of the parents possessed it. This is called a new "mutation", and the disease can then be passed on to successive children in the usual way. A specific test for the von Willebrand factor gene (DNA test) is now available for some forms of von Willebrand disease. It is sometimes possible to trace von Willebrand disease over several generations. The figure above shows the usual pattern of dominant inheritance. Although the genetic defect is inherited in an autosomal manner, it does not follow the classical pattern of autosomal dominant or autosomal recessive inheritance. Moderate VWD and some forms of the disease (type 2A or 2B) appear as a consequence of the autosomal dominant model; severe VWD, with von Willebrand factor, occurs only when two genes are defective.
The exact prevalence is unknown, but some estimates suggest it is present in 1% of the world's population. BV occurs throughout the world among people of all socioeconomic and ethnic groups. This is an autosomal disease (that is, it affects both men and women equally) (Fig. 4). There are three main types of VWD depending on whether the VWF defect is quantitative or qualitative. In VWD type 1, there is a deficiency of von Willebrand factor (vW). Type 2 VWD, which has four subtypes, occurs when there is a qualitative defect in vWF (the factor does not function properly). In type 3, vWF is almost or completely absent. Most types are inherited in an autosomal dominant manner. Type 3 and 2N are inherited in a recessive manner. It is important to know which type of BV each individual patient has because treatment for different types of disease is different. If there is a significant decrease in vWF, as in type 3, or a problem with vWF associated with factor VIII, as in type 2N, then a significant decrease in factor VIII relative to normal may also occur. Sometimes people with type 3 or 2N BV are misdiagnosed as having hemophilia due to significantly reduced factor VIII. To prevent such misdiagnosis, it is necessary to check the level of factors VIII and von Willebrand when determining a blood coagulation disorder in a patient.
Signs of BV are expressed in the body's inability to form a blood clot. Bleeding mainly occurs from the mucous membrane and (or) skin. The most common signs are the presence of a large number of bruises on the body, frequent or prolonged nosebleeds, heavy or prolonged menstrual bleeding (menorrhagia) and prolonged bleeding from wounds, surgery, tooth extraction and in women in labor during childbirth. Gastrointestinal bleeding may also occur. Joint bleeding in BV is less common than in hemophilia and usually occurs in patients with low levels of factor VIII in the blood.
Hemophilia
Since the inheritance principle of hemophilia A (factor VIII deficiency) and hemophilia B (factor IX deficiency) is a sex-linked recessive trait, women extremely rarely suffer from these diseases. It is more possible, but unproven, that bleeding occurs in female carriers of hemophilia A or B. A symptomatic carrier with low levels of factor VIII or IX may experience increased bleeding in the same way as a patient with mild hemophilia during surgery or trauma. In women, however, abnormal periods may be the only symptom. Irregular, heavy or prolonged menstrual periods are the most common symptoms among carriers of the hemophilia A and B genes. Excessive bleeding associated with pregnancy and childbirth can also occur in cases where factor levels are below 30%. Female carriers whose factor level allows them to be classified as having a mild form of hemophilia require the same treatment for bleeding as men with a mild form of hemophilia. Clinically there is no difference.
Mixed diseases
Deficiency of any of the blood clotting proteins (factors) may indicate signs of varying degrees of severity as well as quantitative and qualitative platelet defects. Most symptoms of such defects will resemble those of von Willebrand disease. Some diseases associated with deficiency of blood clotting factors are quite mild (for example, factor XII deficiency). Others, such as hypofibrinogenemia (deficiency of the clotting factor fibrinogen) are particularly problematic. Many of these diseases are inherited autosomalally by women and men equally.
Gynecological symptoms observed in women with increased bleeding
Menorrhagia/metrorrhagia
Prolonged and heavy menstrual bleeding is the most common hemorrhagic symptom observed in women with bleeding problems. Some suffer from excessive bleeding during the menstrual cycle (menorrhagia); others experience similar problems immediately after the end of the menstrual cycle (metrorrhagia). The uterus is a highly vascular organ capable of losing large amounts of blood over a short period of time. Prolonged bleeding can cause iron deficiency anemia. Therapeutic interventions such as dilatation and curettage of the walls of the uterine cavity usually only worsen the situation, since the alignment of the lining tissues of the uterus prevents the formation of a fibrin clot, the uterine cavity remains unprotected and the resumption of hemostasis is complicated.
Dysmenorrhea and mid-cycle pain
Another common complaint among women with excessive bleeding is pain during menstrual periods and mid-cycle pain. One can only speculate about their reasons, since no reliable scientific data on this issue exists. Some women may experience pain as a result of heavy bleeding and incomplete formation of clots in the uterus. In other cases, there is pain in the pelvis or abdomen, which occurs with endometriosis. Endometriosis is an abnormal condition in which the growth of endometrial tissue occurs in the abdominal cavity outside the uterus. When any woman is on her menstrual period, the intrauterine tissue - wherever it is - will bleed. If a woman has a bleeding disorder and endometriosis, tissue outside the uterus may bleed, causing peritoneal irritation (irritation of the peritoneum) and pain.
I have spoken with women who experience excessive bleeding during ovulation and experience severe pelvic pain. When the egg is released from the ovary, healthy women experience very little bleeding. But in women with bleeding disorders, this can be a significant problem. I once met a woman with von Willebrand disease type 3 whose bleeding during ovulation was so intense that she had to take birth control pills for the rest of her life to avoid ovulation.
Conception/fertility problems
Many women with bleeding problems use birth control pills or other hormone therapy. Obviously, this affects a woman's ability to conceive. The long-term effect of such long-term hormonal therapy is not known. It is also unknown whether von Willebrand factor deficiency has any effect on the ability of a fertilized egg to attach to the uterine wall, which in turn may affect the ability to carry a fetus to term. It seems casuistic that there is a higher likelihood of miscarriage in women with BV than in the general case. This may be simply because when a miscarriage occurs, the subsequent excessive bleeding forces the woman to seek medical attention and her diagnosis is noted. At the same time, a miscarriage that occurs in the early stages of pregnancy in an ordinary woman may not even be perceived as such. The bleeding that follows spontaneous termination of pregnancy can be quite significant, since the high level of clotting factors naturally maintained in the blood during pregnancy decreases sharply after the loss of the fetus. Postpartum bleeding can be a problem for women with bleeding disorders. Depending on the disease, problems may be small or very minor because hormones that rise during pregnancy cause clotting factors to increase. This is especially true for factors VIII and von Willebrand. However, even if there are no complications immediately after birth, postpartum hemorrhage may occur a few days later, when hormone levels and levels of clotting factors begin to decline. Patients with von Willebrand disease have a greater number of primary (immediate) and secondary (delayed) postpartum hemorrhages. In women who breastfeed, hormone levels remain high, but it is not known whether this protects against postpartum hemorrhage. Pregnancy does not provide any protection to women with VWD type 2, since hormonal increases and increases in von Willebrand factor do not alter the functional impairment of vWF. Factor IX levels do not increase during pregnancy.
Diagnosis of hereditary diseases that cause increased bleeding
For non-hematology physicians, including obstetricians-gynecologists and family physicians, diagnosing a bleeding disorder can be challenging at best. First responders typically rely on prothrombin time (PT) and activated partial thromboplastin time (aPTT) tests and, to a lesser extent, clotting-bleeding time to make a diagnosis. The difficulty with this is that the most common bleeding disorder in women, von Willebrand disease, cannot be detected using these tests.
In von Willebrand disease, there are no changes in PT, and the aPTT is only occasionally prolonged. Increased PT occurs only with a deficiency of factors X, VII, V, II, I, or with certain liver diseases. The aPTT is prolonged only when the patient has a deficiency of factors XII, XI, X, IX, VIII, V, II or I. The aPTT in von Willebrand disease is prolonged only if the level of factor VIII is below 40%. For patients with qualitative type 2 VWD (except 2N), the aPTT will usually be normal. Bleeding time can be normal or prolonged. Bleeding time testing is not very accurate. This is a superficial test to assess platelet function and can be affected by various external factors, such as a cold. VWF testing should include a ristocytin cofactor test, which assesses the function of VWF, the antigen to VWF, which measures vWF levels and factor VIII levels. Many doctors also use the test to evaluate the binding capacity of vWF collagen. Additional tests, such as the vWF multimer assay, are used to study protein structure, which is especially useful in studying the different subtypes of von Willebrand disease type 2. There is no perfect test for diagnosing VWD.
Laboratory tests to determine the presence of BV are often negative or inconclusive and may require repeat testing for confirmation. People with BV may have cyclical variations in their levels, making diagnosis difficult, especially in its milder forms. The timing of the test is important. It is better to test a woman during her menstrual cycle, when hormonal and factor norms are at their lowest. When performing a coagulation test, it is important for the examiner to consider any environmental factors or medications that may affect the accuracy of the test. Hormonal therapy such as oral contraceptives, due to their stimulating effect on vWF and factor VIII, should be interrupted before testing. The use of certain drugs that have contraindications that affect platelet function should also be discontinued. This is aspirin and most non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen, diclofenac, Voltaren, Celebrex, etc. Because of a number of reasons that can affect the accuracy of the result and normal fluctuations in factor levels, it is necessary to repeat tests in women with a history of bleeding, even if the test results are normal at the time. It is also necessary to refer the woman to hematologists with experience in treating bleeding disorders.
These hematologists are typically affiliated with treatment centers throughout the United States and around the world. Special tests necessary to establish a diagnosis usually require the use of specialized equipment, reagents and technology. Laboratory errors in the assessment of coagulation problems are common among non-specialized laboratories. Very few of the women I interviewed were diagnosed without repeated testing. This is a huge waste of time and money.
Treatment of gynecological complications in women with increased bleeding
The various treatments described below have been successful in the women I interviewed. This list is not final. You should consult your doctor to determine the appropriate method for your particular case.
Hormone therapy
Oral contraceptives (OCs) are very effective in increasing levels of factors II, VIII, and von Willebrand factor. For this reason, they are especially useful in treating heavy menstrual periods as well as other bleeding in women. Women often report that during their menstrual period and taking placebo pills (pacifiers), they also have an increase in the number of strokes and nosebleeds, which decrease once they take the contraceptives again. For symptomatic carriers (factor VIII), OC may be the only possible treatment option. For women with qualitative VWF defects, the effectiveness of oral contraceptives is reduced because the hormones increase VWF levels but do not correct the inherent structural defects. For these women, OCs probably have some success in helping regulate their menstrual periods and reduce bleeding, but other treatments may also be necessary. For bleeding not sensitive to OCs, the use of pure progestin components, such as Norulat and Provera, can be very useful because they cause thickening of the lining uterine tissue (secretory myometrium) and stop bleeding. Question: How long can you stop menstruating? Some doctors prefer the use of progesterone components such as Depo-Provera for intramuscular administration, although the results, according to surveys of women, vary. Progesterone components when deposited intramuscularly are unsafe for a number of reasons:
1. They require an intramuscular injection, which is not recommended for people with bleeding problems. 2. If side effects occur in some patients during administration, they may last for several months, whereas the half-life for oral contraceptives is much shorter. 3. Dosage can be better managed with the assistance of a specialist. Strictly speaking, in case of life-threatening bleeding, the use of intravenous combined estrogens (Premarin) is very effective.
Desmopressin acetate
This medication is usually administered by injection (intravenously or subcutaneously - DDAVP) and intranasally (nasal drops - Stimate). It is chemically related to antidiuretic hormone (vasopressin). When used, DDAVP causes a dramatic increase in circulating plasma factor VIII and von Willebrand factor, stimulating the production of these proteins from blood vessel walls. This drug is very effective in treating bleeding in women with type 1 BV and symptomatic carriers of hemophilia A with factor VIII deficiency. It is less effective for women with type 2 VWD because it does not correct the molecular defects in von Willebrand factor. The drug is ineffective in VWD type 3, where little or no VWF is produced, and should not be used in type 2B due to excessive platelet binding and subsequent thrombocytopenia. (Thrombocytopenia is a condition characterized by a decrease in the number of platelets and, accordingly, an increase in bleeding). Unfortunately, DDAVP does not provide any benefit to female symptomatic carriers of hemophilia B because it has no effect on factor IX. When a "strong" spray (Stimate) is prescribed, doctors do so because there is a less concentrated formulation of intranasal desmopressin called DDAVP used to treat nocturnal enuresis. This less concentrated form of the drug is correspondingly ineffective for patients with increased bleeding.
Plasma preparations
Women with increased bleeding who are not sensitive to desmopressin or active hormonal therapy are indicated for replacement therapy for clotting factor deficiency or defectiveness. Today, with the advent of more reliable, virus-inactivated lyophilized plasma preparations (factor concentrates) in many countries, the use of preparations such as cryoprecipitate or fresh frozen plasma is unacceptable. The US National Hemophilia Organization and Scientific Advisory Board recommend against their use if virus-inactivated drugs are available. In the United States and other countries where safe and hemostatically effective drugs are available for the treatment of bleeding associated with disorders of factors II, VII, VIII, IX, X, and von Willebrand factor. In the United States, the two most widely used drugs for treating von Willebrand disease are Humate-P (Haemate-P in other countries) and Alphanate SD. Both of these drugs are concentrates with high levels of factor VIII and von Willebrand factor. Monoclonal or recombinant factor VIII preparations should not be used for VWD because they do not contain von Willebrand factor.
Antifibrinolytics
Drugs such as aminocaproic acid may be useful in treating menstrual bleeding, as well as bleeding from the mucous membranes of the nose and mouth. These medications do not form a clot, they simply keep the clot in place longer by blocking the enzymes responsible for fibrinolysis (the spontaneous, normal process of breaking up a clot once it has formed). These drugs should not be used for joint and kidney bleeding.
NSAIDs and analgesics
Most NSAIDs tend to interfere with platelet function. They interfere with platelet adhesion and aggregation (platelets become unable to join to form a clot). Data exist to show that two anti-inflammatory drugs, choline-magnesium-trisalicylate (Tri-lisate) and salsalate (Disalcid), do not alter platelet function and may therefore be useful for use in individuals with bleeding disorders. These medications are often useful for managing pain associated with ovulation and menstruation. A new class of NSAIDs, Cox-2 inhibitors (Celebrex), do not cause platelet dysfunction and may be useful for people with bleeding problems.
Surgical issues
Intrauterine ablation
In women who do not respond to other treatments, the uterine lining may need to be removed to prevent menstruation, although this will render it sterile. This may serve as a safe alternative to hysterectomy for bleeding problems. There is scientific evidence in the literature supporting the safety and effectiveness of this procedure for women with a range of bleeding problems.
Hysterotomy
For some women who are minimally responsive or completely resistant to other therapies, hysterotomy may be the only acceptable treatment. Vaginal or transabdominal hysterectomies have been safely performed in women with bleeding problems after adequate and appropriate plasma factor concentrations have been achieved.
Laparoscopy
In women experiencing pain due to endometriosis (bleeding from endometrial tissue growing outside the uterine cavity), removal of migrating tissue using a laparoscopic technique can be effective. In this procedure, two small incisions are made in the abdomen. A special probe for visual manipulation is guided by the surgeon through one of the incisions, while the tissue is removed through the second incision.
Dilatation and curettage of the uterine cavity
These procedures entail relaxing and sufficiently dilating the cervix and scraping the endometrium. The use of these procedures with the intention of reducing the intensity of bleeding cannot be effective for women with bleeding, since this technique prevents thrombus formation on damaged vessels of the subendometrial location. Also, if dilatation and curettage of the uterine cavity are not performed for diagnostic purposes, this is unacceptable in cases with patients with increased bleeding.
Ovariectomy
Ovariectomy (removal of the ovaries) may be an acceptable option for women who experience bleeding during ovulation and who, for one reason or another, cannot benefit from hormone therapy. However, this procedure not only makes the woman sterile, but also stimulates menopause. It is imperative that women considering any of these options fully understand the risks, benefits, and alternatives before making a definite decision.
Conclusion
I hope that this article will be useful for women and practitioners looking for answers to some of the questions that arise in patients with problems with increased bleeding. I also hope the article will raise many questions that the medical and scientific communities will try to find answers to. The time has come to join forces to solve these problems.
additional literature
1. "Females Bleed Too." HANDI Quarterly (Fall 1993).
2. "Symptomatic Carriers." HANDI Quarterly (Fall 1994).
3. Medical and Scientific Advisory Council "Recommendations Regarding Women With Bleeding Disorders." Medical Advisory #303 (1997), National Hemophilia Foundation.
4. Medical and Scientific Advisory Council “Treatment of von Willebrand Disease.” Medical Advisory #314 (1998), National Hemophilia Foundation
5. Bottini, E., et al. “Prevention of Hemoperitoneum during Ovulation by Oral Contraceptives in Women with Type III von Willebrand Disease and Afibrinogenemia. Case Reports." Haemoatologica 76 (1991): 431-33.
6. Brenner, P.F., Ed., “Management of Bleeding Disorders in Women, The Role of the Obstetrician/Gynecologist.” American Journal of Obstetrics and Gynecology. (1996): Suppl. 175(3) Part 2. 761-792.
7. Bunschoten, EP, et al. "Bleeding Symptoms in Carriers of Hemophilia A and B." Thrombosis and Hemostasis (Germany) 59, no. 3 (1988): 349-352.
8. Caldwell, David, et. al. "Hereditary Coagulopothies in Pregnancy." Clinical Obstetrics and Gynecology 28, no. 1 (March 1985).
9. Conti, M., et al. "Pregnancy in Women with Different Types of von Willebrand Disease." Obstetrics and Gynecology 68 (1986): 282.
10. Cohen, S., et al. "Epidural Analgesia for Labor and Delivery in a Patient with von Willebrand Disease." Regional Anesthesia 14 (1989): 95-97.
11. Ewenstein, B. “von Willebrand's Disease.” Annual Reviews in Medicine 48 (1997): 525-42
12. Kouides, P “Females with von Willebrand disease: 72 years as the silent majority.” Haemophilia 4 (1998): 665-676
13. Lee, CA "Women and von Willebrand disease." Haemophilia 5 (1999): Suppl. 2. 38-45
14. Murray E. and Lilicrap, D. “von Willebrand Disease: Pathogenesis, Classification, and Management.” Transfusion Medicine Reviews Vol. X, no 2 (1996): 93-110
15. Paper, R., Baker J and Larson K. “Women Can Have Bleeding Disorders.” Slide presentation. National Hemophilia Foundation. 1999
16. Robertson, L. E., et al. "Hereditary Factor VII Deficiency in Pregnancy: Peripartum Treatment with Factor VII Concentrate." American Journal of Hematology 40 (1992): 38-41.
17. Scott, J. P., and R. Montgomery. "Therapy of von Willebrand Disease." Seminars in Thrombosis and Hemostasis 19, no. 1 (1993).
18. Vosburgh, E. “Rational Intervention in von Willebrand Disease.” Hospital Practice (March 1993).
Prevention of heavy menstruation (menorrhagia, hypermenorrhea)
To prevent menorrhagia, medical doctors recommend, first of all, to refrain from extra-heavy physical activity (including sports), and also to be careful when choosing a diet. If you want to lose weight with its help, it is best to create a menu and diet with the help of a qualified specialist and consult with him periodically. In cases where a woman’s well-being noticeably worsens, it is worth resuming a normal diet and consulting a doctor.
In addition, the prevention of heavy and prolonged menstruation can be done by taking vitamin complexes containing vitamins C, group B, iron and folic acid. In this case, however, it is important to take into account the woman’s general physical condition, age, and predisposition to any diseases. The wrong choice of vitamin preparations, as well as their irregular intake, can cause a negative reaction in the body, so before using them it is recommended to consult a doctor and even undergo special tests.
Women who notice an increase in the volume of menstrual flow can also be advised to rest more and avoid excessive nervous tension and stress. Keeping a menstrual calendar will help determine the moment when painful disorders appear and simplify the process of diagnosis and treatment.
Calculate the cost
To learn more about the treatment of menorrhagia, fill out the form or call. Experienced specialists will answer all your questions, prescribe the necessary tests and draw up a treatment program for the disease.
Heavy menstruation after childbirth
A common cause of heavy uterine bleeding is also the recovery process after childbirth, in which case it is normal. Menstruation should begin within 6-8 weeks for a non-breastfeeding woman and at the end of breastfeeding or earlier for women who choose natural feeding.
The nature and course of menstruation after childbirth depend on the individual characteristics of the young mother (nutrition during pregnancy, rest regimen, psychological situation, etc.). Normally, menstruation lasts 5-9 days; during the period of greatest intensity, blood loss is 50-70 ml. After giving birth, a woman should be observed by a doctor and be sure to inform him when her period begins. If menorrhagia is diagnosed, the gynecologist will prescribe treatment appropriate for the lactation period.
Treatment of heavy menstruation should be carried out exclusively by a specialist; do not self-medicate - this can lead to serious complications of hypermenorrhea.