Every woman after a certain age faces a natural and irreversible process - menopause. But this new period of life is sometimes overshadowed by the complications of menopause: pain, increased sweating and nervousness, weight gain, depression and bleeding. Why do such problems arise and, most importantly, how to treat them, how to deal with them? Let's figure it out.
Bleeding during menopause: what is it?
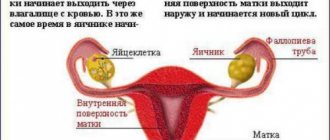
During menopause, women often experience bleeding, which can vary in intensity, abundance, pain and consequences. Bleeding during this period is any spotting that should alert the patient. They are not normal and require consultation with a doctor. For many women, menopause is a time when they forget about themselves, intimate life, and visits to the gynecologist. And the appearance of such discharge is a “bell” that should prompt the fair sex to take care of her health.
Menopause has 3 stages: premenopause (menstruation can still sometimes “happen”), menopause itself (when the last “critical days” begin) and postmenopause (the period that occurs after the last menstruation). In all these stages, the appearance of bloody discharge is quite possible. But bleeding during menopause must be treated adequately, clearly selected by a doctor. There is no need to solve this problem yourself. Even if the bleeding was one-time, you still need to be examined.
Prevention of DMK
In order to avoid pathology at an early stage, prevention must begin during the development of the fetus in the womb. Next, you need to monitor the health and condition of the immune system in childhood and adolescence. It is especially important to prevent abortions and acute diseases of the reproductive system.
But following all the specialist’s recommendations does not always lead to the desired result. When intrauterine bleeding occurs, all efforts must be directed toward restoring the menstrual cycle and preventing exacerbations in the future. For this purpose, experts use the following treatment regimen:
- During the first three cycles, oral contraceptives are taken (from 5 to 25 days).
- During cycles 4, 5, 6, medications are taken from 15 to 25 days.
- Progestin agents are taken from 15 to 25 days of the cycle for no more than 5-6 months.
Fact: oral contraceptives reduce the number of abortions and disruptions in the hormonal system, and also eliminate the development of breast cancer and other serious diseases.
Classification of bleeding during menopause
Bleeding during menopause is different and can be divided into types. This:
- Organic. Such bleeding is associated with diseases of the kidneys, liver, reproductive and circulatory systems.
- Iatrogenic. Such bleeding occurs due to the fact that the patient is taking some medications.
- Uterine bleeding of a dysfunctional type. They are due to the fact that there is an imbalance in the functioning of the reproductive system, problems with hormones.
You can also distinguish the following uterine bleeding during menopause:
- Menorrhagia - such bleeding is characterized by a duration of more than 7 days and a large amount of discharge. Bloody discharge occurs according to a specific cycle. The woman already knows when to expect them.
- Metrorrhagia. Bleeding of this type is characterized by a small volume of blood, but occurs spontaneously.
- Menometrorrhagia. Such discharges appear without cyclicity, at any time, but they have a large volume of discharge.
- Polymenorrhea. This is discharge that cannot be considered menstruation, but at the same time appears with a certain cyclicity. Usually their interval is 21 days, but no more.
In any case, treatment for bleeding during menopause should be prescribed exclusively by a doctor after a thorough examination. Regardless of what type of bleeding is present, this condition cannot go unnoticed.
Our services
The administration of CELT JSC regularly updates the price list posted on the clinic’s website. However, in order to avoid possible misunderstandings, we ask you to clarify the cost of services by phone: +7
| Service name | Price in rubles |
| Appointment with an obstetrician-gynecologist with ultrasound examination (primary) | 4 200 |
| Taking gynecological smears | 700 |
| Hysteroscopy (diagnostic, therapeutic) | 47 500 |
All services
Make an appointment through the application or by calling +7 +7 We work every day:
- Monday—Friday: 8.00—20.00
- Saturday: 8.00–18.00
- Sunday is a day off
The nearest metro and MCC stations to the clinic:
- Highway of Enthusiasts or Perovo
- Partisan
- Enthusiast Highway
Driving directions
Why does spotting occur during menopause?
There can be many reasons for bleeding during menopause. Some of them are quite harmless, but there are others that indicate a serious illness. As a rule, a woman cannot figure this out on her own, as this requires a detailed consultation with a doctor. But treatment of uterine bleeding during menopause is required almost constantly, and how it will proceed depends on the reasons.
The causes of bleeding during menopause can be:
- Hormonal disorders.
- Taking certain medications, including hormonal and contraceptive medications.
- Early onset of menstruation, absence of labor or a large difference between them, refusal to breastfeed.
- Heredity.
- Uterine fibroids.
- Uterine cancer.
- Ovarian dysfunction.
- Endometriosis.
- Endometrial hyperplasia.
- Polyps that are on the endometrium.
- Vaginitis
- Tumors, ovarian cysts.
- Ovarian cancer.
- Cervical cancer.
What symptoms are typical for bleeding?
Treatment of bleeding during menopause is a process that requires a careful study of the symptoms of the disease. The main sign of pathology is the presence of bloody discharge. They can be very abundant, and sometimes quite scanty; often such bleeding resembles a “daub”, in which the discharge of blood is insignificant. Sometimes they contain mucus. The color can also be different: from bright scarlet to dark brown. But regardless of this, even a small amount of blood should be considered bleeding. It also happens that the blood changes color from red to black. All these symptoms are extremely dangerous and can indicate the presence of infections, tumors and various problems.
Particularly dangerous symptoms of bleeding are considered to be fever, dizziness, pale skin, cold sweat, a prolonged period of discharge, sharp pain in the lower abdomen, a feeling of heaviness and “fullness” of the space in the lower abdomen. The worst and most dangerous symptom is sudden, heavy bleeding, in which the blood is bright scarlet, not thick, but rather liquid. In this case, the bleeding does not stop and increases, and there is a sharp, throbbing pain in the abdomen. Such conditions require emergency hospitalization and can even lead to the death of the patient.
How to diagnose pathology?
Menopausal bleeding requires careful diagnosis using the most modern methods. Only they can accurately establish the diagnosis, the cause, and only then can treatment be prescribed. First of all, you will need a detailed medical history, in which the doctor will find out the symptoms, history of the onset of menstruation, childbirth, abortion, surgery and other manipulations. The doctor may also ask about breastfeeding and the presence of gynecological diseases in close relatives. A thorough gynecological examination is required, during which smears are taken from the vagina. Based on initial examinations, the following diagnostic procedures can be prescribed:
- Testing for a hormonal panel, blood testing and blood clotting.
- Additional studies of the liver, kidneys, and thyroid gland.
- Testing for tumor markers, liver tests.
- A vaginal or transvaginal ultrasound is performed.
- A biopsy is performed and biological material is examined to detect cancer.
- An MRI of the pelvic organs is performed
Depending on the results of the study, additional examination procedures may be prescribed. Sometimes the diagnosis of uterine bleeding requires consultation not only with a gynecologist, but also with an endocrinologist, mammologist, oncologist, therapist, and hematologist. If a woman has a number of concomitant diseases, then this problem must be solved comprehensively, using all available specialists.
Methods for examining patients with uterine bleeding
Women who visit a medical facility due to menopausal bleeding are advised to undergo a thorough examination. What to do if the uterus starts to bleed? For severe bleeding, diagnosis and treatment are carried out simultaneously. In other circumstances, especially in old age, the source of metrorrhagia is first established, and then the cause of the blood loss.
Diagnosis of uterine menopausal bleeding is a set of measures, including:
- physical examination by a gynecologist and collection of information with the compilation of menograms (menstruation schedule) and its analysis;
- hormone test: determination of the level of estrogen, progesterone, LH, FSH, 17-ketosteroids, β-hCG;
- General and biochemical blood test, urine test;
- study of blood clotting, assessment of liver function;
- Ultrasound of the pelvic organs;
- tumor marker study;
- dilatation and curettage: curettage of the cervical canal and uterine cavity;
- oncocytological studies of materials taken by vacuum aspiration of the contents of the uterine cavity and a smear from the cervix;
- puncture of the posterior vaginal fornix;
- GHA - X-ray diagnosis of uterine diseases and tubal pathologies;
- hysteroscopy.
The number of measures prescribed as part of the examination for abnormal bleeding depends on the results of the examination by the gynecologist and the patient’s condition. Some diagnostic methods are carried out only in hospital settings.
After receiving the data from the above diagnostics, doctors establish an accurate diagnosis and prescribe appropriate therapy.
How to stop bleeding during menopause?
Treatment of uterine bleeding during menopause depends on the cause. Abnormal uterine bleeding during menopause can be one that requires immediate intervention, or it can be one that requires inpatient or outpatient treatment with conservative methods. If the bleeding is profuse, the abdominal pain is severe, and the woman feels extremely unwell, an ambulance should be called. Next, you need to lie down and put something cold on your stomach. You should not take any medications yourself or try to use traditional methods to stop bleeding.
If abnormal uterine bleeding during menopause is systematic, but does not pose a clear immediate threat to the patient’s life, it requires treatment. It can be conservative or surgical. It all depends on the reasons. If the problem is hormonal, drug treatment is used to stabilize it. If the cause is uterine fibroids, then resection of this organ can be performed. This means that the uterus will be removed. Sometimes the method of ultrasonic abalization is used, in which the fibroids are removed from the uterus. Uterine artery embolization is sometimes used. In this case, the tumor is deprived of blood supply and disappears.
Hyperplasia is treated with laser radiation, liquid nitrogen, and electric current. For endometriosis and polyps, curettage is often used, which stops bleeding and allows material to be taken for examination.
If adenomyosis occurs, then resection of the damaged areas or the uterus is performed.
If there are malignant tumors, they are usually removed along with the organs on which they originated.
Perimenopause is defined as "the period surrounding menopause, characterized by various physiological signs such as hot flashes and menstrual irregularities"
. Perimenopause can also be viewed from the perspective that it is a mirror image of adolescence, which is the beginning of the reproductive period, while perimenopause accompanies its end. The period of perimenopause can vary greatly depending on the age of onset, duration and pattern of bleeding [1].
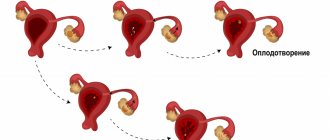
Regular menstrual cycles are due to the normal secretion of sex steroid hormones, the presence of ovulation and the production of progesterone in the luteal phase. The definition of abnormal uterine bleeding (AUB) is “bleeding outside of normal volume, duration, regularity, or frequency” [2]. Among patients who visit a gynecologist, 1/3 consult about AUB, of which more than 70% are women in the peri- and postmenopausal period [3]. A thorough examination of patients is important for two main reasons: 1) exclusion of severe pathology, such as cancer or complex atypical hyperplasia; 2) determining the cause of bleeding in order to initiate appropriate treatment (which in some cases may be watchful waiting). The classification of the causes of AUB is shown in the figure.
FIGO classification of abnormal uterine bleeding [4].
Diagnosis in women with abnormal uterine bleeding
The term AMB is an umbrella term that covers heavy menstrual bleeding (HMB, formerly called menorrhagia) and intermenstrual bleeding (IMB, formerly called metrorrhagia). The purpose of diagnosis is a sample of women whose AUB is caused by anatomical pathology of the reproductive system (endometrial cancer or hyperplasia, polyps, leiomyomas), and women with normal anatomy in whom AUB can be caused by ovulatory dysfunction, adenomyosis without endometrial abnormalities and is least likely coagulopathic and iatrogenic reasons. A common reason for peri- and postmenopausal women to see a doctor is breakthrough bleeding during menopausal hormone therapy.
As in all medical practice, the diagnosis of AUB begins with a thorough history and physical examination, followed by appropriate laboratory tests and the use of instrumental methods. Diagnosis of abnormal uterine bleeding.
Overall rating:
— anamnesis and assessment of the nature of bleeding;
- physical examination, pelvic examination and speculum examination.
Laboratory tests:
— clinical blood test, biochemical analysis (iron content), β-hCG (human chorionic gonadotropin);
- hormonal examination (FSH, LH, anti-Mullerian hormone, estradiol, progesterone), thyroid hormones and prolactin (as indicated);
- concentration of tumor markers (CA125, HE4, ROMA) in ovarian tumors;
- cytological examination of cervical smears (PAP smear);
- study of the blood coagulation system.
Transvaginal ultrasound (ultrasound) of the pelvic organs: measuring the size of the uterus and ovaries, endometrial thickness:
— color Doppler mapping (according to indications);
- sonohysterography;
Magnetic resonance imaging of the pelvic organs (if indicated).
Special studies:
— office endometrial biopsy and histological examination;
— pipell biopsy of the endometrium and histological examination;
- hysteroscopy and separate diagnostic curettage of the endometrium and endocervix with histological examination of the material.
The history should include a family history, taking into account the main disorders of the hemostatic system, the use of drugs or herbal preparations that can provoke bleeding, for example, contraceptives, menopausal hormone therapy (MHT), non-steroidal anti-inflammatory drugs (NSAIDs), warfarin, heparin and their derivatives, ginseng , gingko, motherwort [5, 6]. Physical examination findings include symptoms suggestive of anemia (exertional shortness of breath, dizziness), respiratory rate, heart rate, blood pressure, body mass index, skin examination (pallor, bruising, stretch marks, petechiae), and thyroid examination. Gynecological examination: examination using speculum to differentiate bleeding from the vagina or cervix, bimanual examination of the pelvic organs, including the size and contours of the uterus and its appendages.
Laboratory evaluation should include a complete blood count and iron test, as well as a test to look for hemostatic abnormalities if they are suspected or indicated. Pregnancy tests and thyroid screening may also be indicated.
Although many women may not be sure how often or how long they bleed, a thorough history of bleeding patterns, frequency, and severity is critical to making a diagnosis. For example, cyclic MMCs without MMCs are unlikely to be due to carcinoma or even hyperplasia. The most common cause of irregular bleeding is anovulatory uterine bleeding. Most often, anovulatory bleeding is not associated with anatomical abnormalities. A study of 443 women, which used transvaginal ultrasound and sonohysterography with isotonic sodium chloride infusion (SIF) as a first step in diagnosis, reported that 79% of women aged 35 years and before menopause with AUB were free of anatomical abnormality [7] . Most women with AUB experience dilation of the cavity and an increase in the size of the uterus due to childbirth, the presence of leiomyoma without submucosal growth, or adenomyosis without endometrial abnormalities. Patients with anovulatory bleeding most often have endometrial pathology, and therefore, at the first stage of diagnosis, a thorough assessment of the condition of the endometrium is of great importance in order to identify groups with focal or widespread pathological processes. Historically, dilatation of the cervical canal and curettage of the walls of the uterine cavity were the main method of diagnosing the condition of the endometrium. In fact, it was the most common surgical procedure for women for most of the 20th century. Dilatation and separate diagnostic curettage (DDC) is no longer the standard for initial endometrial evaluation. This is a blind procedure with a high risk of complications.
Disadvantages of blind endometrial biopsy
After the publication of the study by T. Stovall et al. [8] Blind endometrial biopsy using disposable suction piston devices has become the standard approach in patients with AUB. T. Stovall performed outpatient biopsies on 40 patients with carcinoma one week before hysterectomy. Endometrial carcinoma was confirmed in 39 out of 40 samples, indicating an accuracy of 97.5%, and therefore blind endometrial biopsy quickly became the gold standard. In a similar study, R. Guido et al. [9] performed blind endometrial biopsies on 65 patients with carcinoma in the operating room immediately before hysterectomy. In 11 of 65, malignant tumors were missed (sensitivity of only 83%), but after surgery the authors reported that in cases where the cancer occupied more than 50% of the endometrial surface, the accuracy of the biopsy was 100%. Similar studies have been carried out by other authors. In women with pre-diagnosed carcinoma, the sensitivity of blind biopsy was only 84% [10, 11], resulting in false-negative results of 16 and 32%, respectively. These studies were conducted using blind biopsies in women with confirmed carcinoma. To understand why these biopsies are ineffective for non-advanced pathology, it is enough to familiarize yourself with the prehysterectomy study by M. Rodriguez et al. [12], in which the biopsy device covered an average of 4% of the endometrial surface area (range 0–12%).
In 2012, the American College of Obstetricians and Gynecologists (ACOG) in its Practice Bulletin [2] recognized that “the primary role of endometrial biopsy in patients with AUB is to diagnose carcinoma or preneoplastic changes.” It is also indicated that endometrial biopsy has “high overall accuracy in diagnosing endometrial cancer, provided that the material obtained is adequate and the process is widespread in the endometrium. However, if the cancer covers less than 50% of the endometrial surface area, a blind endometrial biopsy may miss it. Thus, this method has a limit in detecting cancer or complex hyperplasia.” Of course, medical professionals, especially in poorly resourced settings, may begin the diagnosis with a blind biopsy, but if the results do not reveal cancer or atypical hyperplasia, then the assessment is inadequate, especially if bleeding persists. Thus, the concept of distinguishing between “common” and “focal” forms of the disease is becoming increasingly clear and important. This has enormous implications for clinical practice.
Visualization methods
The main method of uterine imaging to evaluate AUB is transvaginal ultrasound. However, it is not possible to perform an adequate ultrasound in all cases, for example, in cases of concomitant fibroids, previous surgery, significant obesity or adenomyosis. In such cases, another alternative is SIF (infusion of a liquid or gel into the uterine cavity to further define the anatomy of the uterine cavity). When using SIF, one can almost always distinguish between the presence or absence of actual anatomical pathology and focal abnormalities. Office hysteroscopy can be used as an outpatient diagnostic method, although it is more expensive and sometimes requires anesthesia [3].
Transvaginal ultrasonography
The vaginal probe provides the same degree of image magnification as using ultrasound with a low-power microscope, and its use can be considered a form of sonomicroscopy [13]. With the help of a vaginal probe, you can see features that are not visible to the naked eye. Early observational and subsequent large multicenter studies mainly from Western Europe clearly confirmed that in postmenopausal women with bleeding, thin, distinct endometrium (M-echo) indicates the absence of excess tissue and has a higher negative predictive value for endometrial cancer than blind endometrial biopsy [13]. This led the ACAG to change its opinion in February 2009 and state that if endometrial thickness is 4 mm or less on transvaginal ultrasound, endometrial biopsy is not required [14].
Data collected on perimenopausal women with AUB are limited. In perimenopausal women, cyclical changes in the endometrium persist due to the remaining unstable synthesis of estrogen by the ovaries during perimenopause. Therefore, the use of transvaginal ultrasound in such patients should be timed towards the end of the bleeding episode, when the M-echo will be thin. As discussed earlier, it is not possible to perform adequate ultrasound in all cases. In a study of 433 perimenopausal women aged 37–54 years, 10.2% required sonohysterography because non-contrast transvaginal ultrasound at the end of the bleeding cycle was not sufficient to effectively characterize and measure endometrial thickness [15]. ]; 64.7% of patients had an endometrial thickness of 5 mm or less, while 25.1% had an endometrial thickness of more than 5 mm and thus underwent SIF to distinguish between widespread and focal changes. The final diagnosis of the entire cohort revealed that 79% of patients had dysfunctional anovulatory bleeding, 13% had polyps, 3.5% had hyperplasia, and 5.3% had submucosal fibroids (although 33% had sonographic evidence of fibroids, only 5.3% of them were submucosal).
Hysteroscopy and separate curettage of the walls of the uterine cavity and endocervix are certainly the “gold standard” for the diagnosis and treatment of AUB. Like any invasive method, hysteroscopy requires great surgical skill and the ability to comply with all the necessary rules for its implementation. Even with high information content, hysteroscopy cannot replace morphological diagnosis; the final diagnosis is established by histological examination of the biopsy specimen.
Thus, diagnostic evaluation is of paramount importance for successful treatment and will have important implications for the selection of treatment options, particularly surgical, medical, or expectant management.
Treatment of patients with bleeding in perimenopause
Treatment should always be aimed at stopping bleeding and preventing relapse. After pregnancy and malignancy have been excluded, patients with anovulatory dysfunction, adenomyosis and endometrial hyperplasia (in the absence of anatomical abnormalities of the uterus and its appendages) taking contraceptives or MHT are treated in various ways. The goal of treatment for patients with AUB is to regulate menstrual cycles, minimize blood loss, prevent worsening anemia, and improve quality of life.
Treatment for heavy menstrual bleeding is aimed at preventing the anemia from getting worse and reducing the need for blood transfusions. For many non-anaemic patients, bleeding is more of a “quality of life” issue than a medical problem. Thus, for patients with dysfunctional anovulatory bleeding, it is important to be confident that there is no serious problem and understand that this is a normal situation during the transition from reproductive to perimenopausal life.
Control of abnormal uterine bleeding should include the following drug and non-drug measures:
- non-hormonal medications;
- NSAIDs;
- antifibrinolytic agents;
- combined oral contraceptives;
- cyclic or prolonged progestogen regimens;
- analogues of gonadotropin-releasing hormone (GnRH) (in the presence of fibroids);
- selective progesterone receptor modulators (in the presence of fibroids);
— intrauterine system with levonorgestrel (IUD-LNG);
- hysteroscopy and separate diagnostic curettage of the walls of the uterine cavity and endocervix;
— ablation or hysteroresectoscopy of the endometrium;
— embolization of the uterine arteries (in the presence of fibroids);
- hysterectomy.
Pharmacological (hormonal) therapy for AUB
According to a recent survey of ACHA members, the first-line treatment for patients with AUB in the United States is combined oral contraceptives (COCs). IUD-LNG has become the next most widely used option [16]. COCs regulate menstrual irregularities resulting from oligomenorrhea or anovulation and make menstruation more predictable. They can also reduce heavy menstrual bleeding in most patients and are considered a reasonable option for the initial control of MCH. COCs are less effective for the treatment of TMK in women with organic pathology. Menstrual blood loss is reduced by approximately 50% in women using COCs, and the reduction is most obvious during the first two days of menstruation. Long-acting or continuous COC regimens are associated with a significant reduction in bleeding compared with cyclic COC dosing. Reducing the hormone-free interval from 7 to 4 days significantly reduces the number of days of withdrawal bleeding in each cycle and increases the percentage of amenorrhea.
Many patients who are already taking COCs experience what we call “breakthrough bleeding.” Usually, adjusting the dose or type of tablets reduces their frequency, but continued bleeding of this nature should be a reason for further diagnosis of concomitant organic pathology.
For those patients who have contraindications to estrogen therapy, progesterone or LNG IUD therapy may be an alternative. Due to the antiproliferative effect of levonorgestrel on the endometrium, the duration of menstrual bleeding and blood loss are reduced. This effect begins during the first menstrual cycle after insertion of the device, and bleeding gradually becomes less heavy over time. Patients should be aware of the possibility of breakthrough bleeding, which occurs in the first months of treatment. Amenorrhea occurs in approximately 30-40 and 20-80% of cases in the first 12 months after installation of a progestin-containing contraceptive implant and LNG IUD, respectively [17]. The use of depot medroxyprogesterone acetate results in relatively high rates of dose-dependent amenorrhea (approximately 90% in some studies) and has traditionally been widely used for menstrual suppression.
Non-steroidal anti-inflammatory drugs - prostaglandin synthetase inhibitors
NSAIDs reduce the synthesis of prostaglandins. Prostaglandins may play a role in aberrant neovascularization leading to uterine bleeding. Oral NSAIDs are a means to reduce TMB. Compared with placebo, they reduce cramping menstrual pain and menstrual blood loss by 25–33% [18]. There were no significant differences in the effectiveness of reducing TMB when using different NSAIDs. Mefenamic acid 500 mg three times daily for 5 days and ibuprofen 600 mg every 6 hours or 800 mg every 8 hours are usually prescribed during the first 3 days of the menstrual cycle to reduce blood loss and menstrual cramps.
Tranexamic acid is a fibrinolysis inhibitor
Tranexamic acid reversibly blocks the binding sites of lysine with plasminogen, preventing the interaction of plasmin and fibrin polymers, which leads to fibrin degradation, stabilization of clots and reduction of bleeding. Tranexamic acid compared with placebo leads to a significant reduction in blood loss - by 45-60%. It has been used for many years to reduce blood loss and the need for blood transfusions during and after surgical procedures. Its therapeutic effect is superior to placebo and leads to a significant reduction in idiopathic TMB [19]. Tranexamic acid does not affect the duration of bleeding or the relief of unscheduled bleeding. The US Food and Drug Administration (FDA) has approved the use of tranexamic acid at a dose of 1300 mg (2 tablets of 650 mg) 3 times a day orally for 5 days of each menstrual cycle [20]. The oral bioavailability of tranexamic acid is only about 35%, making frequent administration necessary. In all studies analyzed, the disadvantages of frequent use include decreased adherence to treatment in patients and an increased risk of adverse gastrointestinal reactions (most often nausea, vomiting and diarrhea) [20]. The drug is contraindicated in women with an increased risk of thromboembolism.
Drugs that reduce the permeability and fragility of blood vessels include etamsylate at a dose of 1-2 g/day. The drug reduces blood loss by less than 10% and is effective when used in combination with other hemostatic drugs.
Non-drug approaches to the treatment of AUB (endometrial ablation)
Endometrial ablation is a minimally invasive alternative for the treatment of TMB that is well suited to the needs of patients. It is usually used in patients who are refractory to medical treatment and who would like to avoid surgical treatment (hysterectomy). Although endometrial ablation is a less invasive surgical alternative to hysterectomy, it does not eliminate the risk of surgery. There is evidence that over the next four years, 38% of women who underwent ablation undergo hysterectomy [21]. Endometrial ablation should be considered an alternative to hysterectomy, especially in older women who have chosen to preserve the uterus, but not in women who would like to preserve fertility. The patient's age is an important predictor of treatment success. Unlike the original resectoscopic endometrial ablation, several new ablation devices have the advantage of being performed on an outpatient basis. Careful patient selection appears to be a key factor in reducing the risk of endometrial cancer after ablation. In a recent systematic review [22], which analyzed 22 cases of endometrial cancer after ablation, the time to diagnosis of endometrial cancer varied from 2 weeks to 10 years after endometrial ablation. Most patients had symptoms of persistent bleeding or pain after the procedure; 86% of patients have risk factors for developing endometrial cancer such as obesity, complex atypical endometrial hyperplasia, diabetes mellitus, arterial hypertension and postmenopause. Therefore, endometrial ablation should be performed in those peri- and postmenopausal women who are at low risk of developing endometrial cancer and who have normal endometrial histopathological characteristics as assessed prior to ablation.
Non-surgical treatment of patients with uterine fibroids
Uterine fibroids clinically manifest in 30-35% of women aged 35-40 years and are often associated with abnormal uterine bleeding. Although hysterectomy remains a common treatment option for older patients with uterine fibroids, other treatment options need to be discussed so that women can make informed choices.
The combination of clinical symptoms, the size and location of the fibroids, and the patient's desire to preserve fertility may influence the choice of treatment proposed and accepted by the patient. There are no medications that can completely cure a patient with uterine fibroids, but some are available to relieve symptoms. In premenopausal women, these treatments are used to alleviate symptoms before menopause.
Tranexamic acid and mefenamic acid
Tranexamic acid (discussed above) is used as first-line therapy for TMC and is often used in patients with small fibroids, despite little proven effectiveness [23]. However, it has been shown to be safe and effective in women with uterine fibroids compared to placebo.
Mefenamic acid is an NSAID that is widely used for dysmenorrhea, resulting in a modest reduction in BMB in women without fibroids, although it is less effective than tranexamic acid. Currently, there have been no studies demonstrating the benefits of NSAIDs in women with fibroids [18].
Levonorgestrel - releasing intrauterine system
IUD-LNG is used to treat patients with MCI [24, 25]. Studies in patients with fibroids have demonstrated relief from dysmenorrhea and a positive effect in reducing blood loss. The overall spontaneous expulsion rate of the LNG IUD is 9.6% over a 3-year period. Their frequency increases to 15.8% in the presence of uterine fibroids.
Gonadotropin-releasing hormone agonists
Gonadotropin-releasing hormone agonists can be used before surgery for fibroids because they reduce uterine volume and node size [26]. They also reduce the incidence of iron deficiency anemia and reduce intraoperative blood loss. If the size of the uterus is such that midline incision is planned, this can be avoided in many women through the use of GnRH agonists. However, some authors argue that these drugs make myomectomy difficult because they disrupt tissue planes, increase the risk of recurrence, and are associated with side effects in situations where they do not provide benefit or where cheaper alternative drugs with fewer side effects are available. The effectiveness of treatment for uterine fibroids with GnRH in perimenopause has been proven. Adjuvant therapy should be initiated concurrently with GnRHa treatment to reduce hypoestrogenic side effects such as vasomotor symptoms and loss of bone mineral density when used for more than 6 months in those who do not desire surgical treatment.
Selective progesterone receptor modulators
Ulipristal acetate (UPA) is currently the only selective progesterone receptor modulator (SPRM) available in some countries. UPA induces amenorrhea in 63.1% of women and controls menstrual bleeding in 91% at a dosage of 5 mg/day and in 71.3 and 92%, respectively, at a dosage of 10 mg/day, although irregular bleeding is common in patients with submucosal fibroids. UPA also has some effect on fibroid size, although to a lesser extent than GnRHa [27]. The potential long-term impact of UPA on the endometrium is being studied because of the unusual histologic pattern of benign “nonphysiologic” endometrial change that is observed in many women treated with UPA. This change is called PMSIE (progesterone modulator-associated change in the endometrium). Common side effects of selective progesterone receptor modulators include headaches, nasopharyngitis, abdominal pain, and hot flashes. The antiprogesterone properties of mifepristone have also been used to treat patients with fibroids and have been shown to be effective in reducing nodule size and improving quality of life only at low dosages.
Other treatments
Other treatments may also be used, although they are less effective against fibroids. Those that induce amenorrhea, such as oral contraceptives, norethisterone acetate, may be useful. Studies have also been conducted with aromatase inhibitors, although the side effects of the latter may reduce their long-term use for these indications.
Radiation therapy: uterine artery embolization
Uterine artery embolization (UAE), performed by a specially trained surgeon, is a minimally invasive treatment option for patients with uterine fibroids. The catheter is inserted through the femoral artery in the groin area under local anesthesia and guided to the uterine arteries under fluoroscopic guidance. The uterine artery is blocked on each side using an appropriate embolic agent. The goal of UAE is to completely infarct all fibroid tissue while sparing the uterus, ovaries, and surrounding pelvic structures.
UAE was initially used for massive obstetric hemorrhage. The procedure is also indicated for symptomatic fibroids and is an alternative to myomectomy, since it allows you to save the uterus during a short hospital stay. The most common problem associated with UAE is postoperative pain, which is usually treated with analgesics. The birth of submucosal necrotic fibroids, chronic vaginal discharge and the development of premature ovarian failure are less common consequences associated with UAE.
A recently published Cochrane review concluded that UAE is a safe and effective treatment for patients with fibroid-related menstrual disorders. Severe complications were rare. Since the effects on fertility and pregnancy are still unclear, this method is a good option for most perimenopausal women [28, 29]. UAE is also associated with some decline in ovarian function in women over 45 years of age, which may lead to menopause [30].
Surgical treatment (hysterectomy)
Hysterectomy is the standard surgical treatment for women who no longer plan to become pregnant. Although hysterectomy is a major surgical procedure for patients with uterine fibroids, it eliminates most symptoms, especially those associated with menstrual disorders, and has a high degree of success [31].
Myomectomy is a surgical procedure to remove a fibroid node and restore the structure of the uterus. It is used as a fertility-friendly option. Myomectomy may be associated with significant bleeding, risk of hysterectomy, prolonged postoperative recovery, postoperative adhesion formation, and fibroid recurrence [32, 33].
Myomectomy can be performed open, laparoscopically, or hysteroscopically, depending on the location of the fibroid node and the skill of the surgeon. In addition, it may depend on the size and number of fibroids that can be removed laparoscopically and skills, which are often only available in specialized units [34]. These restrictions also apply to vaginal myomectomy. Hysteroscopic myomectomy is most suitable for nodes with a diameter of less than 5 cm, if the majority of them are located in the uterine cavity [35, 36]. Submucosal or pedunculated nodes deform the endometrial cavity and may be covered with vessels that collapse, causing irregular bleeding. Nodules less than 5 cm in diameter can be removed hysteroscopically, and the procedure has now been facilitated by the development of new instruments that have improved the safety and performance of the procedure. If the diameter of the node is more than 5 cm, the intervention can be performed in two stages and/or with the previous use of drugs such as GnRHa or SPRM, which will reduce the size of the node.
Malignant and precancerous diseases
Although many benign gynecological diseases involve abnormal bleeding, it is also a common symptom of endometrial cancer, hyperplasia and, less commonly, vaginal or even vulvar cancer.
Endometrial polyps
Endometrial polyps are usually removed because their malignancy potential is uncertain and they can cause irregular bleeding. Removal is often performed under local anesthesia.
Treatment of patients with endometrial hyperplasia with low malignant potential
Observations of endometrial hyperplasia with low malignant potential, formerly called simple or complex hyperplasia without atypia, can be managed conservatively along with an appropriately timed repeat endometrial biopsy to assess regression. However, the most commonly used progestogens are administered either orally or intrauterine (IUD-LNG). A systematic review of progestogens in the treatment of patients with hyperplasia indicates that IUD-LNG is a highly effective treatment method for hyperplasia without atypia, with a high level of success and patient adherence to treatment [37, 38]. In some cases, such as relapses, hysteroresectoscopy or, less commonly, hysterectomy is indicated.
Treatment of patients with complex hyperplasia with endometrial atypia
Patients with atypical endometrial hyperplasia are usually treated with total hysterectomy and bilateral salpingo-oophorectomy. In some cases, especially when it is necessary to preserve fertility, high doses of progestogens are used.
Thus, abnormal uterine bleeding in perimenopausal patients is often encountered in the clinical practice of obstetricians and gynecologists. Fortunately, most cases of AUB are not associated with malignancy or common precancerous conditions, although these must be carefully excluded during the diagnostic workup. Most often, bleeding is mainly a concern and negatively affects the quality of life. All the advantages and disadvantages of various diagnostic procedures, as well as medical and surgical treatments, have been previously discussed, and once the appropriate diagnosis has been made, the most appropriate treatment for each individual patient should be successfully carried out.
Summarizing the above, we can consider it advisable to do the following.
1. In the absence of absolute indications for surgery for AUB, one should almost always begin with drug treatment.
2. Not all uterine bleeding while taking MHT requires treatment; Watchful waiting can be used after serious pathology has been ruled out.
3. Any therapeutic options must take into account the patient's wishes regarding fertility preservation and her social status.
4. Empirical treatment should be started if the results of diagnostic tests are still not available or if there are difficulties in making an accurate diagnosis.
5. Many therapeutic modalities produce similar results, so it is important to discuss the risks, benefits, and alternatives of available treatment options.
The author declares no conflict of interest.
*e-mail; https://orcid.org/0000-0003-4911-719Х
Complications of bleeding: what are they?
Heavy bleeding during menopause can have various complications. You should not perceive them as something insignificant and frivolous. Women during menopause often do not want to see a gynecologist and undergo treatment. They believe that if their periods stop, then their life and youth are over. But this is not so: even at this time you can live an active sex life, enjoy and be happy. Therefore, you need to undergo a gynecological examination twice a year. After all, bleeding can have consequences:
- They are life-threatening if they occur suddenly, are very abundant, and can lead to large blood loss.
- They can be a sign of malignant tumors, because if there is prolonged bleeding for no clear reason, then it could be cancer. And the sooner it is detected, the easier it is to cure. Otherwise, a woman may miss precious time and the opportunity to recover.
- If there are benign tumors (fibroids, cysts), no one can exclude the possibility that they will not develop into malignant ones. They need to be removed.
- Hormonal imbalance and constant bleeding will lead a woman to a state of constant stress, nervousness, and inability to have a sexual life.
- Constant bleeding negatively affects all organs and systems of a woman.
Uterine bleeding during menopause is a serious reason to think about your health.
Menopause is “autumn” in a woman’s life. And this period can be pleasant, eventful and easy. It should not be marred by bleeding. But in case of such trouble, you should not be afraid, but you should immediately consult a doctor.
Ways to stop bleeding from the uterus at home
Currently, patients are increasingly resorting to the use of traditional medicine recipes to eliminate various diseases, and uterine bleeding is no exception. However, it should be noted that such methods can only eliminate the consequences of uterine discharge and stop bleeding, without in any way affecting the causes of their occurrence.
Do not forget that regarding taking these medications, you must first consult with a gynecologist as a supplement.
As a rule, decoctions and infusions are especially popular. They may be based on nettle, viburnum bark, yarrow or horsetail. Before you begin self-medication, you should pay attention to the fact that this process can aggravate the situation and provoke complications, although these components may well stop the bleeding that occurs.
Thus, climatic uterine bleeding indicates the presence of a pathological process in a person, requiring immediate consultation with a specialist and further elimination.