General information
The prevalence of mycoses (fungal diseases) covers up to 20% of the population and increases with age.
At the age of 70, 50% of the population suffers from these diseases. There is a tendency towards an increase in fungal skin diseases in children. The increase in the incidence of mycoses is explained by the increased use of broad-spectrum antibiotics and the increase in the number of patients with immunodeficiency conditions. More than 500 species of fungi are known, but some of them affect the skin and its appendages (hair and nails), without affecting deep tissues. This group of pathogens causes superficial mycoses or dermatomycosis. Fungi, the causative agents of dermatomycosis (they are called dermatophytes), require nutrition with organic compounds, in this case it is keratin of human or animal tissues. Dermatophytes are highly contagious and are transmitted from person to person, from animals, or enter the skin from the environment. Superficial mycoses include mycoses of the feet , rubromycosis , inguinal dermatophytosis , trichophytosis , favus , microsporia .
For the introduction of the fungus into the skin and the development of a disease of any localization, the virulence and pathogenicity of the pathogen, as well as the state of the macroorganism, are important - this is a decrease in reactivity, age, vitamin deficiency , metabolic disorders and the presence of endocrine pathology. The condition of the skin is important - a factor that contributes to infection. The presence of cracks, abrasions, maceration, cuts, injuries caused by tight shoes.
Today we will look at two dermatomycosis - athlete's foot (it also has another name - fringed eczema), caused by the fungus Epidermophyton floccosum and athlete's foot, which is caused by Trichophyton mentagrophytes (this dermatophyte can parasitize both the feet and the area of large folds). Fungi of the genus Candida rarely lead to the development of the disease on their own; more often they are detected as a mixed infection with dermatophytes.
Of course, among dermatomycosis, mycoses of the feet and nails (onychomycosis) come first. In terms of prevalence among adults, they prevail over other infectious skin lesions. Dermatophytosis of the feet occurs 3 times more often than other localizations.
Much less attention is paid to mycoses affecting the folds, in particular the groin areas, although the prevalence of the disease is also significant. These two diseases should be considered together, since foci of infection on the legs play an important role in affecting the folds. This pattern is expressed mostly in men.
Symptoms: rash, burning and itching
Inguinal athlete's foot in men has pronounced clinical symptoms. Red, scaly spots appear in the groin folds or on the inner thighs. In the center they are almost no different from healthy skin, but at the edges they are red or red-pink. This is how the initial stage of the disease manifests itself.
Gradually the number of spots increases, they merge with each other. The meeting point of the spots is called the focus. It is in the foci that scales (which, falling off, are visualized as peeling), blisters and pustules are localized. All this causes burning and itching.
The contour of epidermophytosis is characterized by wavy edges (in dermatology they are called the beautiful word “scalloped”) and an elevation above healthy skin. In appearance, the roller-shaped outline resembles a red worm curled into a ring at the site of the pathology. In medicine, this symptom is called a more euphonious phrase - “cord symptom.”
Pathogenesis
Skin folds are places with high humidity and temperature, which creates conditions for dermatophytes. Dermatophytes that get into the folds do not cause manifestations of the disease if the barrier function of the skin, its acidity and the body's specific defense system are preserved.
A decrease in these protective factors and a change in the biocenosis of the skin contributes to the active proliferation of the fungus. The presence of damage to the stratum corneum causes increased permeability of the skin to pathogens. The causative agent of athlete's foot penetrates into the deep layers of the epidermis and dermis and causes characteristic rashes.
Dermatophytes have keratolytic and lipolytic effects. Their keratinase enzyme only breaks down human keratin. The growth and reproduction of fungi causes destruction of the stratum corneum of the skin. The process is characterized by progression, so inflammatory changes are most pronounced at the periphery of the lesions. If the rate of restoration of the epidermis is greater than the rate of reproduction of the fungus, then the pathogen is often eliminated and spontaneous recovery occurs.
Endogenous factors play an important role in the pathogenesis of dermatophytosis. Inguinal athlete's foot is often observed against the background of diseases such as diabetes mellitus , hepatitis , vegetative-vascular dystonia or in oncological pathology. Often, manifestations in the folds serve as “signal signs” of diabetes mellitus, since the bactericidal activity of the skin in patients with diabetes mellitus is lower than in healthy people. Also, mycoses of large folds often occur when taking systemic glucocorticosteroids for various concomitant diseases ( bronchial asthma , rheumatoid arthritis , lupus erythematosus ). A very severe course of epidermophytosis of the skin and folds is observed in HIV-infected individuals.
Causes
The causative agents of inguinal mycoses are Epidermophyton floccosum (35-40% of cases), Trichophytom rubrum (15-20% of cases), Trichophytom mentagrophytes var. interdigitale (20-25%). Candida and aspergillus (opportunistic fungi) are detected in association with the above. Thus, the cause of lesions in the groin area are various pathogens, which means that treatment requires antifungal drugs with a wide spectrum of activity.
Inguinal athlete's foot is promoted by increased air temperature, increased sweating and impaired carbohydrate metabolism. It is not surprising that this disease is more common in places with warm and humid climates. Infection occurs through contact with a patient, but more often through objects (thermometers, washcloths, underwear) used by the patient.
In the development of athlete's foot, contact with contaminated objects in the shower, sauna, swimming pool, living quarters, or wearing someone else's shoes and socks is important. Exfoliated epidermis in patients with epidermophytosis or particles of destroyed nails end up in the environment in public places, and then on the feet of a healthy person. Onychomycosis (damage to the nails) mainly develops due to autoinfection (from the patient himself), if there is a long-term fungal infection of the skin.
Predisposing factors for mycoses of the feet and inguinal folds are:
- foot hyperhidrosis;
- poor hygienic foot care;
- unfavorable social conditions;
- metabolic and endocrine disorders, primarily diabetes mellitus;
- high ambient temperature;
- injuries, diaper rash , abrasions;
- wearing tight shoes;
- reduced body resistance;
- long-term use of antibiotics, cytostatics or corticosteroids;
- ionizing radiation;
- chronic diseases accompanied by immunodeficiency (AIDS and others).
Epidemiology of athlete's foot
The fungus Epidermophyton floccosum is ubiquitous. Among all fungal diseases, athlete's foot accounts for no more than 1.2 - 1.8%. Men are more often affected, children - rarely; cases of mycosis in them are registered during puberty.
The contagiousness (infectiousness) of athlete's foot inguinal is quite high. Outbreaks have occurred in nursing homes, hospitals, schools and families. Infection occurs in saunas, baths, showers and restrooms, when using a shared bathroom, through washcloths, towels, sponges, underwear of a sick person, oilcloths, thermometers and bedpans, in gyms through equipment.
Contribute to the development of inguinal athlete's foot:
- increased sweating,
- obesity,
- wearing tight and warm (out of season) clothes,
- staying in a humid climate,
- long-term use of glucocorticoids.
- maceration of the skin,
- warming compresses.
Rice. 2. Fungus in a man’s groin.
Symptoms
The clinical picture of epidermophytosis of the folds is due to the destruction of the stratum corneum of the skin and a pronounced inflammatory reaction. If the pathogenicity of dermatophytes increases, the process worsens and the patient’s general condition deteriorates. Lesions are characterized by their ability to grow peripherally. This is due to the fact that the rate of reproduction of the pathogen outstrips the protective reaction of the epidermis in the form of proliferation and restoration.
Inguinal athlete's foot in men
In men, the inguinal folds are affected more often than in women. This sexual predisposition is explained by the peculiarities of the anatomy and physiology of the male body: a more pronounced function of the apocrine glands of the genital area, a different composition of the sweat secreted by them, and constant trauma to the thighs due to friction with the scrotum. The lesion of the folds is characterized by symmetry, so there is the possibility of a latent course of the process on the other side without clinical manifestations. To prevent relapse, prophylactic treatment is carried out on an externally unchanged inguinal fold.
There is also the possibility of a hidden course of mycosis of the scrotum - it is constantly affected, but the clinical signs are not expressed (mild erythema ). Dermatophytosis of the inguinal folds is more common in obese men with excessive sweating. In addition to damage to the inguinal folds, they may also be affected by the axillary folds and under the mammary glands.
The disease most often begins acutely and, if correct and timely treatment is not prescribed, it can become chronic. Typical localization is the skin of the inguinal folds and intergluteal folds. It is also possible for lesions to spread to the scrotum and penis. First, a swollen bright red lesion appears with flaky skin and a peripheral ridge.
Photos of inguinal athlete's foot in men
The formed lesion contains various elements: spots, papules, vesicles. The elements of the rash reflect the degree of allergic reaction to the fungus: from the least reaction - spots, and at the maximum - large quantities of vesicles, weeping and erosion.
Epidermophytosis is characterized by ring-shaped growth and expansion of the lesion. As the lesions grow, they merge and form garland-like shapes that spread far beyond the folds. This occurs because the fungus invades new areas of the skin and the lesion looks like an expanding ring. The patient is bothered by severe itching. Resolution processes may begin in the center of the lesion, while an acute process continues to occur at the periphery. Complete resolution of the spots does not occur, but over time the redness is replaced by a brown background.
The skin of the scrotum is affected in almost all patients and is characterized by slight redness. Athlete's foot is often complicated by secondary bacterial and candidal infections, especially if local corticosteroid ointments are used in cases of incorrect diagnosis. If treated incorrectly, the disease becomes chronic with relapses.
Inguinal athlete's foot in women
In women, the folds, inner thighs and lower abdomen are also affected. In women, damage to the intergluteal fold and buttocks is more common. Rashes in the form of outlined, slightly raised round spots of pinkish-brownish color, on the surface of which there is fine-plate peeling. Characteristic is the gradual growth of lesions and the merging of nearby ones, so they take on scalloped outlines. Papules are located along the periphery of the lesion. Itching, just like in men, is the main symptom. Over time, the central zone of the spot turns pale, and the peeling becomes almost invisible, the inflammation in the center decreases. This process does not affect the periphery - an inflammatory ridge (cord symptom) remains here.
Photos of inguinal athlete's foot in women
The pathogen can affect not only the inguinal folds, but also the folds under the breasts. Also in 19% of cases, the skin of the buttocks and torso is involved. In this case, the lesions occur with minimal symptoms: slight inflammation and peeling. They are often misdiagnosed as lichen (rosacea or pityriasis versicolor) and superficial trichophytosis .
Athlete's inguinal: photo of lesions of the buttock and gluteal fold
Without treatment, the disease is long-lasting, with periodic exacerbations, mainly in the summer. During an exacerbation due to sweating, small bubbles, crusts, and itching appear again on the surface of the lesion. Elements of the rash appear mainly on the periphery of the lesion. The same protracted, erased nature of the disease is caused by the use of corticosteroid ointments, which effectively eliminate inflammation but do not act on the pathogen. Complications occur 2 times more often in women than in men. Pyoderma predominates allergic dermatitis and fungal eczema in the background . Treatment of inguinal athlete's foot in women and men will be discussed below.
Athlete's foot
E. floccosum also affects the feet. This is a chronic fungal disease that affects the skin and very often the nails. Effective local therapy, when only the skin of the foot is affected, can prevent involvement of the nails. Damage to the nail plates occurs in a distal-lateral form, and the nail folds are not involved.
Athlete's foot occurs in various forms: squamous, intertriginous, dyshidrotic, squamous-hyperkeratotic, onychomycosis and acute form. Among the clinical forms, the leading one is intertriginous, affecting the folds between the third and fourth fingers. Squamous-hyperkeratotic is less common.
The squamous form is manifested by peeling of the skin (fine, pityriasis-like) on the arch of the foot, sole, and in the skin grooves. Sometimes peeling occurs against a background of redness. The process eventually spreads to the lateral surfaces of the fingers.
With the squamous-hyperkeratotic form, areas of skin thickening form on the feet, as with callus, and lamellar peeling appears on it.
The intertriginous form begins with peeling of the skin between the toes. Then diaper rash appears, vesicles open, a crack appears in the folds, surrounded by a peeled layer of the epidermis. Itching and sometimes burning occurs between the fingers.
With prolonged walking, the cracks deepen and form into erosion. When bacterial or yeast flora is attached, redness, swelling of the skin appears, pain appears and itching intensifies. The course of this form is chronic, with exacerbations observed in the summer.
With the dyshidrotic form, blisters with a dense covering appear on the arches of the foot, the lateral surface outside, along the edge of the sole, and between the toes. The bubbles are filled with transparent contents and look like “sago grains”. The bubbles are located in groups and often merge to form multi-chambered bubbles. After opening the blisters, erosions form with a roll of exfoliated epidermis. If pyococcal flora is added, the contents of the blisters become purulent. Patients may develop lymphangitis (inflammation of the lymphatic vessels) and lymphadenitis (enlargement of regional lymph nodes). This is accompanied by fever, pain and general malaise.
Photo of athlete's foot, dyshidrotic form
Dyshidrotic epidermophytosis of the hands and feet occurs There are rashes on the palms called epidermophytids. But damage to the hands is more typical for rubromycosis , since the causative agent Trichophyton rubrum is detected in the disease in 90% of cases.
The classic form is manifested by redness and dryness of the palms and soles, and floury peeling in the skin grooves. Rubromycosis of the feet occurs as epidermophytosis (squamous, dyshidrotic or intertriginous), but differs in that not only the sole, but also the dorsum of the foot is affected. Here plaques with nodules, scales, blisters, and crusts are identified. The same picture can be seen on the hands, but with less intensity. Rubrophytosis of the hands begins with damage to the palms and is combined with onychomycosis . Dry skin, thickening, and floury peeling are observed.
Lesions on the back of the hand appear later and are represented by nodules, blisters and crusts. Infection of the hands occurs from foci of rubrophytosis on the feet with lymphohematogenous spread of fungi. Acute epidermophytosis is an exacerbation of intertriginous and dyshidrotic forms. Against the background of pronounced swelling of the skin, abundant vesicular-bullous elements appear. Pyodermic complications, lymphadenitis , lymphangitis , and the temperature rises significantly.
Onychomycosis (damage to the nails) more often than the 1st, 4th and 5th toes occurs in 25% of cases. In men, damage to the nail plates occurs almost 2 times more often than in women. The affected nails thicken, and yellow-gray spots appear in the thickness of the plate, under which hyperkeratosis , the plate itself loosens and breaks. Loosening and fragility develop much more slowly than with rubromycosis of nails.
Diagnosis of mycosis of inguinal folds
Most cases of inguinal mycosis can be recognized by examination by a dermatologist. Additional examination may include:
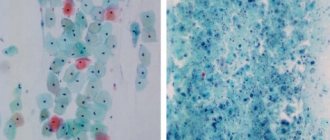
- scraping the skin from the affected area, treating it with potassium hydroxide and examining it under a microscope to identify fungal cells;
- placing a scraping sample on a nutrient medium so that fungal cells grow in large numbers, which will allow them to study their biochemical properties.
Sometimes inguinal mycosis is misdiagnosed. In this case, it occurs under the guise of other diseases, for example, eczema. Treatment of inguinal mycosis may not be effective enough. In this case, you may need to be examined by a dermatologist using a Wood's lamp or even a biopsy of the affected area.
Tests and diagnostics
- Microscopy of pathological material is used as a method of preliminary diagnosis.
- Isolation of a pathogen culture (growth of the pathogen in a culture) takes time.
- Polymerase chain reaction (PCR). It makes it possible to obtain results within 24 hours that are highly specific (90-98%). It is especially important for onychomycosis and atypical forms of dermatomycosis, since in the earliest stages it allows to prescribe rational therapy, reduce complications and the severity of lesions.
Procedures and operations
In advanced forms of onychomycosis and irreversible changes in the nail plate, the patient may be offered surgical removal of the nail plate, which is performed under local anesthesia. After surgery, an antibiotic and antifungal ointment is applied to the wound. The dressing is changed twice a day. The course of treatment with local antifungal agents continues until a healthy nail grows - this may take 6-9 months.
Laser removal of the nail plate is also used. The procedure is less painful and bloodless than conventional surgical nail removal, is characterized by rapid tissue restoration, and there is no deformation of the growing nail. If the nail plate is slightly affected, it is not completely removed using a laser. It is enough to destroy the mycelium and spores of the pathogen with laser exposure. With the help of a laser, this is possible because it penetrates 7-8 mm through the nail into the soft tissue. The course of treatment is 4-5 procedures, and after a month it is recommended to repeat the course of treatment.
Frequently asked questions about dermatophytosis inguinalis
How dangerous is dermatophytosis inguinalis?
If not treated promptly, dermatophytosis inguinalis can lead to the formation of lichenification. This is a thickening of the skin and a violation of pigmentation due to scratching due to severe itching. It is also possible that a secondary infection may occur, erosions, ulcers, and ulcers appear, and pain increases.
How long does it take to treat dermatophytosis inguinalis?
On average, the duration of treatment for inguinal dermatophytosis is 4–6 weeks.
Which doctor treats dermatophytosis inguinalis?
A dermatologist deals with diseases of the skin. Sometimes, for more effective treatment, a dermatologist refers patients to a mycologist and trichologist.
Prevention
It is important to observe the rules of personal hygiene:
- Wash your feet daily with cool water and laundry soap.
- Daily change of socks.
- Wear shoes according to the season, since excessively warm shoes can provoke athlete's foot .
- In public places (bathhouse, sauna, swimming pool) it is mandatory to use individual rubber shoes.
- Have for personal use a separate towel for legs and body and individual scissors.
- It is not permissible to use someone else's shoes in everyday life.
- Active treatment of sweating.
- Disinfection of shoes to prevent reinfection and relapse. To reduce the likelihood of relapse, you need to treat all the patient’s shoes with a formaldehyde solution.
- Timely treatment of a general disease that provokes skin pathology.
In public places:
- Carrying out frequent disinfection of floors, benches, decking, showers, swimming pools.
- Inspection of workers of baths, saunas and swimming pools to detect epidermophytosis.
- Regular examinations of those visiting the pools by a dermatologist.
Consequences and complications
When athlete's foot complications are considered:
- Transition from one form to another.
- Onychomycosis.
- The addition of a bacterial infection is secondary pyoderma , lymphangitis , lymphadenitis and recurrent erysipelas, resistant to antibiotic treatment. Against the background of such lesions, thrombophlebitis , lymphostasis and elephantiasis occur .
- Allergization of the body: urticaria , bronchial asthma , allergic rhinitis , the occurrence of mycids . These are secondary allergic rashes due to mycoses.
For inguinal athlete's foot:
- Mycotic eczema . It occurs in a chronic form, manifested by lichenification of the skin (thickening), which occurs from scratching. The process resembles neurodermatitis.
- Allergic dermatitis.
- Impetiginization is the development of impetigo as a complication of mycosis. Impetigo is a strepto-staphylococcal skin lesion.
Treatment
Medication method
There are 2 options for using antifungal drugs:
- external use at the site of pathology localization,
- oral medication.
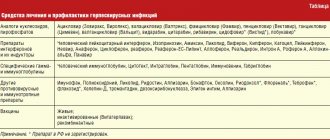
The question of how to treat inguinal epidermophytosis is decided based on concomitant diseases. Taking medications orally occurs when, in addition to mycosis in the groin area, there is a fungus on other parts of the body (on the nails, on the feet). Information about the drugs recommended in such cases is provided in the table.
Doctor's advice
The causes of a rash in the groin area can be very different: bacteria (for example, erythrasma), contact dermatitis (for example, on the material of clothing, underwear), eczema, and so on. Therefore, it is very important to see a doctor when a rash is detected in order to determine the true cause of the disease and quickly help the skin.
Inna Zhikhoreva Dermatologist, Venereologist, Hair diseases
| Notes on use | Terbinafine tablets (250 mg per tablet) | Itraconazole capsules (100 mg per capsule) |
| Daily intake of the drug | 1 tablet once after meals | 2 times 2 capsules |
| Duration of treatment | 2-4 weeks | 1 Week |
| Contraindications | vascular pathology of the extremities, metabolic disorders, the presence of tumors, liver failure | heart pathology (treated by a cardiologist) |
| special instructions | lack of improvement after 2 weeks is a reason to consult a doctor to confirm the correctness of the identified causative agent of the disease | use caution in case of renal pathology, peripheral neuropathy and liver disorders |
| Side effects | diarrhea, dizziness, abdominal pain | hair loss, heart failure, hypokalemia, diarrhea, dizziness, abdominal pain |
The drugs indicated in the table disrupt the cell membrane of fungi, which causes their death. It is important to avoid interruptions in taking medications. Otherwise, there is a surge in the disease.
If inguinal athlete's foot is not accompanied by other mycotic lesions on the body, treatment of the patient is limited to antifungal agents for external use.
The already mentioned Terbinafine is available not only in tablets, but also in the form of 1% ointment or cream. The active substance of the drug is good at destroying pathogens of mycoses, therefore it tops the list of drugs prescribed by dermatologists for the treatment of inguinal athlete's foot.
The affected area of the groin area is washed and dried. Twice a day, apply a thin layer of ointment (or cream) and rub in gently. The area of application is not limited to just the affected area; the medication is also applied beyond the “cord” by about 2-3 cm. Cure occurs in about a week.
In the line of antifungal drugs, another medication occupies an advantageous position - Termicon (generic Terbinafine).
The medicine is available in the form of a spray, thanks to which it:
- does not cause a greenhouse effect (unlike fat-based ointments);
- dries affected skin areas;
- not only fights fungal infection, but also has anti-inflammatory and antipruritic effects.
The method of using the spray is similar to using ointment and cream.
Treatment of inguinal athlete's foot (even advanced ones) does not involve large material costs. Each of the drugs mentioned is characterized by affordability. This thesis is confirmed by information from the table.
| Drug name | Release form | Price range (RUB) |
| Terbinafine | tablets (250 mg) | 200 – 300 |
| Terbinafine | ointment 1% (15 g) | 70 – 100 |
| Terbinafine | cream 1% (15 g) | 70 – 100 |
| Thermikon | spray (15 ml) | 200 – 300 |
| Itraconazole | capsules (100 mg) | 300 – 400 |
It is not difficult for an experienced dermatologist to identify the disease when examining a patient. However, given the self-medication often practiced by patients (the use of various ointments, the use of traditional methods, etc.), it would be more competent to conduct a cultural study of the scales. This is sowing on a special medium, which takes about a month. Unlike the conventional microscopic method, cultural analysis is more informative.
Inna Zhikhoreva
Dermatologist, Venereologist, Hair diseases
Athlete's inguinal athlete is not a cause for concern. It is easy to diagnose and just as easy to treat, which is why treatment occurs at home.
To get healthy men back on track faster, do not self-medicate. Thus, taking anti-inflammatory drugs (instead of antifungals) for inguinal athlete's foot relieves itching and some other obvious symptoms. At the same time, the causative agents of fungal infection are not destroyed, but lead a secretive lifestyle in order to expose themselves at the most inopportune moment.
This article has been verified by a current qualified physician, Inna Zhikhoreva, and can be considered a reliable source of information for site users.
Rate how helpful this article was
4.3 15 people voted, average rating 4.3
Did you like the article? Save it to your wall so you don’t lose it!
Forecast
Despite the fact that epidermophytosis is characterized by a long course and a tendency to recur, the prognosis is usually relatively favorable. If treatment is prescribed correctly, recovery occurs. At the same time, it is important to carefully observe the timing of treatment, observe the rules of personal hygiene and eliminate all risk factors, including adjusting sugar levels in diabetes mellitus .
Athlete's foot is characterized by a more persistent course, but with proper and long-term treatment, the prognosis for recovery is also favorable. When bacterial infections are associated, the prognosis of the disease is more serious. Onychomycosis can be treated, but it must be long-term and use systemic drugs. The effect in the treatment of onychomycosis depends not only on the prevalence of the process, the form of nail damage and the correct choice of means, but also on the disinfection of shoes until a healthy nail grows back.
List of sources
- Sergeev A. Yu., Sergeev Yu. V. Fungal infections (a guide for doctors). M., 2003. 185–193.
- Leshchenko V. M. Fungal skin diseases. In the book: Skin and venereal diseases (a guide for doctors). Ed. Yu. K. Skripkina, V. N. Mordovtseva. M., 1999. T. 1. P. 257–311.
- Sergeev V.Yu., Sergeev A.Yu. Dermatophytes: new in the diagnosis, therapy and prevention of the most common human mycoses. Consilium medicum. – Dermatology. – 2008. – No. 1. – P. 30–35.
- Haldin A.A., Sergeev V.Yu., Izyumova I.M. Modern ideas about inguinal dermatophytosis: etiology, epidemiology, clinical picture and effective therapy. Ross.zhur. leather and veins Bol. – 2005. – No. 5. – S. 43–48.