What is fibrous tissue?
Fibrous tissue is a type of connective tissue consisting primarily of collagen fibers and amorphous matter. It is produced by liver stellate cells, which are the main connective tissue cells in the liver and are activated during chronic inflammation.
Unlike connective tissue, fibrous tissue is rougher and more fibrous. It contains more collagen and amorphous intercellular substance. This tissue composition is unchanged and does not depend on the type of pathology developing in the liver.
Pathology of soft tissues of the shoulder and hip joints - diagnosis and treatment
Periarticular pathology is widespread and includes a huge range of changes from syndromes divided into separate nosological units to symptoms accompanying rheumatological diseases.
When describing soft tissue pathology, the following concepts are usually used:
- tendonitis - inflammation of tendon tissue;
- tenosynovitis/tenosynovitis - inflammation of the tendon tissue and tendon sheath;
- enthesitis/enthesopathy - inflammation of the tendon tissue at the site of its attachment to the bone;
- Bursitis is an inflammation of the bursae, thin-walled cavities lined with synovium that facilitate the movement of tendons and muscles over bony prominences.
Periarticular diseases of the shoulder joint are represented by several nosological forms:
1) isolated damage to the tendons of the muscles surrounding the joint:
- rotator cuff tendonitis (specifying the specific muscle);
- biceps tendinitis;
- calcific tendinitis;
- rupture (partial or complete) of the tendons of the muscles of the shoulder joint;
2) diffuse non-inflammatory damage to the capsule of the shoulder joint (retractile capsulitis);
3) subacromial syndrome (complex damage to the structures surrounding the subacromial bursa).
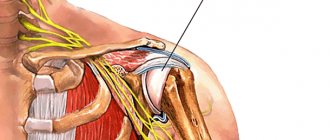
The spherical structure of the shoulder joint allows it to perform a variety of movements: flexion, extension, abduction, adduction and rotation. It should be remembered that the angle of movement in the shoulder joint without the participation of the scapula characterizes the true range of movements in it, and with their participation - the full range. When testing shoulder abduction, pain in the joint may only appear when it reaches 70–90°. In this case, the greater tubercle of the humerus rises close to the acromion process and can compress the structures passing here (the supraspinatus tendon and the subacromial bursa). As you continue to raise your arm, the greater tubercle moves away from the acromion process and the pain decreases significantly. This painful arch is characteristic of supraspinatus tendinitis or subacromial bursitis. The appearance of pain at the moment of maximum abduction of the arm in the shoulder joint (up to 160–180°) indicates damage to the acromioclavicular joint. With an anterior dislocation, there is a displacement of the head of the humerus anteriorly and downward, which leads to a characteristic change in the contours of the shoulder and a sharp limitation of mobility due to pain (Table 1).
For shoulder tendinitis, the following is recommended:
- avoid movements that cause pain for 2–3 weeks;
- prescribing non-steroidal anti-inflammatory drugs (NSAIDs) for the duration of severe pain and inflammation;
- local application of ointments and gels with NSAIDs 3 times a day for 14 days (in the acute period), as well as irritating ointments that increase blood flow (with capsaicin) - in the chronic course;
- periarticular administration of glucocorticoids (GC) (avoid in case of biceps tendinitis);
- physiotherapeutic methods: phonophoresis, electrophoresis, cryotherapy, magnetic currents, balneotherapy.
Treatment for calcific rotator cuff tendinitis follows the same principles as for normal tendinitis. However, calcific tendinitis is rarely cured completely and often recurs. There is evidence of the effectiveness in a number of cases of extracorporeal shock wave therapy in relation to both the pain syndrome and the calcifications themselves.
Retractile capsulitis should be considered as one of the variants of the syndrome of reflex sympathetic dystrophy (isolated or as part of the “shoulder-hand” syndrome), which differs from tendinitis in the absence of a degenerative component in the pathogenesis, diffuse damage to the capsule of the shoulder joint, manifested by fibrosis, involvement of bone structures in the form of regional osteoporosis.
Treatment of retractile capsulitis is aimed at physical rehabilitation with restoration of the original range of motion in the shoulder joint, and follows the principles of treatment of reflex sympathetic dystrophy.
Subacromial syndrome (subacromial collision syndrome) develops as a result of an imbalance between the muscles - stabilizers and depressors of the head of the humerus (supraspinatus, infraspinatus, subscapularis and biceps brachii), which leads to a decrease in the space between the head of the humerus and the acromion, to chronic injury to the tendons of the rotator cuff muscles shoulder cuffs during movements.
There are stages of subacromial syndrome.
I. Swelling and hemorrhages in the tendons. II. Fibrosis, thickening of the tendons, the appearance of partial tears in them. III. Complete tendon ruptures, degenerative bone changes involving the inferior surface of the acromion and the greater tubercle of the humerus.
Treatment of subacromial syndrome depends on the severity of clinical manifestations and the stage of the process. In stage I - avoid raising the arm above the head, trial therapy with full doses of NSAIDs for two weeks, subacromial administration of glucocorticosteroids (GCS) (repeated injection no earlier than after 6 weeks), physiotherapeutic treatment in the presence of weakness of the muscles of the shoulder girdle (after 1-2 weeks). At stage II - drug treatment (see above), if ineffective within a year - subacromial decompression (intersection of the coracoacromial ligament with anterior acromionoplasty), at stage III - arthroscopic revision of the subacromial space, removal of osteophytes, restoration of tendon integrity.
Damage to the periarticular tissues of the hip joint
The hip joint is a large ball-and-socket joint that has a significant range of motion: flexion/extension, abduction/adduction, pronation/supination. The mobility of the hip joint is determined by the elongated neck of the femur, which forms an angle of 130° with the axis of the limb. The most common causes of pain in the hip joints are injuries, arthritis (osteoarthritis (OA), rheumatoid arthritis), aseptic necrosis of the femoral head, osteochondritis dissecans (Perthes disease), infections (for example, osteomyelitis, tuberculous coxitis). However, pathology of the soft tissues surrounding the joint is also common (Table 2).
The most difficult diagnostic situation arises when the patient complains of pain in the hip joint, but no changes are detected during X-ray examination. In these cases it matters:
- well-collected medical history;
- physical examination: a combination of pain with extreme abduction and internal rotation suggests arthritis or osteonecrosis; restriction of movements in the direct projection in patients with diabetes mellitus will allow one to suspect adhesive capsulitis;
- the presence of general signs such as weakness, fever, weight loss or increased pain at night requires special laboratory testing to exclude a tumor or hidden infectious processes.
The most common cause of pain is bursitis in the area of the greater trochanters, which is characterized by:
- the pain is deep, sometimes burning, mainly along the lateral surface of the joint and thigh. The pain increases when walking on a flat surface and stairs, squatting, and is combined with lameness in 15% of patients;
- pain decreases with rest, but can periodically intensify at night, especially when lying on the sore side;
- upon palpation, tension is noted in the area of the greater trochanter;
- resistance is felt when the hip is abducted while the patient is lying down in the opposite direction, and a feeling of discomfort may occur.
Treatment of periarticular pathology of the hip joint area should take into account the underlying disease (for example, OA - the prescription of “chondroprotective” drugs, body weight control; seronegative spondyloarthritis - the prescription of disease-modifying drugs (sulfasalazine, methotrexate, etc.), tuberculous coxitis - specific anti-tuberculosis drugs, etc. .d.). Often the main methods of treatment are local administration of GC, electrophoresis and iontophoresis, and the administration of muscle relaxants.
One of the main directions in the treatment of periarticular soft tissue pathology is the prescription of various forms of NSAIDs. The anti-inflammatory and analgesic activity of NSAIDs is associated with a decrease in the production of prostaglandins. The anti-inflammatory effect of NSAIDs is due to the suppression of the activity of cyclooxygenase (COX), the main enzyme in the metabolism of arachidonic acid on the path of its conversion into prostaglandins. The mechanisms of action of NSAIDs are quite well studied, and the main side effects of this group of drugs are also described, limiting their use in patients at risk. An alternative to oral and parenteral use of NSAIDs, as well as an important auxiliary component of the complex treatment of pain syndrome in periarticular pathology, is local therapy with NSAIDs. Currently, the basic requirements for local therapy have been formulated: the drug must be highly effective, must not cause local toxic and allergic reactions, and also have the ability to penetrate the skin, reaching the target tissue; the concentration of drugs in the blood serum should not reach a level leading to side effects. The most successful form for local therapy is the use of a gel, in which alcohol as a solvent ensures rapid absorption of the active substance into the superficial structures of the joint. Therefore, the use of gel is justified compared to ointments or creams and is more economical. All these requirements are met by Deep Relief - a two-component gel for external use based on ibuprofen 5.0% and menthol 3.0% of natural origin, in which the analgesic and anti-inflammatory effects of ibuprofen are complemented and enhanced by the therapeutic properties of levomenthol (optical isomer of menthol) due to the reflex reaction associated with irritation of the nerve endings of the skin, stimulation of nociceptors. Thanks to the components of the gel base, ibuprofen molecules in a bound state penetrate the surface layer of the skin. Menthol causes the release of vasodilating peptides, which leads to additional distracting, analgesic effects, causing a feeling of slight coolness. To enhance the local anti-inflammatory effect, the product should be applied multiple times throughout the day. Clinical studies in recent years have shown that the minimum is 4 times the application of a local product during the day. In case of active inflammation with the most severe pain, the application of the drug should be increased to 6 times a day.
Literature
- William J. Koopman (editor) et al. Arthritis and Allied Conditioins: A Textbook of Rheumatology, 13th edition. Williams & Wilkins, 1997.
- Hakim A., Clunie G., Hag I. Oxford Handbook of Rheumatology, 2nd edition. Oxford University Press, 2008. 606 p.
- John H. Klippel. Primer on the Rheumatic Diseases, 12th edition. In: Leslie J. Grofford, John H. Stone, Cornelia M. Weyand. Atlanta, Georgia, 2001.
- R. Watts et al. Oxford Desk Reference: Rheumatology. Oxford University Press, 2009.
N. A. Shostak, Doctor of Medical Sciences, Professor N. G. Pravdyuk, Candidate of Medical Sciences A. A. Klimenko, Candidate of Medical Sciences, Associate Professor
GBOU VPO RNIMU im. N. I. Pirogova Ministry of Health and Social Development, Moscow
Contact information for authors for correspondence
Causes of fibrosis
Fibrosis is a complication of chronic processes occurring both in the liver itself and in other organs. All causes can be divided into two large groups - congenital and acquired.
The most common acquired causes are alcoholic liver disease, viral and toxic hepatitis, non-alcoholic fatty liver disease, and cirrhosis.
Hereditary causes are congenital pathologies such as Wilson-Konovalov disease, alpha-1-antitrypsin deficiency, hemochromatosis and galactosemia.
Diagnosis of fibrosis
The doctor may suspect a pathological process in the liver based on the patient’s complaints, as well as data from visual examination, palpation and percussion. Only instrumental diagnostic methods in combination with or without laboratory tests can confirm the presence of fibrosis:
- elastography (“fibroscan”) – allows you to determine the elasticity of tissue;
- biopsy – collection of material for histology and cytology, which will help confirm the presence of fibrosis and identify its cause;
- highly specific biochemical blood tests - fibrotest, fibrospect II, fibromax, fibrometer V.
Such diagnostics may be required to clarify the cause of fibrosis, its form and the severity of the process. This will allow you to choose the most effective treatment methods.
Fibrous dysplasia. Types and therapy of the disease
Fibrous dysplasia is a systemic disease of bone tissue, which mainly affects the skeletal system of women and is diagnosed at a late age, although the first manifestations of the disease are possible in children. Dysplasia refers to diseases that give rise to cancer, although it is not cancer initially, but only transforms into it over time if no effort is made to eliminate it. In inaction, it turns into a state of a benign tumor and then requires completely different treatment. The causes of dysplasia have not been established, although there are assumptions about a hereditary predisposition, but this has not been confirmed by research.
Types of fibrous dysplasia
There are two forms of pathology: when one bone is affected - the monoosseous form, the second option is the polyostotic form - damage to two or more bones. In the first case, the disease can develop in different age categories, even in elderly people. Massive bone damage mainly occurs in childhood, or even in utero, and disrupts the functioning of the internal organs of the body, especially the endocrine glands. It is characterized by excessive pigmentation (melanosis) and cardiac abnormalities.
The course of the disease can be acute or in remission. Exacerbations can occur several times a year.
There are several types of fibrous dysplasia, namely:
- Intraosseous. It manifests itself in the form of the appearance of one or several foci of fibrous tissue inside the bone with partial or complete replacement. But since the bone shell remains intact, it does not lead to deformation.
- Total or polyostotic. In this case, the entire structure and all bone elements are affected, causing deformation and frequent fractures.
- Albright's syndrome. It is characterized by complete damage to bone tissue with damage to internal organs, which at an early age leads to dysfunction of puberty, skin pigmentation and deformation of not only an individual bone, but also the entire body, for example. The form can originate in the form of postural disorders, such as spinal scoliosis
, kyphosis. - Fibrous-cartilaginous. It affects cartilage and muscles, and leads to their transformation, often preceding the appearance of a tumor.
- Tumor-like. Very rare. Appears due to the proliferation of fibrous tissue in large quantities.
- Calcifying. A special form of dysplasia is most often diagnosed on the tibia. It is extremely rare.
Depending on where the source of the disease is located, it can manifest itself differently, but have common signs for its detection. The course and severity of the form depend on the type of dysplasia, which affects treatment and manifestation.
Main features
Fibrous dysplasia has main symptoms such as skeletal deformity and pain. Very often it is not possible to detect a disease before it manifests itself. Pathological fractures are one of the first messengers signaling disorders in the skeletal system, and it is when diagnosing a fracture that this disease can already be detected.
With focal damage, the following areas of the bone are usually affected:
- ulna;
- radial;
- shoulder;
- tibial;
- femoral
The bones of the head, shoulder blades, ribs and spine may also be affected. Due to the heaviness of the body, the legs most often suffer, especially the thigh, which manifests itself in the form of deformities, shortening of the length of the legs and, as a result, lameness and pain when walking.
If the fibula is affected, no deformation is observed, but if the tibia is affected, then deformation of the tibia occurs, as well as its shortening. Dysplasia of the ischium has a destructive effect on the spine, and if foci of fibrous dysplasia are added to it, then the curvature process becomes too pronounced.
The focal form occurs without pronounced symptoms, without causing harm to other internal organs.
Symptoms:
- frequent fractures;
- pain;
- bad feeling;
- lameness;
- external changes (shortened fingers, legs, legs).
With total damage, signs of the disease make themselves felt at an early age. Basically, at the initial stage, everything is asymptomatic.
Diagnostics
The variety of symptoms makes it difficult to accurately determine the type of diagnostics to make a diagnosis. Therefore, the disease is usually determined by chance, during an examination, perhaps for some other reason, for example, a broken leg, or a bone deformity, or simply feeling unwell. However, when pathology is detected, a more accurate diagnosis helps to make:
- radiography;
- CT (computed tomography);
- appointment with specialized specialists (therapist, endocrinologist, orthopedic surgeon).
Treatment and prevention
Fibrous dysplasia develops in the prenatal state, so it cannot be treated. In addition, it is not clear what causes the pathology; some cases cannot be explained at all. It is possible to perform surgical removal at the source of formation in some cases, but this may not have significant results, or it may only stop the development of the disease for some time. Therefore, orthopedic treatment is carried out quite often in order to reduce the manifestation of pathology. Surgical treatment is carried out according to doctor's indications in special cases. These include:
- Fractures that are life-threatening.
- Rapid progression.
- Cysts.
- Pain that is not relieved by medication.
In children, radical treatment is used, with resection of the entire pathology focus and replacement with an implant.
Subsequently, growth is corrected with medication by stimulating osteoblasts. Preventive measures have not been identified, since the etiology of this disease is not clear. Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr