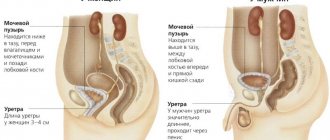
The urethra is the duct that connects the bladder to the outside. The male urethra is about 20 cm long, connecting the bladder to the head of the penis. When men urinate, urine leaves the bladder through the urethra, and seminal fluid is also released during sexual intercourse. Urethritis - inflammation of the urethra - is one of the most common reasons why men should visit a urologist or dermatovenerologist.
Causes of urethritis - infectious pathogens
Urethritis is usually caused by an infection, although this is not always the case. Infectious urethritis is usually transmitted through sexual contact.
Male urethritis is divided into:
- gonococcal urethritis caused by Neisseria gonorrhoeae;
- non-gonococcal urethritis caused by non-gonorrheal infection;
- persistent or recurrent urethritis, the multifactorial causes of which often cannot be identified.
Infectious pathogens of urethritis
Non-gonococcal urethritis is caused by:
- Chlamydia trachomatis (40%);
- Ureaplasma urealyticum (10-20%);
- Mycoplasma genitalium (10-20%);
- Trichomona vaginalis (1-17%).
Other causes of infection are less common:
- urinary tract infection (less than 6%);
- adenovirus (2-4%);
- herpes simplex virus (2-3%).
Adenovirus or herpes simplex virus are more associated with oral sex.
Sometimes urethritis is caused by: Candida spp., Haemophilus spp., Neisseria meningitidis, E. coli infection, Bacteroides infection.
Non-infectious causes:
- trauma, for example, during catheterization;
- irritation of urethral structures, for example from soaps, spermicidal creams and deodorants.
Other causes of inflammation include:
- lichen sclerosus, Stevens-Johnson syndrome, Reiter's syndrome, reactive arthritis;
- foreign bodies in the urethra;
- in about 20% of cases there is no obvious cause.
Anatomy of the male genitourinary system
Anatomy of the male genitourinary system
Human upper urinary tract
Lower urinary tract and male genital organs
Bladder
The bladder is an organ of the human urinary system. The bladder is located in the pelvis behind the bones of the womb, above the prostate, and in front of the rectum. Part of the upper and posterior walls of the bladder is covered by the parietal peritoneum. The following parts are anatomically distinguished in the bladder:
- Bubble Bottom
- Bladder walls (front, side, back)
- Bladder neck
The right and left ureters approach the posteroinferior surface of the bladder. The neck of the bladder continues into the urethra (urethra). When full, the bladder may protrude above the pubis. In this condition, the bladder can be felt with your hands in the lower abdomen directly above the pubis in the form of a round formation, when pressed, the urge to urinate occurs. The bladder capacity is usually 200–400 ml. The inner surface of the bladder is covered with mucous membrane. The main functions of the bladder are:
- In the accumulation and retention of urine (continuously flowing from the kidneys through the ureters)
- In urine output
The accumulation of urine in the bladder occurs due to the adaptation of the bladder walls to the volume of incoming urine (relaxation and stretching of the walls without a significant increase in intravesical pressure). With a certain degree of stretching of the walls of the bladder, the urge to urinate is felt. A healthy adult can hold urine despite the urge to urinate. Containment of urine inside the bladder is carried out using a sphincter apparatus (valves) that compress the lumen of the bladder neck and urethra. There are two main sphincters of the bladder: the first is involuntary (consists of smooth muscle fibers), located in the urinary neck at the outlet to the urethra, the second is voluntary (consists of striated muscle fibers), located in the middle part of the pelvic urethra and is part of the pelvic floor muscles. During the act of urination, which normally in an adult is carried out voluntarily at will, both sphincters relax and the walls of the bladder contract, which leads to the expulsion of urine. Impaired functioning of the muscles that expel urine and sphincters leads to various urinary disorders. Frequent diseases of the bladder are infectious inflammation of the mucous membrane (cystitis), stones, tumors and disorders of the nervous regulation of its functions.
Corpus cavernosum
The corpus cavernosum is a structural part of the penis. The corpora cavernosa (right and left) are cylindrical in shape and located inside the penis. To the ventral surface of the cavernous bodies, parallel to them, is the spongy (spongiosum) body of the penis. Anatomically, the corpus cavernosum is divided into:
- Top (apex) - distal part
- Middle part
- Pedicel - proximal part
In the apical part, the cavernous bodies are covered by the glans penis, which is part of the corpus spongiosum. At the symphysis pubis in the proximal part, the cavernous bodies diverge downward and posteriorly parallel to the descending (ischial) branches of the pubic bones, to which they are attached by ligaments. In the area of the symphysis pubis, the corpus cavernosum is attached to the bones using the unpaired infundibular ligament. The corpora cavernosa can be felt as ridges on the right and left inside the penis. The main function of the corpora cavernosa is to ensure erection of the penis (increase in size and hardening of the penis during sexual arousal). The corpus cavernosum consists of cavernous tissue surrounded by a tunica albuginea. Cavernous tissue has a cellular structure. Each cavity (cell) has the ability to change its internal volume by changing the tone of the smooth muscle elements (trabecular muscles) included in the structure of the cavern walls. Blood enters the caverns through arterioles radiating from the cavernous artery, located centrally inside the corpus cavernosum. During sexual arousal, in response to the release of a mediator (NO - nitric oxide), due to the relaxation of the trabecular muscles and the muscles of the walls of the cavernous arteries, the lumen of the cavernous arteries and the volume of the caverns increase. Increased blood flow to the cavernous tissue and filling of the caverns with a larger volume of blood leads to an increase in the total volume of cavernous tissue (tumescence or swelling of the penis). Normally, the outflow of blood from the cavernous tissue occurs through the venous plexuses located directly under the tunica albuginea. When the venous plexuses are pressed to the tunica albuginea due to an increase in the volume of cavernous tissue during tumescence (the basis of the veno-occlusive mechanism), the outflow of blood from the cavernous bodies decreases, leading to the appearance of a hard erection. At the end of sexual activity (usually after ejaculation), the release of norepinephrine, a sympathetic transmitter that increases the tone of the trabecular muscles, leads to the disappearance of an erection (detumescence) in the reverse order to the appearance of an erection. Insufficient blood flow to the cavernous bodies, excessive outflow of venous blood from the cavernous bodies, damage to the nerves that conduct signals for the appearance of an erection, as well as damage to the cavernous tissue leads to a deterioration in the quality of sperm and erection, up to its complete absence (impotence). The tunica albuginea of the corpus cavernosum is the case of the cavernous bodies and consists of elastic connective tissue. During an erection, the tunica albuginea, evenly stretching in different directions, ensures a symmetrical enlargement of the penis. Congenital disorders of the elasticity of the tunica albuginea, scar changes after injuries to the penis and the formation of fibrous plaques on the tunica albuginea in Peyronie's disease can lead to curvature of the penis during erection.
Kidneys
The kidneys are the main and most important paired organ of the human urinary system. The kidneys are bean-shaped, measure 10–12 x 4–5 cm and are located in the retroperitoneum on the sides of the spine. The right kidney is bisected by the line of the right 12th rib, while 1/3 of the left kidney is above the line of the left 12th rib, and 2/3 is below (i.e., the right kidney is located slightly lower than the left). During inhalation and when a person moves from a horizontal to a vertical position, the kidneys shift downward by 3–5 cm. Fixation of the kidneys in a normal position is ensured by the ligamentous apparatus and the supporting effect of the perinephric tissue. The lower pole of the kidneys can be felt with your hands while inhaling in the right and left hypochondrium. The main functions of the kidneys are:
- In the regulation of the water-salt balance of the body (maintaining the necessary salt concentrations and fluid volume in the body)
- To remove unnecessary and harmful (toxic) substances from the body
- In blood pressure regulation
The kidney, filtering the blood, produces urine, which is collected in the cavity system and discharged through the ureters into the bladder and further out. Normally, all the blood circulating in the body passes through the kidneys in about 3 minutes. Per minute, 70–100 ml of primary urine is filtered in the renal glomeruli, which is subsequently concentrated in the renal tubules, and per day an adult ultimately excretes an average of 1–1.5 liters of urine (300–500 ml less than he drank) . The renal cavity system consists of calyces and pelvis. There are three main groups of renal calyces: upper, middle and lower. The main groups of calyces unite to form the renal pelvis, which then continues into the ureter. The movement of urine is ensured by peristaltic (rhythmic wave-like) contractions of the muscle fibers of the walls of the renal cups and pelvis. The inner surface of the renal cavity system is lined with mucous membrane (transitional epithelium). Violation of the outflow of urine from the kidney (stone or narrowing of the ureter, vesicoureteral reflux, ureterocele) leads to increased pressure and expansion of the abdominal system. Long-term disruption of the outflow of urine from the renal cavity system can cause damage to its tissue and serious impairment of its function. The most common kidney diseases are: bacterial inflammation of the kidney (pyelonephritis), urolithiasis, tumors of the kidney and renal pelvis, congenital and acquired abnormalities of the kidney structure, leading to impaired outflow of urine from the kidney (hydrocalicosis, hydronephrosis). Other kidney diseases include glomerulonephritis, polycystic disease and amyloidosis. Many kidney diseases can lead to high blood pressure. The most severe complication of kidney disease is renal failure, which requires the use of an artificial kidney device or a donor kidney transplant.
Prostate
The prostate gland (prostate) is one of the organs of the male reproductive system. The prostate has the shape of a chestnut, is located in the male pelvis downward from the bladder, posterior to the bones of the pubis, anterior to the rectum and covers the initial sections of the urethra on four sides. The seminal vesicles are located on the posterior surface of the prostate. The posterior surface of the prostate can be felt with a finger through the anterior wall of the rectum. The prostate, being a gland, produces its own secretion, which enters the lumen of the urethra through the excretory ducts. The main functions of the prostate are:
- In the production of part of the seminal fluid (about 30% of the ejaculate volume)
- Participating in the mechanism of sperm release during sexual intercourse
- Participating in the mechanisms of urinary continence
The prostate has no direct relation to the mechanism of the appearance of penile erection and disturbances in its quality.
five anatomical and physiological in the prostate :
- Anterior fibromuscular
- Peripheral
- Central
- Transient (transitional)
- Periurethral
From a clinical point of view, the transient and peripheral zones are of greatest importance. With age, the transition zone usually increases in size. As the size of the transition zone increases, mechanical compression of the urethra can occur, leading to disruption of the outflow of urine from the bladder. An increase in the transitory zone and associated urinary disorders are called adenoma or benign prostatic hyperplasia, which is present in approximately 50% of men aged 50 years and, accordingly, 90% of men aged 80 years. The importance of the peripheral zone lies in the fact that about 80% of all prostate cancers develop there. Every sixth to seventh man over 50 has a chance of getting prostate cancer, and this chance increases with age. Another common prostate disease that disrupts a man’s quality of life is prostatitis or inflammation of the prostate.
Testicles
Testicles (testes) are male reproductive glands. The testicles (right and left) are located in the corresponding halves of the scrotum in a man. The spermatic cords, consisting of the testicular membranes, testicular artery, veins of the testicular venous plexus and the vas deferens, approach the upper pole of each testicle. Along the lateral surfaces of the testicles, from the upper to the lower poles, there are epididymis, which at the lower pole of the testicle continue into the vas deferens. The testicles can be felt with your hands through the skin of the scrotum in the form of round formations of elastic consistency. The epididymis is palpated in the form of ridges on the lateral surface of the testicles. Main functions of the testicles :
- Production of male sex hormone (testosterone)
- Production of sperm (male reproductive cells necessary for the fertilization process)
Main functions of the epididymis :
- Carries sperm from the testis into the vas deferens
- Carrying out the process of sperm maturation.
Anatomically, the testicle has parenchyma (the testicular tissue itself) and a dense and elastic tunica albuginea surrounding the parenchyma. The bulk of the testicular parenchyma consists of many convoluted microscopic tubules lined with spermatogenic epithelium, consisting of Sertoli cells, on which sperm formation and maturation occurs. The tubules gather towards the upper pole of the testis (a network of straight tubules), where they become the epididymal tubules. Moving along the tubules of the epididymis, the sperm mature, after which they enter the vas deferens and then through the ejaculatory canals out through the urethra during ejaculation. Between the tubules in the testicular parenchyma there are Leydig cells that produce the main male sex hormone - testosterone. Regulation of the concentration of testosterone in the blood is carried out by the hypothalamus and pituitary gland - structures of the brain, due to more or less release of luteinizing hormone, which in turn stimulates Leydig cells to release testosterone. Lack of testosterone secretion can be caused either by poor functioning of Leydig cells due to testicular damage (congenital, traumatic or inflammatory changes), or by insufficient secretion of luteinizing hormone by the pituitary gland. Lack of testosterone leads to infertility, decreased libido and sometimes causes erectile dysfunction.
The testicle, initially developing in the abdominal cavity of the fetus, gradually moves downward during intrauterine development and by the time of birth (or immediately after it) descends into the scrotal cavity. The need to move the testicles from the abdominal cavity to the scrotum is due to the fact that the process of sperm formation requires a lower temperature than body temperature. Normally, the temperature in the scrotum is 2–4° C lower than body temperature. The movement of the testicle into the scrotum leads to some peculiarities in the blood supply and the structure of the membranes. When passing from the abdominal cavity through the inguinal canal, the testicle carries with it the muscles of the anterior abdominal wall and the peritoneum, thus acquiring the muscular and vaginal membranes. The vessels supplying the testicle (artery and veins) originate in the upper floors of the abdomen (on the right side - from the aorta and inferior vena cava, on the left side - from the renal arteries and veins) and repeat the path of passage of the testicle into the scrotum in the retroperitoneal space and inguinal channels. Violation of the outflow through the testicular veins (occurs more often on the left) leads to the appearance of varicocele (varicose veins of the spermatic cord), which is a common cause of male infertility. The presence of a muscular membrane (creamaster muscle or levator testis muscle) leads to the possibility of pulling the testicle to the outer ring of the inguinal canal. In a vertical position, when you run your finger over the skin along the inner surface of the thigh, the testicle begins to rise upward (creamasteric reflex). The entrainment of the parietal (parietal) peritoneum by the testicle during the intrauterine movement of the testicle into the scrotum leads to the formation of a vaginal process (protrusion) of the peritoneum, which by the time of birth overgrows along the spermatic cord, forming a closed serous cavity near the testicle. Non-closure of the vaginal process of the peritoneum leads to the appearance of a congenital inguinal hernia or hydrocele of the testicle communicating with the abdominal cavity. The accumulation of fluid in a closed cavity inside the tunica vaginalis of the testicle leads to the formation of true hydrocele (hydrocele). Failure of the testicle to descend into the scrotum (cryptorchidism) or failure of the testicle to progress further into the abdomen or inguinal canal often results in significant damage to all testicular function (infertility) and is a risk factor for the development of testicular cancer. Penetration of infection into the epididymis from the urethra through the vas deferens often leads to the development of epididymitis (inflammation of the epididymis). In sexually active men under the age of 30, acute epididymitis in 65% of cases is associated with chlamydial infection acquired through sexual contact. Inflammation of the epididymis can lead to male infertility due to blockage of the tubules. In addition to inflammation, a common disease of the epididymis is spermatocele (epididymal cyst). One of the acute diseases of the testicle is its torsion, a condition requiring emergency care. This disease is similar to inflammation of the testicle and its epididymis (orchiepididymitis), but in the absence of timely help it can lead to testicular necrosis. It occurs more often before the age of 20.
Ureters
The ureters are part of the human urinary system. The ureters (right and left) begin at the renal pelvis, pass in the retroperitoneal space on the sides of the spinal column, crossing the transverse processes of the lumbar vertebrae approximately in the middle, descend into the pelvic cavity, run along the posteroinferior surface of the bladder and, passing through the wall, open with mouths in its cavity. It is impossible to palpate the ureters through the abdomen and lower back. The ureters are ducts 27–30 cm long, 5–7 mm in diameter, having a wall with a muscular layer and lined with mucous membrane (transitional epithelium) on the inner surface. The main function of the ureters is to conduct urine from the kidneys to the bladder. Conduction of urine is carried out due to involuntary peristaltic (rhythmic wave-like) contractions of the muscular lining of the walls of the ureters. Every 15–20 seconds, urine alternately flows from the ureters into the bladder cavity in portions. Each ureter has mechanisms that prevent the backflow (reflux) of urine from the bladder cavity when intravesical pressure increases (including when the bladder contracts during urination). With urine reflux, the function of the ureter and kidney can be impaired. Each ureter has 3 physiological constrictions located at the point of origin from the renal pelvis; at the border of their middle and lower thirds at the intersection with the iliac vessels; at the site of passage inside the wall of the bladder. The presence of narrowing of the ureters is important in case of urolithiasis, when a calculus (urinary stone) that has entered the ureter from the kidney can linger at the site of narrowing, disrupting the outflow of urine through the ureter, thus causing renal colic (paroxysmal pain in the lower back and the corresponding half of the abdomen). ). The most common diseases of the ureters are: ureteral stones, ureteral strictures (pathological narrowing of the lumen), vesicoureteral reflux, ureterocele (cystic dilatation of the intravesical part of the ureter). Tumors of the ureter are rare.
Urethra
The urethra (urethra) is part of a woman's urinary system and a man's urinary and reproductive systems. In men, the 20 cm long urethra is located both in the pelvis and inside the penis, and opens into an external opening on the glans.
Anatomically, the following sections of the male urethra :
- External hole
- Scaphoid fossa
- Penile section
- Bulbous department
- Membranous section
- Prostatic section (proximal and distal sections)
Figure taken from www.urologyhealth.org
The prostatic urethra passes through the prostate and is divided into proximal and distal parts at the level of the seminal tubercle. In the proximal part of the prostatic urethra, the excretory ducts of the prostatic glands open at the orifices along the posterolateral surfaces. On the sides of the seminal tubercle are the mouths of the right and left ejaculatory ducts, through which sperm enters the lumen of the urethra from the seminal vesicles and vas deferens. In the distal part of the prostatic part and in the membranous part of the urethra there are elements of the urethral sphincter. Starting from the bulbar region, the urethra passes inside the corpus spongiosum of the penis. The bulbar region is located inside the bulb of the corpus spongiosum. In the membranous and bulbar sections, the urethra bends anteriorly upward. In the penile region, the urethra is located medially along the ventral surface of the penis downward from the cavernous bodies. The capitate part of the urethra is located inside the head of the penis. The inner surface of the male and female urethra is covered with mucous membrane (transitional epithelium, with the exception of a short area near the external opening, where there is flat non-keratinizing epithelium).
The main functions of the urethra in a man:
- Passage of urine from the bladder to the outside
- Carrying sperm out during ejaculation (ejaculation)
- Participation in the mechanism of urinary continence
The most common diseases of the urethra :
- Urethritis (inflammation of the urethra) often due to sexually transmitted infections (gonococci, chlamydia, ureoplasma, etc.).
- Strictures (narrowing of the lumen) of the urethra in its various parts (due to formation: congenital, traumatic and inflammatory origin).
- Anomalies of urethral development: the most common is hypospadias (the location of the external opening of the urethra on the ventral surface of the penis is more proximal than the apex of the glans).
Seminal vesicles
The seminal vesicles are the organs of the male reproductive system. The seminal vesicles (right and left) are located on the posterior surface of the prostate on the sides of it, posterior to the bladder, anterior to the rectum. The seminal vesicles can be palpated with a finger through the anterior wall of the rectum on either side of the basal parts of the prostate. The seminal vesicles are approached by the vas deferens, which, after joining the seminal vesicles, become the ejaculatory ducts. The ejaculatory ducts pass through the prostate and open at the mouths into the lumen of the prostatic urethra on the sides of the seminal tubercle. The tissue of the seminal vesicle has a cellular structure.
The main functions of the seminal vesicles are:
- In the production of a significant part of the seminal fluid (up to 75% of the ejaculate volume).
- In the accumulation of components of seminal fluid until the moment of ejaculation (there are usually no sperm from the seminal vesicles, and the main receptacle for sperm is the ampoules of the vas deferens).
- Participating in the mechanism of ejaculation (at the moment of ejaculation, the contents of the seminal vesicles and vas deferens enter the urethra through the ejaculatory ducts, where they are mixed with prostate secretions and discharged out).
Pathology of the seminal vesicles (usually inflammation - vesiculitis) can lead to deterioration in sperm quality and infertility.
Testicular arteries and veins
Testicular veins and arteries are vessels that supply the male sex glands - the testicles. On each side there is one testicular artery and one, and often several, testicular veins. On the right side, the testicular artery arises from the aorta, and the testicular vein flows into the inferior vena cava. On the left side, the testicular artery arises from the left renal artery, and the testicular vein drains into the left renal vein. The testicular vessels pass vertically to the right and left in the retroperitoneal space lateral to the ureters, penetrate the inguinal canal through the internal inguinal ring, and as part of the spermatic cord, exiting through the external inguinal ring, approach the upper pole of the testicle. As part of the spermatic cord and in the scrotum, the testicular veins form the testicular venous plexus. The outer diameter of the testicular artery is usually 0.5–1.0 mm. The most common pathology associated with testicular vessels is varicocele (varicose veins of the testicular venous plexus). Varicocele develops, as a rule, in young people aged 12–15 years, most often on the left side. With insufficiency of the venous valves and increased pressure in the left testicular vein system (anatomical predisposition), due to blood flow in the opposite direction, a compensatory expansion of the scrotal veins of varying degrees occurs. Impaired blood supply to the testicle (high venous pressure) and impaired thermoregulation of the scrotum (the testicle is located in the scrotum to operate at a temperature below body temperature, and a large mass of blood in the dilated veins disrupts these conditions) leads to dysfunction of the testicle. Varicocele is one of the common causes of male infertility. Moreover, the longer a varicocele is present, the greater the likelihood of pronounced disturbances in sperm quality (sperm concentration and motility) and the degree of hormonal changes. In recent years, it has been found that varicocele may be the cause of an earlier onset of male menopause.
Similar
How to avoid complications of urethritis? How not to miss the disease?
To avoid complications, more frequent preventive examinations should be carried out, especially after unprotected sexual intercourse, even in the absence of complaints. The earlier the diagnosis is made, the easier the treatment will be.
In fact, sex, no matter what it is (vaginal, oral or anal), can be equally unsafe, since all body fluids can contain a variety of pathogens. Unsafe sexual intercourse means promiscuity and frequent changes of sexual partners.
Frequent change of sexual partners
But even one woman is not a guarantee of health, since she can have an intimate relationship with another man. In this sense, a condom is a reliable barrier to the spread of infection.
From the data provided, it is clear that only a urologist who conducts special and serological tests can determine the cause of urethritis and what infection caused the urethritis - a possible option, even several infections at once. Some of them may have an incubation period and may not appear immediately. Therefore, having noticed unpleasant signs, there is no need to immediately blame the last partner.
Diagnostics
The following tests and procedures may be used to diagnose urethral diseases:
- Anamnesis collection.
- Digital rectal examination: examination of the rectum and prostate.
- General urine analysis.
- Urine cytology: A laboratory test in which a urine sample is examined under a microscope for abnormal cells.
- Culture of urethral discharge.
- CT scan.
- Urethroscopy: a procedure for examining the urethra with a special thin instrument.
Symptoms
At the initial stage of development, urethritis does not manifest itself with severe symptoms. Almost always, men experience slight discomfort in the penile canal, and women experience slight discomfort in the lower abdomen, slightly above the pubis. Such symptoms often go unnoticed.
As a rule, patients consult a doctor when the disease becomes acute. This is manifested by severe pain and burning when urinating. There is also a frequent urge to urinate, but the bladder cannot be emptied completely. In severe cases, the following symptoms are noted:
- Cloudy urine, possible inclusions of blood and mucus;
- Purulent discharge with an unpleasant odor.
In addition, a symptom of inflammation of the urethra is redness:
- In men, the external opening of the urethra.
- In women, the labia majora and minora.
Strictures of the external urethral meatus and navicular fossa
If the narrowing is small, then a meatotomy is possible - this is a longitudinal dissection of the external opening of the canal and the application of a transverse suture to the mucous membrane and skin of the head of the penis. It is important to suture the mucosal tissue rather than the submucosal tissue. The error leads to new scarring and an increase in the size of the narrowing.
If the stricture of the outer part of the scaphoid fossa is short, then plastic surgery is performed with a glans flap. This approach makes it possible to increase the lumen of the fossa. For longer urethral strictures, tissue from the foreskin or cheek is used.
General methods of treating urethral diseases
Treatment of urethral diseases depends on the type of disease. It can be either conservative (various medications and physical procedures) or surgical.
The Department of Urology of the Moscow State University named after M.V. Lomonosov, when choosing surgery as a treatment method, always gives preference to minimally invasive methods - the most progressive method of surgical interventions. This ensures minimal impact on surrounding tissue and rapid recovery.
More information about urethral diseases: