What is chronic heart failure
When the heart does not provide sufficient blood supply to the body, it causes swelling and oxygen starvation of tissues and internal organs. This condition is called heart failure and has two forms - acute and chronic.
The acute form occurs due to a sharp disturbance in the contractile activity of the myocardium, is accompanied by severe pain in the chest and always requires emergency medical care. An attack can be triggered by: exacerbation of a current cardiovascular disease, sudden damage to the heart muscle, poisoning, trauma, stroke, etc.
Chronic form of heart failure
, unlike acute, it begins asymptomatically and develops gradually. The initial stage of the disease does not have obvious symptoms, and heart problems can only be identified during a medical examination. Over time, the patient develops shortness of breath and rapid heartbeat during physical activity. In later stages, these symptoms persist even at rest.
Structure of the heart: atria, ventricles and heart valves
Chronic heart failure
The data on chronic heart failure (CHF) that have accumulated in recent years have led to the need for a unified approach to the diagnosis and treatment of this pathology, which in turn has contributed to the emergence of a number of advisory documents. Over the past 5 years alone, authoritative cardiological associations have already published several revisions of their recommendations for the diagnosis and treatment of CHF: American College of Cardiology / American Heart Association (2001, 2005), European Heart Association (2001, 2005), VNOK (1993, draft, 2006 ).
Ideas about CHF have been constantly changing over the past decades. Moreover, not only the issues of pathogenesis, diagnosis and treatment, but also approaches to determining
CHF.
Thus, in the European recommendations of 2001
CHF is presented as “
a pathophysiological syndrome
in which, as a result of a particular disease of the cardiovascular system, a decrease in pumping function occurs, which leads to an imbalance between the hemodynamic need of the body and the capabilities of the heart.”
According to the domestic recommendations of the All-Russian Scientific and Cultural Organization (2003),
CHF is also “
a syndrome
that occurs when a person has systolic and/or diastolic dysfunction, accompanied by chronic hyperactivation of neurohormonal systems and clinically manifested by shortness of breath, weakness, palpitations, limitation of physical activity, pathological fluid retention in the body "
At the same time, the modern neurohormonal theory of the pathogenesis of heart failure has convincingly shown that, regardless of the initial causes, its development occurs on a single pathophysiological basis. These provisions allowed GFCI experts to put forward a proposal that CHF is a separate nosological unit, and in the draft national recommendations of GFCI and OSCH of 2006
.
CHF is proposed to be understood as “ a disease with a complex of characteristic symptoms (shortness of breath, fatigue and decreased physical activity, edema, etc.), which are associated with inadequate perfusion of organs and tissues at rest or during exercise and often with fluid retention in the body.”
Active studies of any individual component of the pathogenesis of CHF in different years have led to the emergence of different pathophysiological definitions and, accordingly, models of its development (Table 1).
| Most common etiological factors CHF remains coronary heart disease (CHD), in particular myocardial infarction (MI), angina pectoris and ischemic cardiomyopathy, which is primarily associated with a decrease in global systolic function of the left ventricle (LV). The second and third positions are occupied by dilated cardiomyopathy and rheumatic heart defects, respectively. At the same time, in people over 70 years of age, hypertension and associated disturbances in myocardial diastolic relaxation play a leading role in the development of CHF, along with ischemic heart disease. Diagnostics CHF is built on three main pillars: 1) clinical manifestations, among which the most common are shortness of breath, fatigue and decreased performance, peripheral edema; 2) objective signs of heart damage, that is, evidence of the connection of clinical signs specifically with cardiac and not other pathology; 3) ex juvantibus effect. In this case, the presence of the first two criteria is mandatory. However, diagnosing CHF is quite a difficult task, since clinical signs, like objective data, are very nonspecific and can occur in a wide variety of diseases. At the same time, they should be constantly remembered, since it is they who, already at the first communication between the doctor and the patient, allow one to suspect the presence of CHF. The most common symptoms and objective data characteristic of CHF are presented in table. 2. | It should be remembered that such characteristic clinical symptoms CHF, such as peripheral edema, wheezing in the lungs, orthopnea and cough, are not as common - from 28 to 73%, according to the IMPROVEMENT study (2000). But the most common complaints are shortness of breath (98.4%), fatigue (94.3%) and palpitations (80.4%). The second important “pillar” on which the diagnosis of CHF is based is the results of instrumental and laboratory tests, making it possible to associate the occurrence of very nonspecific clinical symptoms with the pathology of the cardiovascular system, and not any other system.
The simplest and most accessible method, electrocardiography
, is almost never normal (negative predictive value >90%).
Most often, the ECG records signs of myocardial hypertrophy, focal changes of a cicatricial nature, and various disturbances of heart rhythm and conduction. Chest X-ray
allows you to verify cardiomegaly and venous congestion.
The dynamics of the last sign can be used as a criterion for the effectiveness of therapy. Extremely important and most complete information about the structural and functional state of the heart can be obtained from echocardiography.
The method allows not only to identify the very fact of a decrease in myocardial contractile function, but also to assess its degree and dynamics during the treatment process.
The most common indicator associated with the systolic function of the left ventricle is the ejection fraction, although shortening fraction, myocardial contractility index, sphericity index, etc. are also used to assess the latter. Low EF values are a predictor of an unfavorable prognosis in patients with CHF. It should be remembered that a normal ejection fraction does not exclude the presence of CHF. Individuals with normal or slightly reduced EF (≥50%) and clinical symptoms of CHF are most likely to have diastolic heart failure. In addition to the first two conditions, to verify diastolic HF, the presence of signs of impaired LV relaxation and/or its distensibility (the ratio of the peak velocity of early and late ventricular filling E/A, the time of LV isovolumic relaxation, the time of blood flow deceleration, etc.) is required. In addition to the functional characteristics, Echo-CG allows one to assess the size and volume of the chambers of the heart, as well as their dynamics during treatment, the condition of the heart valve apparatus, pressure in the cavities and large vessels, etc. When transthoracic access is limited, there is a suspicion of complicated valvular heart disease, valvular dysfunction can be performed on the prosthesis .
Routine laboratory tests blood (clinical analysis, creatinine, urea, electrolytes, “liver” enzymes, thyroid hormones) and
urine
(general analysis, functional tests) primarily serve to exclude extracardiac (renal, thyroid, etc.) causes of clinical symptoms characteristic of CHF. However, the presence of anemia is currently recognized as an unfavorable prognostic factor in patients with CHF. A close relationship is clearly shown between the severity of CHF and the content of natriuretic peptides in plasma, which makes an increase in the latter a kind of “laboratory” criterion for CHF. Moreover, their definition should be used not so much to confirm, but rather to exclude the diagnosis of CHF (negative predictive value >90%). Classification of CHF provides for an assessment of the patient’s condition in two main positions: a) stage of the disease (an irreversible process that can be slowed down and even stopped for a while, but stage II will never turn into stage I) and b) the functional capacity of the cardiovascular system (functional class of CHF – a dynamic parameter that can change during treatment). With regard to the first point, the Vasilenko-Strazhesko classification was recognized as the most successful (Table 3), with regard to the second – the NYHA classification (Table 4). Determining the functional class of CHF according to this classification is based on a certain degree of subjectivity, therefore, in practical clinical activities, a 6-minute walk test is used to objectify this process. Depending on the distance that a particular patient can walk in 6 minutes, one or another class of CHF is verified (Table 5). | The severity of heart failure, assessed by functional class, has prognostic significance. Thus, the annual mortality rate of patients with FC I CHF is about 10%, FC II - 20, FC - 40, FC IV - more than 60%. Despite the introduction of new treatment methods, the mortality rate of patients with CHF remains virtually unchanged. Treatment of CHF - a very complex and expensive task.
The following main goals of therapy
: - elimination or minimization of clinical symptoms;
- slowing down the progression of the disease by protecting target organs (vessels, heart, kidneys, brain);
- improving quality of life;
- increase in life expectancy;
- reduction in the number of hospitalizations.
There are six ways to achieve your goals when treating decompensation: - diet
- physical activity regimen;
- psychological rehabilitation, organization of medical supervision, schools for patients with CHF;
- drug therapy;
- electrophysiological methods of therapy;
- surgical, mechanical methods of treatment.
Diet. The main principle is to limit salt consumption, and the more, the greater the FC of CHF. In FC I, it is recommended not to eat salty foods (up to 3 g NaCl); at FC II, do not add salt to food (up to 1.5 g NaCl); at III FC plus products with reduced salt content and preparation without salt (<1.0 g NaCl). Recommendations for fluid restriction are relevant only for decompensated CHF, when parenteral administration of diuretics is required. Patients should strictly monitor their weight; an increase of 2 kg or more over several days most often indicates fluid retention and a high risk of decompensation. Physical activity indicated for all patients with CHF, regardless of severity. However, its nature and volume depend on the functional class (Fig. 1). During the training process, you should constantly evaluate the effectiveness of the activities carried out, determine the functional class based on the 6-minute walk test and, depending on this, move from one level to another. Moreover, the transition process should be quite long and take from 5-6 to 10-12 weeks. Rice. 1. The volume of physical activity in patients with CHF. Drug therapy for CHF From the standpoint of evidence-based medicine, all drugs that are used to treat CHF are divided into three groups: main (their effectiveness has been proven and is beyond doubt),
additional
(their effectiveness and safety have been studied, but require clarification),
auxiliary
(their effect on the prognosis has not been proven, but they improve the clinical picture). Main This group of drugs fully meets the criteria of evidence-based medicine and is recommended for use. These are ACE inhibitors (ACEIs), beta-blockers (BABs), aldosterone antagonists (AAs), diuretics (D), cardiac glycosides (CGs) and angiotensin receptor antagonists (AARs, currently only candesartan). It is possible to assign additional group of drugs, which currently consists of statins and anticoagulants. Auxiliary The drugs are peripheral vasodilators, antiarrhythmics, calcium channel blockers, antiplatelet agents, non-glycoside inotropic agents. It is worth dwelling on a brief description of the drugs of the main group. ACE inhibitors. To date, ACEIs firmly occupy a leading position in the list of drugs for the treatment of CHF. Back in 1995, a meta-analysis that included more than 7,100 patients demonstrated the ability of ACE inhibitors to reduce the risk of death in patients with CHF by 23%, and this effect was even more pronounced in the first 90 days of treatment (44% risk reduction). These results have been repeatedly confirmed in many studies and analyzes showing that the positive effects of ACE inhibitors do not depend on age and persist in most clinical situations and with any severity of CHF. The main provisions for the use of ACE inhibitors are as follows: - ACE inhibitors should be prescribed to all patients with CHF, regardless of the etiology and stage of the process. However, the effectiveness of ACE inhibitors for ischemic etiology of CHF and in women is somewhat lower. Concomitant use of non-steroidal anti-inflammatory drugs may also weaken the effect of ACE inhibitors.
- ACE inhibitors can improve clinical symptoms, quality of life (QoL), slow the progression of the disease, reduce morbidity and improve the prognosis of patients with CHF.
- The effectiveness of ACE inhibitors is manifested in all stages of CHF - from the very beginning, including asymptomatic LV dysfunction, to the most advanced stages of decompensation.
- In individuals with preserved systolic cardiac function, ACEIs are the most reasonable method of treating CHF.
Most common adverse reactions when prescribing ACE inhibitors (in total, no more than 7-9% of the reasons for cancellation) are dry cough, arterial hypotension, an increase in the degree of chronic renal failure in the form of azotemia, hyperkalemia. ACEIs are absolutely contraindicated only in cases of known intolerance (angioedema), bilateral renal artery stenosis and pregnancy. The initiation of ACEI therapy should be carried out with small doses with gradual (no more than once every 2-3 days, and in case of systemic hypotension - once a week) titration to optimal (average therapeutic) doses. Table 6 presents the doses of the main representatives of the ACEI group, the most studied in terms of the treatment and prevention of CHF and registered in the Russian Federation. | Beta blockers. To date, more than 30 studies have been completed, including more than 20 thousand patients with CHF, which have shown the ability of blockers to reduce the mortality of patients with decompensation by 29% (it should be noted that in most cases, blockers were used in addition to ACE inhibitors). Therefore, since 1999 in the USA and European countries, and a little later in Russia, beta-blockers have been recommended for use as the main means for the treatment of CHF. However, not all beta-blockers have a positive effect in CHF. Currently, the effectiveness of beta blockers in reducing mortality and the number of hospitalizations has been proven for only three drugs: carvedilol (BAB with alpha-blocking activity, as well as antiproliferative and antioxidant properties),
bisoprolol
(the most selective blocker for b1 receptors) and
metoprolol succinate
(a selective lipophilic beta-blocker of prolonged action).
In addition to the three recommended beta blockers, nebivolol
of age, which does not significantly reduce mortality, but reduces the morbidity of patients and the number of re-hospitalizations (SENIORS study). The main provisions for the use of ACE inhibitors are as follows: - In their ability to reduce the risk of morbidity and death in decompensated patients, beta blockers are even superior to ACE inhibitors.
- Along with ACE inhibitors, beta blockers are the main means of treating CHF. Their use can slow down the progression of the disease, reduce the number of hospitalizations and improve the prognosis of patients.
- In most cases, beta blockers are prescribed in addition to ACE inhibitors for patients in a stable condition. In rare situations (the predominance of severe tachycardia at low blood pressure, when the combination of an ACE inhibitor and a beta blocker is difficult), you can start therapy with the β1-selective beta blocker bisoprolol, followed by the addition of an ACE inhibitor (CIBIS-III study).
- The starting dose of any beta-blocker in the treatment of CHF is 1/8 of the average therapeutic dose: 3.125 mg twice a day for carvedilol, 1.25 mg for bisoprolol, 12.5 mg for metoprolol, 1.25 mg for nebivolol.
- Doubling the dosage of beta blockers should be done no more often than once every two weeks, provided that the patient’s condition is stable and there is no bradycardia or hypotension.
Contraindications for the prescription of beta blockers for CHF are: bronchial asthma, symptomatic bradycardia (<50 beats/min), symptomatic hypotension (<85 mm Hg), AV block of II or more degrees, severe obliterating endarteritis. Table 7 presents the starting, therapeutic and maximum doses of beta blockers recommended for the treatment of CHF. | Aldosterone antagonists (spironolactone) have been used in the treatment of CHF for more than 40 years. In high doses, the drug is successfully used in complex diuretic therapy of severe CHF as a potassium-sparing diuretic, potentiating the effect of loop and thiazide diuretics. Its prescription during the period of decompensation of CHF in combination with other diuretics was not in doubt. The results of some studies (primarily RALES) have expanded the list of indications for its use, especially in patients with FC III-IV. In small dosages (the average dose in this study was 27 mg), aldactone exhibits the properties of a neurohumoral modulator and, in combination with ACE inhibitors and beta blockers, can significantly reduce the risk of death by 27%, both sudden and associated with exacerbation of decompensation. The question of using small doses of aldactone in patients with low functional class of CHF (FC I-II) remains open. Although there is already evidence that in patients who suffered a MI complicated by the development of class II CHF, the use of the new aldosterone antagonist eplerenone reduced the risk of death, nevertheless, the administration of small doses of spironolactone to patients with class II CHF cannot yet be strictly recommended. Based on adverse reactions spironolactone (in addition to possible hyperkalemia and an increase in creatinine levels), the development of gynecomastia should be noted (up to 10% of patients). The frequency of the latter effect when taking a new (not yet registered in the Russian Federation) drug of this group, eplerenone, does not exceed 1%. Diuretics. There are currently no multicenter controlled studies examining the effectiveness of diuretics in CHF. Nevertheless, the accumulated many years of positive experience in the use of diuretics in patients with clinical signs of overhydration allowed experts to place this group of drugs on the list of “essential” drugs for the treatment of CHF. The main provisions for the use of diuretics are as follows: - The main indication for prescribing diuretics is the elimination of edema syndrome and improvement of clinical symptoms of patients with CHF. When used correctly, these drugs can reduce the number of hospitalizations, but do not affect the progression of CHF and do not improve the prognosis of patients. Their impact on the quality of life if prescribed incorrectly (loading doses every 3-4-5-7 days) can even be negative.
- Diuretics are prescribed only for clinical signs of stagnation (stage IIA). Prophylactic use of diuretics is not indicated, as they do not improve the prognosis.
- Therapy with diuretics should be combined with the use of neurohormonal modulators, such as ACE inhibitors and aldosterone antagonists, to prevent refractoriness to diuretics.
- Preference should be given to thiazide diuretics (hypothiazide) and only if they are insufficiently effective, proceed to the prescription of powerful “loop” diuretics (furosemide, uregit, bumetanide).
- Treatment should begin with small doses, subsequently selecting the dose according to the principle of quantum satis.
Recommended doses for the most commonly used diuretics: - hypothiazide: starting = 25 mg, maximum = 75-100 mg;
- furosemide: starting = 20-40 mg, maximum = up to 500 mg;
- uregitis: starting = 25-50 mg, maximum = up to 250 mg;
- bumetanide: starting = 0.5-1.0 mg, maximum = up to 10 mg.
In 2006, the loop diuretic torasemide was registered in the Russian Federation, which, in comparison with furosemide, demonstrated a better ability to influence the prognosis of patients with CHF. The initial dosage of the drug is 5-10 mg and can subsequently be increased to 100-200 mg per day. We should not forget about diacarb, the main mechanism of action of which is the blockade of carbonic anhydrase in the epithelium of the proximal renal tubules, which ultimately, in addition to the diuretic effect, leads to acidification of the urine. This effect is especially necessary in the case of development of resistance to loop diuretics, as well as in patients with concomitant COPD. Diacarb is prescribed 0.25 mg three times a day for 3-4 days with an interval of 2-3 weeks. The main indication for prescribing diuretics is the clinical signs and symptoms of excessive fluid retention in the body of a patient with CHF, but one should remember their side effects : 1) hyperactivation of neurohumoral systems (once again emphasizing the need for parallel administration of ACE inhibitors and aldactone) and 2) changes in metabolic status (carbohydrate, lipid and electrolyte metabolism, usually in high doses - for hypothiazide more than 50 mg/day). Diuretic therapy in patients with CHF has two phases - active and maintenance. In the first active phase, a combination of diuretics is used with the mandatory inclusion of loop diuretics. The main criterion for effectiveness is the excess of excreted urine over the administered fluid by about 1 liter per day with a decrease in body weight of about 700-900 g per day. Rapid dehydration cannot be justified and only leads to hyperactivation of neurohormonal systems and rebound fluid retention in the body. At the stage of maintenance diuretic therapy, the water balance should be zero with possible fluctuations of up to 200 ml in both positive and negative directions. Cardiac glycosides do not affect the prognosis and progression of CHF, but are able to improve clinical symptoms, quality of life and reduce the number of hospitalizations, which allows us to classify this group of drugs as the “main” drugs for the treatment of CHF. It should be remembered that cardiac glycosides, in addition to the positive inotropic and negative chronotropic effect on the myocardium, also have a neuromodulatory effect. Currently, the most common cardiac glycoside in Russia is digoxin. Non-glycoside drugs that have the ability to increase myocardial contractility negatively affect the prognosis and life expectancy of patients and can only be used in short courses for decompensated CHF. The greatest effectiveness of glycosides is achieved in patients with low EF (<25%), large heart sizes (cardiothoracic index >55%) and non-ischemic etiology of CHF. Glycosides are especially indicated in patients with atrial fibrillation. Their ability to reduce heart rate by blocking AV conduction is well known, but is not always sufficient when the patient is physically active. In the latter case, the combination of digoxin with a beta blocker is optimal, which, in addition to optimal control of the rhythm frequency, helps prevent the development of life-threatening ventricular arrhythmias. Currently, the most optimal is to prescribe small doses of glycosides (digoxin no more than 0.25 mg per day), preferably under the control of its concentration in the blood plasma (no more than 1.2 ng/ml). It must be remembered that plasma digoxin concentrations increase exponentially by the eighth day from the start of therapy, so such patients are ideally advised to perform 24-hour ECG monitoring to monitor the PQ interval and verify rhythm disturbances. It should be remembered that treatment with glycosides in women is more often accompanied by the development of intoxication and fatal complications, even with the same dosages of the drug as in men. Angiotensin II receptor antagonists. Despite the theoretical prerequisites for achieving complete blockade of the renin-angiotensin system with drugs of this group, until recently it was not possible to detect even effects comparable to ACE inhibitors on solid endpoints in patients with CHF. However, the recently completed CHARM study showed that taking candesartan in people with low ejection fraction was associated with a reduction in mortality and hospitalizations. At the same time, candesartan does not have the ability to improve the prognosis of patients with preserved LV systolic function. The ELITE-II study showed that losartan was only slightly and nonsignificantly inferior to captopril in terms of its effect on hard endpoints in patients with decompensated CHF. In addition, in individuals with diabetic nephropathy, losartan is able to prevent the development of CHF. The combination of an ACEI and the ARA valsartan does not affect the prognosis, but can reduce the number of hospitalizations (Val-HeFT). Summarizing the above, it should be emphasized that in patients with CHF with reduced LV systolic function, the ARA candesartan can become an alternative to the ACEI. The prescription of other ARAs (losartan, valsartan) is especially indicated for intolerance to ACE inhibitors. Ruslan LINCHAK, Head of the Cardiology Department of the National Medical and Surgical Center named after. N.I. Pirogova, Candidate of Medical Sciences, Associate Professor |
|
|
|
|
|
|
Reasons for development
Chronic heart failure occurs against the background of other diseases that affect the myocardium and blood vessels. Therefore, it is always necessary to treat or keep primary diseases under medical supervision, as well as monitor the condition of your circulatory system.
Factors in the development of CHF
- Arterial hypertension (AH) is the main cause of chronic heart failure.
- Coronary heart disease (CHD) is in second place among the provoking factors.
- Cardiomyopathies (including those provoked by infectious diseases, diabetes mellitus, hypokalemia, etc.).
- Valvular (mitral, aortic, tricuspid, pulmonary) and congenital heart defects.
- Arrhythmias (tachyarrhythmias, bradyarrhythmias).
- Diseases of the pericardium and endocardium.
- Conduction disturbances (antrioventricular block).
- High load (for example, with anemia).
- Volume overload (eg, renal failure).
The course of any disease from the list above should be monitored by the attending physician
Stages and symptoms of CHF
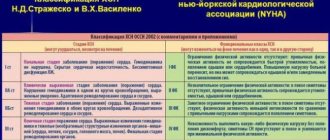
In Russian medicine, two classifications of chronic heart failure are used: classification of chronic circulatory failure N.D. Strazhesko, V.Kh. Vasilenko and the functional classification of the New York Heart Association. In diagnosing the disease, the indicators of both systems are taken into account.
Classification by N. D. Strazhesko, V. Kh. Vasilenko (1935)
The patient's condition is assessed by the number and severity of clinical manifestations of the disease.
Stage 1
Initial, latent circulatory failure, manifested only during physical activity (shortness of breath, palpitations, excessive fatigue). With rest, these phenomena disappear. Hemodynamics are not impaired.
Stage 2
Severe, prolonged circulatory failure, hemodynamic disturbances (stagnation in the pulmonary and systemic circulation), dysfunction of organs and metabolism are also expressed at rest. Working capacity is sharply limited.
Period 2a
- Hemodynamic disturbances are moderate, and dysfunction of any part of the heart is noted (right or left ventricular failure).
Period 2b
- Severe hemodynamic disturbances, involving the entire cardiovascular system, severe hemodynamic disturbances in the small and large circles.
Stage 3
Ultimate, dystrophic. Severe circulatory failure, persistent changes in metabolism and organ functions, irreversible changes in the structure of organs and tissues, pronounced dystrophic changes. Complete loss of ability to work.
The structure of the human circulatory system: arteries are marked in red, veins are marked in blue.
Functional classification of the New York Heart Association
Adopted in 1964 by the New York Heart Association (NYHA). This classification is used to describe the severity of symptoms; on its basis, four functional classes of the disease (FC) are distinguished.
- First class FC
. There are no restrictions on physical activity. Normal physical activity does not cause excessive shortness of breath, fatigue, or palpitations.
- Second class FC
. Slight limitation in physical activity. Comfortable state at rest. Normal physical activity causes excessive shortness of breath, fatigue, or palpitations.
- Third class FC
. Explicit limitation of physical activity. Comfortable state at rest. Less physical activity than usual causes excessive shortness of breath, fatigue, or palpitations.
- Fourth grade FC
. Inability to perform any physical activity without discomfort. Symptoms may be present at rest. With any physical activity, discomfort increases.
Classification of circulatory failure
To assess the degree of circulatory failure in children, the classification of N. D. Strazhesko and V. X. Vasilenko is usually used, according to which chronic heart failure is divided into three stages: HK1, HK2a, HK2b, HK3.
NK1 - the first stage of circulatory failure - is a period of hidden, latent failure. With it, symptoms of circulatory disorders are detected only during physical activity and are manifested by shortness of breath and tachycardia.
Initially, shortness of breath and tachycardia occur during heavy physical activity (quickly climbing stairs to high floors, doing physical education, sports, lifting weights, etc.), then these symptoms progressively increase, shortness of breath and tachycardia develop even with slight physical exertion (with slow climbing stairs, slow walking, etc.).
After cessation of physical activity, patients with circulatory insufficiency find it difficult to “catch their breath,” i.e., it takes a fairly long period of time to eliminate hypoxia and restore the normal frequency and depth of breathing. Patients complain of increased fatigue and decreased performance.
An objective examination of patients with HC1, except for shortness of breath and tachycardia that appears after exercise, signs of heart failure cannot be detected.
Currently, highly informative methods have begun to be used in clinical practice to detect the initial manifestations of heart failure. These methods include ultrasound location of the heart, based on the Doppler effect - echocardiography, which makes it possible to determine the thickness of the walls of the ventricles, the volume of the heart chambers, and also assess the contractility of the left ventricular myocardium. By changes in these indicators, one can judge the presence of circulatory failure.
HK2 - stage II of circulatory failure - is characterized by the presence of symptoms of heart failure at rest. The second stage of circulatory failure, according to the severity of hemodynamic disturbances, is usually divided into 2 periods - HK2a and HK2b.
HK2a is characterized by a predominant hemodynamic disturbance in the pulmonary or systemic circulation. Stagnation in this period is still not clearly expressed.
With HK2b, there are quite profound hemodynamic disturbances in both the pulmonary and systemic circulation as a result of failure of the right and left hearts.
HK2a is characterized by the presence of shortness of breath, tachycardia at rest and a sharp increase in these symptoms even with little physical activity. During an objective examination of the patient, slight cyanosis of the lips is observed, phenomena of myogenic dilatation of the heart are detected: it is significantly increased in size, the apex beat is weakened. The maximum blood pressure has not yet clearly changed, although a slight increase may be observed in some patients; the minimum pressure usually increases; hence the pulse pressure naturally becomes lower. Central venous pressure is increased. The clinical manifestation of increased venous pressure is swelling of the jugular veins. If there is a predominant lesion of the right parts of the heart, then with HK2a congestion in the systemic circulation is still less pronounced. There is a slight enlargement of the liver. In the early stages of stagnation, the liver is smooth, somewhat compacted, and painful on palpation. There is pastiness or moderate swelling of the legs. In some patients, swelling in the legs appears only in the evening; by morning it disappears.
If the left parts of the heart are predominantly affected, then symptoms of venous stagnation in the pulmonary circulation are revealed: congestive wheezing appears in the lungs, and an X-ray examination reveals a picture of venous stagnation in them.
HK2b is characterized by a significant enlargement of the liver, constant edema (transudate may appear in the cavities), and severe congestion in the lungs.
As a result of changes in hemodynamics in the systemic circulatory system, renal dysfunction may develop, which is characterized by the appearance of albuminuria from traces to whole ppm, microhematuria, and cylindruria. During the period of increasing edema, oliguria occurs. The concentrating function of the kidneys at this stage of circulatory failure usually does not suffer significantly. With proper and timely treatment, all these symptoms can disappear. This stage of circulatory failure is still reversible.
At stage HK3, as a result of persistent hemodynamic disturbances, along with pronounced symptoms of heart failure, irreversible degenerative changes in organs and tissues develop (cardiac cirrhosis of the liver, dystrophy, etc.).
In 1955, A. N. Bakulev and E. A. Damir proposed a classification of the stages of heart failure for patients with mitral stenosis, taking into account hemodynamic features. They identified 5 stages of circulatory failure.
This classification is used to assess circulatory failure mainly in cardiac surgery clinics.