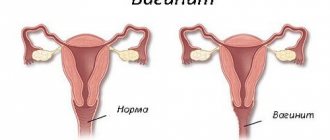
In a healthy state, a certain amount of opportunistic bacteria is always present on the vaginal mucosa, but their “aggressive” activity is restrained by other “useful” microorganisms (for example, Doderlein’s bacillus). With hormonal imbalances, decreased immunity, injuries, hypothermia and other changes in the female body, the protection of the reproductive system weakens, as a result of which an inflammatory process develops.
Treatment of colpitis is a common problem with which patients come to us. Basically, vaginitis in women occurs during childbearing years, but this diagnosis can also be given to very young girls or women after menopause.
Types of colpitis (vaginitis)
According to the form of the disease, they are distinguished:
- acute vaginitis;
- subacute vaginitis;
- chronic vaginitis.
The stages of development of the disease differ in the severity of symptoms and the different nature of the course.
According to the etiological type, they are distinguished:
- specific vaginitis (inflammation caused by sexually transmitted infections);
- nonspecific vaginitis (inflammation caused by opportunistic microorganisms);
- atrophic vaginitis (caused by natural aging of the body).
If you do not take into account atrophic colpitis, from the point of view of etiology there is infectious and bacterial (aerobic) vaginitis. They develop in women of reproductive age.
Atrophic colpitis occurs, as a rule, in 90% of women after menopause. Because of this, it is often called postmenopausal vaginitis. With atrophic vaginitis, a gradual thinning of the epithelium of the vaginal walls occurs due to a decrease in estrogen levels.
Depending on the type of pathogen, it is customary to differentiate:
- Trichomonas vaginitis (caused by the bacteria Trichomonas vaginalis)
- candidal vaginitis (caused by fungi of the genus Candida)
Separately, it is worth identifying this type of vaginitis as colpitis during pregnancy . It occurs in pregnant women against the background of hormonal changes or decreased immunity, and can also be brought in from outside due to insufficient hygiene rules.
All of the listed types of colpitis, including chronic forms of the disease, can be successfully treated. However, when treating vaginitis in pregnant women, there are many contraindications. To preserve the health of the woman and the unborn child, it is necessary to consult a gynecologist.
ETIOLOGY AND EPIDEMIOLOGY
Aerobic (nonspecific) vaginitis is a polymicrobial disease in which the anaerobic species of lactobacilli, which normally prevail, are replaced by aerobic bacteria, mainly Streptococcus spp., Staphylococcus spp., Enterococcus spp., bacteria of the Enterobacteriaceae family (E. coli, Klebsiella spp. , Citrobacter spp., Enterobacter spp., Serratia spp., Proteus mirabilis, Morganella morganii), with the development of an inflammatory reaction.
The prevalence of AV in the female population is 5–10%; among pregnant women it reaches 8.3–12.8%. In women with symptoms of inflammatory diseases of the reproductive tract, AV is observed in 23–30% of cases. The most severe form of AV is desquamative inflammatory vaginitis.
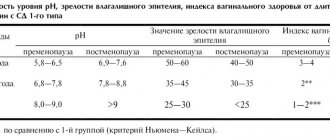
AB is most often detected in girls before menarche and in women during the menopausal period, when, due to physiological reasons (low levels of estrogens that control the exchange of glycogen in the vaginal epithelium), the number of lactobacilli decreases. In reproductive age, the main causes of AV development, as a rule, are infectious diseases, endocrine pathology, decreased functional activity of the ovaries, and exposure to local damaging factors.
In old and senile age, the development of AV is largely due to a decrease in the activity of protective factors of the vaginal mucosa, namely a decrease in the formation of lactic acid from glycogen. Replacement of other members of the microbial community by opportunistic microorganisms with predominantly aerobic catabolism leads to the development of vaginitis with a pronounced leukocyte reaction and clinical signs of inflammation.
The exact causes and mechanism of development of AV have not yet been fully determined. However, it has been established that in the etiopathogenesis of the disease, the microbial factor plays the same important role as the state of the macroorganism and those circumstances that change its immunobiological properties.
Risk factors for the development of AV most often include: metabolic disorders; general infectious diseases; nutritional factor; chronic stressful situations; toxic effects of certain medications (antibacterial, cytostatic, glucocorticosteroid agents, antacids); various extragenital diseases, complicated pregnancy and childbirth.
AB refers to diseases that do not pose a direct threat to a woman’s health. However, with this dysbiosis of the vaginal biotope, the lower parts of the genital tract are massively colonized by opportunistic microorganisms, which are the main causative agents of purulent-inflammatory diseases of the pelvic organs. Bacteria such as Staphylococcus spp., Streptococcus spp., coliform bacteria (Escherichia coli) are considered by modern researchers as the most common causative agents of chorioamnionitis, intraamnial infection, postpartum endometritis, and postoperative inflammatory complications.
According to many researchers, AV is a more common cause of pregnancy complications than bacterial vaginosis. It is also associated with premature rupture of membranes, premature birth and low fetal weight. Another very significant complication of AV, as stated earlier, is the development of inflammatory diseases of the pelvic organs in women.
CLASSIFICATION
There is no generally accepted classification of AB. There are acute, subacute, chronic (recurrent) and subjectively asymptomatic forms of the disease. The severity of AV is established based on the clinical picture and criteria for microscopic diagnosis of aerobic vaginitis (Table 1).
CLINICAL PICTURE
Subjective symptoms:
- profuse yellowish or yellow-green discharge from the genital tract, sometimes with a putrid odor. The disease can last a long time with periodic improvements and exacerbations. In some cases, exacerbations of the disease are observed after menstruation;
- discomfort in the external genital area;
- pain during sexual intercourse (dyspareunia);
- Sometimes there is itching and a burning sensation in the genital area.
Objective sympathomas:
A feature of the course of AV is the presence of a pronounced inflammatory reaction of the vaginal mucosa. During a gynecological examination in the acute stage of the disease, pain during the insertion of speculum, swelling, hyperemia, petechial rashes, superficial erosions of the mucous membrane of the walls and vestibule of the vagina are noted. In chronic forms of AV, these signs are less pronounced.
DIAGNOSTICS
Diagnosis of AV is based on medical history, results of clinical examination and laboratory tests.
Laboratory research
1. Microscopic examination of vaginal discharge (400x magnification, phase-contrast microscope).
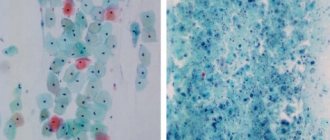
The microscopic picture of a Gram-stained smear is characterized by the following signs typical of an exudative inflammatory process:
- the vaginal epithelium is represented by superficial and intermediate cells; with a pronounced inflammatory process, parabasal cells are observed;
- leukocyte reaction expressed to varying degrees (>15–20 leukocytes per field of view);
- the total number of microorganisms is moderate or abundant;
- Lactobacillus spp. absent or their number is sharply reduced (to a few in the field of view);
- morphotypes of opportunistic microorganisms predominate - coliform bacilli or gram-positive cocci.
For a more accurate diagnosis of AB and assessment of lactobacilli deficiency, it is recommended to determine the lactobacillary grading (LBG), an indicator of the colonization of the vagina with lactobacilli,
which is detected by microscopy of a vaginal smear stained with Gram stain (Table 1).
Degrees I and II A are considered an indicator of vaginal normocenosis. To determine the presence and severity of AV, GG Donders (2002) proposed criteria similar to the R. Nugent system for diagnosing bacterial vaginosis (Table 2).
Points are assessed separately according to 5 criteria (lactobacillary degree, leukocyte count, proportion of toxic leukocytes, background microflora, proportion of parabasal epithelial cells) and are summed up.
- Sum of points up to 3 – no signs of AB;
- 3–4 points – mild degree of AB;
- 5–6 points – moderate AV;
- 6–10 points – severe AV, incl. 8–10 – aerobic desquamative inflammatory vaginitis.
2. Culture testing is traditionally used in clinical practice to identify pathogens, their quantitative assessment and determine the antibacterial sensitivity of isolated isolates. In case of AV, cultural examination reveals:
- lack of growth of lactobacilli or their minimal number;
- high quantitative indicators of aerobic opportunistic microorganisms in the form of monoinfection or polymicrobial associations.
In case of AV, Streptococcus, Staphylococcus spp., Enterococcus spp., bacteria of the Enterobacteriaceae family (E. coli, Klebsiella spp., Citrobacter spp., Enterobacter spp., Serratia spp., Proteus mirabilis, Morganella morganii) are most often isolated and identified.
To evaluate the results of microscopic and cultural examinations, a comprehensive system for identifying disorders of the vaginal microflora is used (“Integral assessment of the state of the vaginal microbiota. Diagnosis of opportunistic infections”, Ankirskaya A.S., Muravyova V.V., 2011).
3. Real-time polymerase chain reaction (PCR) is one of the most accurate molecular biological methods for studying microbiota, which makes it possible to objectively study the amount of opportunistic and normal vaginal microflora, the degree and nature of the imbalance, as well as monitor the effectiveness of treatment.
Consultations with other medical specialists (endocrinologist, gastroenterologist) are recommended in case of frequent recurrence of AV in order to exclude concomitant diseases (conditions) that may contribute to disruption of the normal vaginal microbiota.
DIFFERENTIAL DIAGNOSTICS
Differential diagnosis of AV must be carried out with other urogenital diseases caused by pathogenic (N. gonorrhoeae, T. vaginalis, C. trachomatis, M. genitalium) and opportunistic microorganisms (yeast-like fungi of the genus Candida, genital mycoplasmas, anaerobic microorganisms), anogenital herpes virus infection. The algorithm for differential diagnosis of AV and bacterial vaginosis is presented in Table. 3.
TREATMENT
Indications for treatment
The indication for treatment is the diagnosis of AV, established on the basis of a clinical examination and laboratory tests. Treatment of asymptomatic AV, identified by microscopic examination of vaginal discharge, must be carried out before the introduction of intrauterine devices; before surgical interventions on the pelvic organs, including medical abortions; pregnant women with a history of premature birth or late miscarriages.
If sexual partners have clinical signs of balanoposthitis, urethritis and other diseases of the urogenital system, it is advisable to examine them and, if necessary, treat them.
Treatment Goals
- clinical recovery;
- normalization of laboratory parameters;
- prevention of the development of complications associated with pregnancy, fetal pathology, the postpartum period, the postoperative period and the performance of invasive gynecological
- logical procedures.
General notes on therapy
The main direction in the treatment of AV should be the elimination of an increased number of aerobic microorganisms, which is achieved through the use of etiotropic drugs.
Local therapy. The drugs of choice for local treatment are non-absorbable broad-spectrum antibacterial drugs that act on intestinal gram+ and gram- aerobes: a combination drug of neomycin sulfate 35,000 IU, polymyxin B sulfate 35,000 IU, nystatin 100,000 IU (Polygynax) and clindamycin.
The combined drug: neomycin sulfate 35,000 IU, polymyxin B sulfate 35,000 IU, nystatin 100,000 IU has a wide spectrum of antimicrobial action against AV pathogens, has a pronounced anti-inflammatory effect and helps reduce symptoms of the disease from the first days of treatment. Unlike medications containing glucocorticosteroids, this drug does not have an immunosuppressive effect on local immunity and promotes rapid restoration of the number of lactobacilli and the functional activity of the vaginal epithelium. Intravaginal use of the drug Polygynax allows you to avoid systemic effects on the body, and also makes it possible to prescribe the drug to pregnant women (with the exception of the first trimester). These features of the drug help achieve an optimal therapeutic effect, which is especially important in the presence of mixed bacterial and fungal infection.
Clindamycin for local use is convenient to use both in outpatient and inpatient practice, provides satisfactory compliance and good tolerability in combination with pronounced therapeutic efficacy.
Povidone-iodine (Betadine) in the form of a solution (for douching) or vaginal suppositories promotes faster relief of symptoms due to its pronounced antiseptic effect, activity against antibiotic-resistant strains of bacteria and its own prebiotic effect: povidone-iodine increases the acidity of the vaginal environment, which leads to the rapid creation optimal conditions for restoring normal vaginal microflora.
Short-term use of topical glucocorticosteroid drugs in addition to antibacterial therapy is indicated only for desquamative inflammatory vaginitis.
Treatment of AV may include topical application of estriol or estradiol in cases where the clinical picture is dominated by atrophic changes (increased number of parabasal cells).
Systemic therapy. In severe cases of AV, treatment with systemic antibacterial drugs and local drugs is recommended.
Indications for the use of systemic antibacterial drugs:
- frequent relapses of AV with severe course;
- resistance and ineffectiveness of local treatment;
- the presence of concomitant infectious diseases.
Indications for hospitalization
None.
Recommended treatment regimens
Local therapy
combination drug: neomycin sulfate 35,000 IU, polymyxin B sulfate 35,000 IU, nystatin 100,000 IU, vaginal capsules intravaginally 1 time per day before bedtime for 12 days,
or
clindamycin, cream 2%, 5.0 g intravaginally 1 time per day, preferably before bedtime for 3–7 days, for desquamative inflammatory vaginitis up to 4–6 weeks,
or
povidone-iodine, intravaginal suppositories daily before bedtime, for 10–14 days,
or
dequalinium chloride 10 mg, vaginal tablets, intravaginally daily before bed, for 6 days.
Systemic antibacterial drugs
ofloxacin 200–400 mg 2 times a day for 7–10 days,
or
ciprofloxacin 125–500 mg 2 times a day, in more severe cases – up to 750 mg 2 times a day for 7–14 days,
or
levofloxacin 500 mg 1–2 times a day for 7–14 days,
or
amoxicillin 500 mg 3 times a day; in case of severe infection, the dose can be increased to 1.0 g 3 times a day for 7–10 days,
or
amoxicillin/clavulanate 500 mg+125 mg 3 times a day for 7–10 days.
Evaluation of treatment effectiveness
- clinical recovery;
- normalization of laboratory parameters.
It is recommended to establish cure 14 days after the end of treatment.
Tactics in the absence of treatment effect
Prescription of other drugs or treatment methods.
Causes of colpitis
The main causes of colpitis include:
- unreliable contraception (or lack thereof)
- poor intimate hygiene
- frequent change of sexual partners
- intestinal microflora disorders
- endocrine pathologies
- allergic reactions to condoms or medications
- mechanical damage to the vaginal mucosa (trauma)
- abuse of antiseptics and antibiotics
- self-prescription of contraceptives
- urological and gynecological diseases
- wearing tight synthetic underwear
Atrophic vaginitis. Atrophic colpitis
Atrophy of the vaginal mucosa (atrophic vaginitis, atrophic colpitis) is a gradually increasing thinning of the epithelium of the vaginal walls, dryness of the mucous membrane of the vagina and vulva, directly related to estrogen saturation of tissues.
It occurs in more than 90% of women as a result of natural aging. Early manifestation of signs of mucosal dystrophy significantly reduces a woman’s quality of life and is a source of chronic stress and depression.
Atrophy of the vaginal mucosa (atrophic colpitis, atrophic vaginitis) manifests itself in the form of itching, burning, a feeling of dryness, sensitivity during mechanical friction (sexual intercourse), the presence of leucorrhoea and atypical discharge from the vagina, the appearance of microtraumas and, in some cases, bleeding. Many women, experiencing pain during and after sexual intercourse, significantly lose interest in sex. In addition, since the normal functioning of the reproductive system is closely intertwined with the functioning of the urinary system, atrophy of the vaginal mucosa can cause urological diseases.
The main causes of the disease are a decrease in estrogen levels during physiological or surgical menopause (after removal of the ovaries and uterus). Insufficient blood supply to the vaginal walls leads to a decrease in vaginal secretion, smoothing of folds, changes in the composition of the microflora and an increase in vaginal pH, thinning of the mucous layer.
IntimaLase technology
allows us to solve this problem: the thermal effect of the laser ensures the formation of new microvasculature vessels in the mucous and submucosal layer of the vaginal wall. Restoration of active blood supply leads to restoration of the mucous membrane and normalization of metabolic processes in tissues, natural folding is restored.
IntimaLase laser technology
, is never opposed to hormone replacement therapy.
In mild, initial forms of mucosal atrophy, IntimaLase
makes it possible to restore the normal functioning of the mucous membrane, and in more severe forms, laser therapy is used as an additional method of treatment.
IntimaLase
technology allows you to reduce the dose of hormonal drugs and increases the quality and results of treatment.
Cabinet of laser and radio wave medicine
Symptoms of vaginitis
The first signs of vaginal colpitis in women become noticeable in the early stages. Typically, patients complain of the following symptoms:
- presence of vaginal discharge
- itching and burning in the perineal area
- swelling and redness of the vulva
- pain and discomfort during intercourse or urination
- unpleasant sour smell
- psychological and nervous disorders
- insomnia, anxiety, irritability
- frequent urge to urinate
- urinary incontinence