Heart failure (HF) is a pathological condition caused by the failure of the heart as a pump that provides adequate blood circulation. Manifestation and consequence of pathological conditions affecting the myocardium or complicating the work of the heart: coronary heart disease, heart defects, arterial hypertension, diffuse lung diseases, myocarditis, myocardial dystrophy (including thyrotoxic, sports, etc.), myocardiopathy (including alcoholic) and etc.
Acute heart failure can be either acute itself, or it can be an acute manifestation of chronic heart failure.
What it is
Coronary insufficiency (CI) is a condition in which blood flow through the coronary (coronary) arteries does not meet the energy needs of the heart. In this case, myocardial ischemia occurs - damage to heart cells due to lack of oxygen and nutrients. Ischemia is a local process that occurs in the place of the myocardium (heart muscle) where its nutrition has been disrupted. The process of deterioration of blood flow itself is most often explained by a narrowing of the lumen of the blood-bearing vessel. Globally this can happen for 2 reasons:
- obstruction (blockage) of the artery lumen;
- spasm due to contraction of the vessel walls.
A combination of these reasons is also possible.
In this case, a person cannot notice any changes in his condition until the level of stenosis (narrowing of the lumen of the artery) reaches critical values. Or until the need of the heart for nutrition makes the stenosis significant. When these conditions are met, ischemia develops in the area of the heart muscle—an attack of angina, myocardial infarction, or even sudden cardiac death occurs. Thus, we can say that clinically coronary insufficiency manifests itself in various forms of coronary heart disease (CHD).
According to research, the number of patients with coronary artery disease in Russia exceeds 7.5 million people - this is a very high figure. Moreover, the prevalence among people of retirement age is 16% higher than among people of working age. That is, the incidence of the disease progresses with age. Men get sick earlier and more often than women.
What classes is heart failure divided into?
There are several classifications of heart failure:
- Classification according to V. Kh. Vasilenko, N. D. Strazhesko, G. F. Lang;
- Classification of acute heart failure according to the Killip scale;
- And the most common is the New York Heart Association classification.
According to the New York Heart Association (NYHA) functional classification, heart failure is classified into classes I-IV depending on the severity of symptoms and limitation of physical activity.
Heart failure is divided into four classes depending on the severity of symptoms:
- NYHA I: heart disease without any restrictions on physical activity. Normal activity does not cause increased fatigue, palpitations, or difficulty breathing.
- NYHA II: Heart disease causing moderate limitation in daily activities. No symptoms at rest.
- NYHA III: Heart disease causing marked limitation in daily activities. Simple activities such as brushing your teeth, eating, or talking cause fatigue, palpitations, or difficulty breathing. There are no symptoms at rest.
- NYHA IV: Heart disease that causes symptoms at rest (and with any degree of light physical activity).
Heart failure significantly reduces quality of life. Patients often experience great frustration with physical limitations and tend to withdraw from social life. For this reason, psychological disorders such as depression are often present in addition to the expected physical symptoms.
Causes
Coronary insufficiency most often occurs due to obstruction or spasm of the coronary vessels of the heart or their branches. Let's take a closer look at each of these cases, as well as several more rare situations.
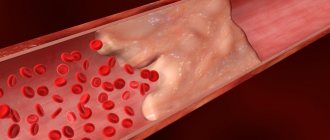
The image is a coronary angiography of the heart vessels. Source: Image by Mario Ohibsky from Pixabay
Artery obstruction
The most important and common cause of coronary insufficiency is atherosclerosis of the coronary arteries. Atherosclerotic plaques protrude into the lumen of the vessel and obstruct blood flow. In this case, chronic coronary insufficiency develops, which most often makes itself felt by attacks of angina pectoris.
Atherosclerotic plaques can also break off or contribute to damage to the inner surface of the vessel and thus provoke thrombosis, which will cause acute coronary insufficiency. Its most common manifestation is myocardial infarction. More information about atherosclerosis can be found here.
Artery spasm
Coronary insufficiency also occurs due to a sharp and prolonged spasm of the coronary arteries. Severe stress, mental and physical overload can lead to this. Often the listed factors complement the existing atherosclerotic lesion of the vessel, which results in angina pectoris or myocardial infarction. However, purely spastic coronary insufficiency is also possible.
Other reasons
There are other, more rare, causes of impaired blood supply to the myocardium:
- Congenital anomalies of the coronary vessels;
- Hypertrophic cardiomyopathy is a condition in which the existing vessels are not enough to meet the needs of the enlarged myocardium (a consequence of hypertension);
- Neoplasms in the chest, compressing blood vessels from the outside (tumor).
Risk factors
Some factors increase the risk of coronary artery disease:
- Male gender and age over 45 years are factors that cannot be adjusted in any way.
- Smoking affects both the development of atherosclerosis and the processes of thrombus formation. Cigarette smoke contains nicotine and carbon monoxide, which have a negative effect on the functioning of the cardiovascular system.
- Low physical activity, a sedentary lifestyle, excess weight and obesity contribute to thrombosis, atherosclerosis, and hypertension, which can lead to coronary insufficiency.
- Eating large amounts of food high in fat and cholesterol contributes to atherosclerosis.
- Chronic stress provokes prolonged spasm of the coronary arteries.
- Heredity - the risk of developing pathology is higher if relatives have it.
Diagnosis of coronary heart failure
In most cases, even after a visual examination of the patient, the doctor may suspect the development of acute coronary insufficiency. But to confirm the diagnosis, it is necessary not only to take into account the totality of clinical signs caused by coronary insufficiency, but also to conduct a diagnostic examination, which includes:
- Complete blood count (the main indicator is an increased number of red blood cells, indicating the presence of an inflammatory process in the body).
- Biochemical blood test (allows us to understand the cause of the disease).
- Blood test for clotting (the consistency of the blood flow and the tendency to thrombosis are studied).
- Coronary angiography (the main diagnostic method aimed at assessing the condition of the coronary arteries).
- X-ray, ultrasound of the chest (allows you to determine whether the patient has other possible diseases of the cardiovascular system and determine the cause of coronary insufficiency).
- Electrocardiography (makes it possible to judge the health of the contractile function of the myocardium and the work of the heart).
- Computed tomography (aimed at identifying stenosis of the coronary arteries, atherosclerotic plaques of different sizes).
- Magnetic resonance imaging of the heart (allows you to take pictures in different planes, measure arterial blood flow, study the filling of the ventricles and atria).
Symptoms
Symptoms of coronary artery disease may vary from case to case. It is also not uncommon for patients to feel nothing strange about their condition until one day, for example, a myocardial infarction occurs.
Among the most characteristic symptoms of coronary insufficiency are:
Angina pain is a pressing, squeezing, burning pain behind the sternum lasting up to 10 minutes. Often appear during physical activity. May begin behind the sternum and then spread to the neck, back, shoulders, arms, jaws;
- Dizziness;
- Cold sweat;
- Pain in the stomach;
- Shortness of breath, especially with exertion;
- Sleep disorders;
- Weakness.
Important! If you notice such symptoms, especially against the background of unusual physical activity, you should immediately call an ambulance. This should also be done if angina has already been diagnosed, but the symptoms are not relieved by nitroglycerin and last longer than 15 minutes.
Source: Pavel Danilyuk: Pexels
The listed symptoms are characteristic of a chronic (reversible) version of coronary insufficiency, which manifests itself as angina pectoris. In the acute (irreversible) version, the described symptoms are more pronounced and last much longer - up to several days (with myocardial infarction). The pain is not relieved by nitroglycerin and can be so severe that it is necessary to resort to narcotic drugs.
Despite the fact that the main symptom of a heart attack is most often severe chest pain (80% of cases), there are other manifestations of the disease:
- Cough and shortness of breath;
- Sharp pain in the upper abdomen;
- Symptoms of brain damage.
An asymptomatic form of myocardial infarction is rare. The area of damage in the heart is not so extensive, and changes are recorded instrumentally after the fact.
Symptoms of chronic and acute coronary heart failure
Among the main signs of coronary insufficiency syndrome:
- cardiopalmus;
- pallor of the skin, the appearance of drops of sweat on the forehead;
- severe pain in the chest, paroxysmal in nature;
- shortness of breath that occurs for unknown reasons;
- chest pain;
- attacks of angina/tachycardia;
- dry cough.
Symptoms worsen after doing physical work, overeating, climbing stairs, emotional experiences (panic, fear). It can also worsen during the resting stage.
Some patients with coronary insufficiency experience:
- nausea;
- vomit;
- frequent urge to urinate;
- flatulence.
If you notice similar symptoms, consult a doctor immediately. It is easier to prevent a disease than to deal with the consequences.
Chronic form
A typical manifestation of chronic coronary insufficiency is angina. Most often it is caused by atherosclerotic damage to the coronary arteries of the heart, which causes a narrowing of their lumen. During physical activity, the myocardium requires more blood, while the permeability of the artery is reduced - ischemia occurs with characteristic symptoms.
When attacks are predictable and repeated in response to a load of the same severity, they speak of a stable version of angina. Its course is relatively favorable and can be easily controlled. There are other options:
- Unstable angina is a form of angina in which a plaque in a coronary vessel undergoes ulceration, a thrombus gradually grows in the lumen, causing attacks to constantly progress and ultimately lead to myocardial infarction.
- Prinzmetal's angina (vasospastic angina) - occurs as a result of a sudden spasm of the coronary arteries.
We wrote about angina in more detail here.
Until this point, we were talking mostly about absolute coronary insufficiency, when the direct cause of the pathological condition was pathological processes in the coronary vessels. But there is also a relative form that occurs against the background of hypertrophic cardiomyopathy, which was discussed in the causes of coronary insufficiency. During this process, the myocardium increases in size due to the increased load, while new vessels do not appear. In this case, ischemia of poorly supplied areas also develops.
Coronary insufficiency - what is it?
- Acute coronary heart failure. It is characterized by a discrepancy between the blood flow and the metabolic needs of the myocardium (in parallel, altered coronary arteries of the heart can be diagnosed, angina attacks, severe heart rhythm disturbances, and ECG changes can be observed). The disease, which occurs in an acute manner, often provokes the development of myocardial infarction.
- Chronic coronary insufficiency. It is characterized by prolonged (constant) insufficient blood supply to the myocardium. A prerequisite for the occurrence of pathology is a change in the coronary bed.
Also, coronary heart failure can occur in:
- absolute form (blood flow through the coronary vessels is sharply limited);
- relative form (myocardial oxygen demand increases significantly, but there are no restrictions on coronary blood flow).
Sudden coronary death
Sudden coronary death (SCD) is said to occur when a person dies within no more than 6 hours against the background of apparent well-being due to a cardinal malfunction of the heart. At the same time, the patient loses consciousness and falls.
As a rule, the immediate cause of VCS is ventricular tachycardia and ventricular fibrillation. These are severe rhythm disturbances in which the efficiency of myocardial contraction decreases so much that blood does not flow to vital organs in sufficient volume.
WHO recommends at least 150 minutes of physical activity per week to help reduce the risk of VCS. Source: Mario Ohibsky from Pixabay
However, these arrhythmias are most often preceded by a severe attack of acute coronary insufficiency. Extensive myocardial damage as a result of this attack not only in itself reduces the contractility of the ventricles of the heart, but also contributes to the occurrence of arrhythmias.
Sometimes death can be prevented with timely assistance, but this is more typical for sudden cardiac death of an arrhythmogenic nature. In this case, the developing arrhythmia is of paramount importance, and coronary causes are secondary. Patients with diabetes are at increased risk of VCS.
Important! If you see a person suddenly lose consciousness, you should call an ambulance and, if you have the appropriate skills, perform primary resuscitation measures. Cardiopulmonary resuscitation should be resorted to if you do not detect a pulse and/or breathing in the victim.
Despite this threat in patients with coronary insufficiency, with well-chosen treatment and strict adherence to doctor’s orders, the likelihood of VCS becomes significantly lower. It is also important to seek medical help in a timely manner. It is known that several weeks before an attack, patients sometimes complain of pain in the chest, worsening mood, and fatigue. This means that some treatment measures can be taken before an attack occurs.
Danger of coronary insufficiency
Coronary insufficiency can lead to two life-threatening conditions:
- unstable angina;
- myocardial infarction.
Based on the symptoms of the disease, doctors can determine how high the risk of sudden coronary death (occurs within six hours of the onset of a heart attack) is.
High risk of death if any of the following are present:
- An attack of angina lasts more than 20 minutes.
- Pulmonary edema has developed (the patient constantly stands, breathes heavily, and produces foamy pink sputum).
- The ECG shows reduced or increased ST segment elevation of more than 1 mm above the isoline.
- Angina pectoris, low blood pressure in the arteries.
- According to laboratory tests, there is a change in the level of markers of myocardial necrosis (death).
The average risk of sudden death due to coronary insufficiency is placed if any of the symptoms are observed:
- The attack lasts less than 20 minutes.
- Angina at rest - less than 20, stopped after resorption of Nitroglycerin.
- At night, attacks of chest pain constantly occur.
- The patient's age is over 65 years.
- Severe angina, the first symptoms of which appeared within the last two weeks.
- On the ECG, Q waves are more than 3 mm, dynamic changes in the T wave to normal levels, a decrease in the ST segment at rest.
A low risk of sudden death can be assumed if the following symptoms occur:
- Attacks occur even after simple physical work.
- Recently, the attacks have become more frequent and severe.
- Angina first appeared two weeks to two months ago.
- There are no new changes on the ECG (compared to the results that were obtained previously) or a normal curve for the patient’s age is observed.
Diagnostics
Signs of coronary insufficiency can be suspected independently by detecting symptoms of angina pectoris, although an asymptomatic course up to myocardial infarction is not uncommon.
The following diagnostic methods are used in clinical practice:
- Coronary angiography is the gold standard in diagnosing cardiac vascular pathology; it allows one to visualize narrowing of the lumen in the coronary arteries and their obstruction. The technique is invasive - a catheter for administering a contrast agent is placed through the radial or femoral artery, so the study is performed in the operating room under local anesthesia.
- Optical coherence tomography of the coronary arteries is one of the new and accurate methods for visualizing problem areas in the coronary vessels of the heart. The method is also invasive and is performed in a similar manner to coronary angiography.
- Various types of echocardiography (Echo-CG) allow visualization of areas of the myocardium with impaired contractility, as well as many associated disorders.
- Myocardial scintigraphy - allows you to identify areas of the myocardium with impaired blood circulation, for which special radionuclides are used.
- Stress tests (treadmill test, bicycle ergometry) - procedures allow you to evaluate ECG changes indicating myocardial ischemia during physical activity.
Blood samples are also examined, paying attention to:
- Lipidogram - determination of cholesterol and the ratio of lipids in the blood to identify predisposition to coronary artery disease.
- Blood glucose - to exclude diabetes mellitus.
- Determination of the level of red blood cells and hemoglobin - to exclude iron deficiency anemia.
- Biochemical markers - study the levels of various enzymes that may indicate a heart attack.
Important: elevated blood cholesterol levels can significantly increase the risk of atherosclerotic plaques. They can become one of the causes of coronary insufficiency. Cholesterol may be too high due to a high intake of low-density lipoprotein (LDL) and low intake of high-density lipoprotein (HDL). A nutritionist will help you adjust your diet so that there are more “good”, low-density foods than “bad” foods.
Risk group for the development of cardiac coronary insufficiency
Most often, coronary heart failure is diagnosed in people:
- with a hereditary predisposition;
- with obesity;
- who smoke a lot;
- who have elevated blood cholesterol levels;
- people with diabetes;
- those engaged in sedentary work and leading a sedentary lifestyle;
- suffering from arterial hypertension.
When several risk factors are combined, the likelihood of developing blood clots increases significantly. This means that it is impossible to 100% exclude the occurrence of sudden coronary death in the patient in the future.
Treatment
When prescribing treatment, a cholesterol-lowering diet, moderate regular physical activity and weight loss are first recommended. If you have bad habits, you need to get rid of them. This is called lifestyle modification. Do not underestimate the benefits of such recommendations; in this case, they largely determine the success of treatment and the prevention of future complications.
Source: Michal Jarmoluk from Pixabay
Pathogenesis
The mechanism of formation of coronary vascular insufficiency is determined by the interaction of a number of factors:
- presence of atherosclerotic plaque ;
- spasm of the coronary arteries;
- extracoronary thrombosis.
It is known for certain that the appearance of an atherosclerotic plaque is the morphological basis of ischemic myocardial damage in 90% of cases. Severe attacks of angina occur when the coronary vessels are damaged by 70-80%. When an artery spasms, a contraction of the smooth muscle vascular wall occurs, which creates an obstacle to normal blood flow in the myocardium. Coronary artery spasm is influenced by the sympathetic nervous system .
Thrombosis is of utmost importance . Thrombi form mainly on the surface of an atherosclerotic plaque at the site of disruption of the integrity and structure of the endothelial layer in the form of destruction and ulceration of the plaque.
Drug treatment
Drug treatment includes several groups of drugs:
- Beta blockers and calcium antagonists - these two groups reduce myocardial oxygen consumption and promote dilation of coronary vessels. These drugs are also effective for common concomitant conditions (hypertension and arrhythmias).
- Statins are drugs that help normalize the lipid profile of the blood. Prevents the growth of atherosclerotic plaques.
- Antiplatelet drugs - reduce the risk of coronary artery thrombosis by preventing blood clotting.
- Nitrates - this group of drugs eliminates the symptoms of angina attacks.
Stages of the disease
Stages of development and severity of congestive heart failure. Of the numerous signs of heart failure listed when describing a particular stage, it is necessary to highlight a few, each of which is sufficient to determine a specific stage. Stage I: Subjective symptoms of heart failure during moderate or greater exercise.
Stage IIA:
- pronounced subjective symptoms of heart failure with light loads;
- orthopnea;
- attacks of suffocation;
- radiographic, and in some cases, electrocardiographic signs of secondary pulmonary hypertension;
- reappearance of edema;
- re-enlargement of the liver;
- cardiomegaly without other signs of this stage;
- atrial fibrillation without other signs of this stage.
Stage IIB:
- repeated attacks of cardiac asthma;
- persistent peripheral edema;
- significant abdominal edema - permanent or reoccurring;
- persistent enlargement of the liver, which may shrink during treatment, but remains enlarged;
- atriomegaly;
- cardiomegaly in combination with at least one of the signs of the previous stage;
- atrial fibrillation in combination with at least one of the signs of the previous stage.
Stage III, terminal:
- severe subjective disorders with minimal exertion or at rest;
- repeated episodes of cardiac asthma during the week;
- dystrophic changes in organs and tissues.
If there is at least one sufficient sign of a more severe stage, then this stage should be established. Priority is given to clinical criteria. Negative results of instrumental studies often turn out to be inconclusive. The most obvious final manifestations of heart failure, such as a decrease in cardiac output, insufficient blood supply to organs and tissues and insufficient supply of oxygen to them, may be absent not only at rest, but also with the load available to the patient. Like blood pressure, the corresponding indicators may not go beyond the wide range of normal variants even in severe heart failure - until the last days and hours of the patient’s life (compensation at the pathological level).
Surgery
Surgical treatment is resorted to when the level of blood flow disturbance in the coronary arteries becomes critical and cannot be compensated for with medication. In this case, we are talking about two operations: coronary artery bypass grafting (CABG) and coronary artery stenting.
Coronary artery bypass grafting is an open operation in which access to the heart is achieved through opening the chest. The idea is to restore blood flow in the coronary artery after the site of narrowing. This is accomplished by connecting the affected artery and a healthy large vessel through another vessel, forming a kind of “bypass bridge” for the flow of blood. The necessary connecting vessel (shunt) can be taken from the lower leg, forearm and other places.
It is important to know that the rehabilitation period is long due to the long fusion of the sternum. Although the operation is complex, it has been practiced in Russia for a long time and, as a rule, goes well.
Coronary artery stenting is a minimally invasive operation in which a narrowed section of a coronary artery is expanded from the inside using a special metal mesh. The heart is most often accessed through the femoral artery of the leg. This surgical intervention is easy and has virtually no recovery period.
Diagnosis and treatment of acute coronary syndrome: from understanding principles to implementing standards
Definition
As defined in the 2000 American College of Cardiology and American Heart Association guidelines, acute coronary syndrome includes any group of symptoms suggestive of acute myocardial infarction (MI) or unstable angina (UA). The main clinical variants of ACS include:
- MI with ST segment elevation;
- Non-ST segment elevation MI;
- MI diagnosed by enzyme changes or biomarkers;
- MI diagnosed by late ECG signs;
- NS.
It should be emphasized that the diagnosis of ACS is temporary, “working” and is used to identify a category of patients with a high probability of MI or NS at the first contact with them. Treatment of patients with ACS begins before obtaining information necessary and sufficient to confidently make a nosological diagnosis. After identifying any of the above clinical conditions, therapy is adjusted based on the results of diagnostic tests.
Pathogenesis
The leading pathogenetic mechanism of ACS is thrombosis of the coronary artery affected by atherosclerosis
. A thrombus forms at the site of rupture of an atherosclerotic plaque. The likelihood of plaque rupture depends on its location, size, consistency and composition of the lipid core, the strength of the fibrous capsule, as well as the severity of the local inflammatory reaction and tension of the vessel wall. The immediate causes of damage to the plaque shell are the mechanical effects of blood flow and the weakening of the fibrous capsule under the influence of proteolytic enzymes secreted by macrophages. The contents of the plaque are characterized by high thrombogenicity - its effect on the blood leads to a change in the functional properties of platelets and the launch of the coagulation cascade. A certain role in the development of ACS is played by spasm of the coronary artery at the location of the damaged plaque. In cases where obstruction of the patency of the coronary artery is caused by its spasm and/or the formation of a platelet aggregate (that is, it is reversible), the clinical picture of NS develops. The formation of a red thrombus that does not completely block the lumen of the vessel leads to the development of MI without a Q wave. With complete thrombotic occlusion of the coronary artery, an MI with a Q wave is formed.
Diagnostics
Recognition of ACS is based on three groups of criteria. The first group consists of signs determined during questioning and physical examination of the patient, the second group - data from instrumental studies, and the third - results of laboratory tests.
Typical clinical manifestations of ACS are anginal pain
at rest for more than 20 minutes, first-time angina of functional class III, progressive angina. Atypical manifestations of ACS include varied pain in the chest that occurs at rest, epigastric pain, acute digestive disorders, pain characteristic of pleural damage, and increasing shortness of breath. Physical examination of patients with ACS often does not reveal any abnormalities. Its results are important not so much for the diagnosis of ACS, but for detecting signs of possible complications of myocardial ischemia, identifying heart diseases of a non-ischemic nature and determining extracardiac causes of the patient’s complaints.
The main method of instrumental diagnosis of ACS is electrocardiography
. The ECG of a patient with suspected ACS should, if possible, be compared with data from previous studies. In the presence of appropriate symptoms, NS is characterized by ST segment depression of at least 1 mm in two or more adjacent leads, as well as T wave inversion with a depth of more than 1 mm in leads with a predominant R wave. Developing MI with a Q wave is characterized by persistent ST segment elevation , for Prinzmetal's angina and developing MI without a Q wave – transient ST segment elevation (Fig. 1). In addition to the usual resting ECG, Holter monitoring of the electrocardiosignal is used to diagnose ACS and monitor the effectiveness of treatment.
Rice. 1. Variants of ACS depending on ECG changes
Of the biochemical tests used to diagnose ACS,
the determination of the content of cardiac troponins T and I in the blood
, an increase in which is the most reliable criterion of myocardial necrosis.
A less specific, but more accessible criterion for determination in clinical practice is an increase in the blood level of creatine phosphokinase (CPK) due to its isoenzyme MB-CPK. An increase in the content of MB-CPK (preferably mass rather than activity) in the blood by more than twice as compared to the upper limit of normal values in the presence of characteristic complaints, ECG changes and the absence of other causes of hyperenzymemia allows one to confidently diagnose MI. An increase in the level of MB-CPK and cardiac troponins is recorded 4–6 hours after the onset of formation of a focus of myocardial necrosis. The earliest biomarker of MI is myoglobin
- its content in the blood increases 3-4 hours after the development of MI. To rule out or confirm the diagnosis of MI, repeat blood tests are recommended within 6 to 12 hours after any episode of severe chest pain. The listed tests become especially important in the differential diagnosis of MI without a Q wave and NS.
Traditional biomarkers of myocardial necrosis, such as aspartic aminotransferase, lactate dehydrogenase, and even total CPK, due to insufficient sensitivity and specificity, are not recommended for the diagnosis of ACS. In practical healthcare conditions, the funds spent on the purchase of reagents for their determination should be directed to the implementation of recommended diagnostic tests.
Risk assessment
During the first 8–12 hours after the onset of clinical symptoms of ACS, it is necessary to ensure the collection of diagnostic information in a volume sufficient for risk stratification. Determining the degree of immediate risk of death or development of MI is fundamentally important for choosing treatment tactics for a patient with ACS without persistent ST segment elevation.
Criteria for a high immediate risk of death and MI include:
repeated episodes of myocardial ischemia (repeated anginal attacks in combination or without combination with transient depression or ST segment elevation);
increase in the content of cardiac troponins (if it is impossible to determine - MV-CPK) in the blood; hemodynamic instability (arterial hypotension, congestive heart failure); paroxysmal ventricular disturbances of heart rhythm (ventricular tachycardia, ventricular fibrillation); early post-infarction angina. Signs of a low immediate risk of death and development of MI are:
absence of repeated attacks of chest pain; absence of depression or elevation of the ST segment - changes only in the T wave (inversion, decrease in amplitude) or normal ECG; no increase in the content of cardiac troponins (if it is impossible to determine them - MV-CPK) in the blood.
to perform a stress test 3–5 days after an episode with ACS symptoms
.
In patients with a high immediate risk of developing MI and death, conducting a stress test to assess the prognosis and determine treatment tactics is considered possible no earlier than 5–7 days after stable stabilization of the condition. If silent myocardial ischemia is suspected, a stress test should be preceded by Holter ECG monitoring. A standard stress test involves recording an ECG during physical activity on a bicycle ergometer or treadmill. In some patients, the exercise test may not be informative enough. In these cases, it is possible to perform stress echocardiography with physical activity
. Pharmacological stress tests using echocardiography or myocardial scintigraphy are indicated in patients who have limitations in physical activity.
The criteria for a high risk of an unfavorable outcome, determined by the results of stress tests, include: the development of myocardial ischemia with low tolerance to physical activity; extensive stress-induced perfusion defect; multiple stress-induced small perfusion defects; severe left ventricular dysfunction (ejection fraction less than 35%) at rest or during exercise; stable or stress-induced perfusion defect in combination with left ventricular dilatation.
Patients classified as high risk based on clinical signs, instrumental and laboratory tests, as well as patients with UA who have previously undergone coronary balloon angioplasty (CBA) or coronary artery bypass grafting (CABG) are indicated for coronary angiography.
. The results of the latter are the basis for the choice of further treatment tactics for the patient - in particular, assessing the feasibility of performing and determining the type of myocardial revascularization operation. In patients with persistently recurrent pain syndrome and severe hemodynamic instability, coronary angiography is recommended to be performed as soon as possible after the onset of clinical symptoms of ACS without prior stress tests.
Drug treatment
Taking into account ideas about the mechanisms of development, the main direction of pathogenetic therapy for ACS should be considered the effect on the blood coagulation system
. The drugs that influence the process of thrombus formation include three groups of drugs: thrombolytics, anticoagulants and antiplatelet agents.
Thrombolytic therapy (TLT)
The indication for TLT is anginal pain lasting more than 30 minutes, persisting despite taking nitroglycerin, in combination with an elevation of 1 mm or more in the ST segment in at least 2 adjacent ECG leads or the appearance of a complete block of the left bundle branch. Analysis of the results of placebo-controlled studies (GISSI-1, ISIS-2, ASSET, LATE) showed that TLT performed in the first 6 hours after the onset of clinical symptoms of developing MI reduces mortality during the first month after the development of MI by an average of 30% . Carrying out TLT within 6–12 hours from the onset of anginal pain reduces mortality by an average of 20% and is considered acceptable in the presence of clinical and ECG signs of expansion of the zone of myocardial necrosis. TLT performed later than 12 hours from the onset of MI does not have a positive effect on mortality. In the absence of persistent ST segment elevation, which is considered a sign of blockage of the coronary artery by a fibrin-containing thrombus, the use of TLT is also inappropriate.
Absolute contraindications to TLT are a history of hemorrhagic stroke, ischemic stroke or dynamic cerebrovascular accident within the last year, intracranial tumor, active internal bleeding, dissecting aortic aneurysm.
GUSTO Study
alteplase
administration is the best thrombolytic therapy strategy currently available for patients with MI.
The scheme for accelerated administration of alteplase (100 mg) for MI within 6 hours from the onset of symptoms with a body weight of more than 65 kg is as follows: 15 mg alteplase bolus over 1-2 minutes, then 50 mg intravenous infusion over 30 minutes. and then 35 mg over 60 minutes. Before starting, intravenous administration of heparin 5000 IU + intravenous infusion of heparin 1000 IU/hour in the next two days.
Anticoagulants
Of the compounds belonging to this pharmacological group, unfractionated heparin is mainly used in the treatment of patients with ACS.
(NFG). Unlike thrombolytic agents, UFH is administered not only to patients with persistent ST segment elevation, but also to patients with other types of ACS. The main contraindications to heparin therapy are active bleeding and diseases accompanied by a high risk of its occurrence.
The regimen for administering UFH to patients with ACS without persistent ST segment elevation: intravenous – bolus 60–80 U/kg (but not more than 5000 U), then infusion 12–18 U/kg/h (but not more than 1250 U/kg/h) within 48 hours. The optimal rate of heparin administration is determined by the value of the activated partial thromboplastin time (aPTT). The use of blood clotting time for this purpose is not recommended. A condition for the effectiveness of heparin therapy is considered to be an increase in aPTT by 1.5–2.5 times compared to the normal value of this indicator for the laboratory of a given medical institution. APTT is recommended to be determined 6 hours after the start of the infusion and then 6 hours after each change in the rate of heparin administration. If the APTT remains within the desired range after two consecutive determinations, the next analysis can be performed 24 hours later. Determining APTT before starting heparin therapy is not necessary.
In cases of ACS with persistent ST segment elevation, in the absence of contraindications, heparin is indicated for all patients who have not received TLT, as well as for patients who are scheduled for myocardial revascularization. UFH is recommended to be administered subcutaneously at 7500–12500 units 2 times a day or intravenously. The recommended duration of heparin therapy when administered subcutaneously is 3–7 days. The intravenous route of administration of UFH is preferable for patients with an increased risk of thromboembolic complications (extensive MI, anterior localization of MI, atrial fibrillation, history of thromboembolism, documented thrombus in the left ventricle).
The advisability of using UFH in combination with TLT is disputed. According to modern concepts, if thrombolysis is carried out with nonspecific fibrinolytic drugs (streptokinase, anistreplase, urokinase) against the background of the use of acetylsalicylic acid in a full dose, the administration of heparin is not necessary. When using alteplase, intravenous heparin is considered justified. Heparin is administered intravenously as a bolus of 60 units/kg (but not more than 4000 units), then at a rate of 12 units/kg/h (but not more than 1000 units/kg/h) for 48 hours under the control of aPTT, which should exceed the control level 1.5–2 times. It is recommended to start heparin therapy simultaneously with the administration of alteplase. The presence of criteria for a high risk of developing thromboembolic complications is considered as an indication for heparin therapy in patients who underwent thrombolysis, regardless of the type of thrombolytic drug.
Low molecular weight heparins (enoxaparin, fraxiparin) have a number of advantages over UFH: these drugs have a longer duration of action and a more predictable anticoagulant effect, are administered subcutaneously in a fixed dose, without requiring the use of an infusion pump and laboratory control. FRIC Research Results
,
FRAXIS
,
TIMI 11B
showed that low molecular weight heparins have no less, but no greater, ability than UFH to reduce the risk of MI and death in patients with UA and non-Q wave MI. Only enoxaparin, according to the
ESSENCE
, is stronger than UFH reduced the risk of developing the total number of “coronary events” (death, MI, recurrent angina) and the frequency of emergency myocardial revascularization operations. The combined results of the ESSENCE and TIMI 11B studies confirmed the clinical benefits of enoxaparin over UFH. The duration of treatment of patients with ACS with low molecular weight heparins is on average 5–7 days. The FRIC, FRAXIS and TIMI 11B studies showed that longer use did not lead to an additional reduction in the incidence of coronary events, but increased the risk of bleeding. However, the results obtained in the TIMI 11B and FRISC II studies suggest that increasing the duration of heparin therapy may be beneficial for patients preparing for myocardial revascularization surgery.
The cost of low molecular weight heparins exceeds the cost of UFH. At the same time, their effective clinical use does not require expensive instrumental and laboratory support. If a medical institution does not have the necessary material and technical resources and is not able to provide the administration of UFH in accordance with the requirements stated above, it is recommended to use low molecular weight heparins for the treatment of patients with ACS.
In recent years, 4 large studies have been carried out (OASIS-2, ASPECT, APRICOT-2, WARIS), the results of which suggest that the prognosis of patients who have suffered ACS can be significantly improved by including the indirect anticoagulant warfarin in complex therapy. Long-term (from 3 months to 4 years) use of warfarin (in addition to acetylsalicylic acid) helped to reduce the frequency of reocclusions of the infarct-related coronary artery in patients with MI after successful TLT, reducing the risk of developing MI, cerebral stroke and death without a significant increase in the frequency of hemorrhagic complications. However, the widespread use of warfarin in the secondary prevention of coronary artery disease is limited by the need for regular monitoring of the anticoagulation effect based on the international normalized ratio.
Antiplatelet agents
The most widely used antiplatelet agent in clinical practice is acetylsalicylic acid. The drug is indicated for all types of ACS. Its use clearly reduces the risk of death and MI. Thus, according to the ISIS II study, within 35 days after the development of MI, compared with the group of patients receiving placebo, mortality in treatment with acetylsalicylic acid alone decreased by 23%, with streptokinase alone - by 25%, and acetylsalicylic acid in combination with streptokinase - by 42%. The minimum dose of acetylsalicylic acid that reduces the risk of death and MI in patients with NS is 75 mg/day.
Among the contraindications to the use of acetylsalicylic acid in clinical practice, the most common are exacerbation of peptic ulcer disease, hemorrhagic diathesis and hypersensitivity to salicylates. In cases of intolerance to acetylsalicylic acid, the use of drugs from the thienopyridine group (ticlopidine, clopidogrel) is recommended. Their main disadvantage is the slow development of the antiaggregation effect. In case of ACS, in order to accelerate the development of drug effects in the first two days of therapy, it is allowed to increase the dose of ticlopidine to 1000 mg/day, followed by a transition to the standard dose of 500 mg/day. In cases of individual intolerance or the development of side effects (allergic reactions, gastrointestinal disorders, neutropenia), ticlopidine can be replaced with clopidogrel - 300 mg once, then 75 mg/day.
The concept of combined antiplatelet therapy, that is, a simultaneous blocking effect on various pathways of platelet activation, is considered very promising. In the CURE
It has been shown that treatment of patients who have undergone non-ST segment elevation ACS with a combination of acetylsalicylic acid and clopidogrel compared with therapy with acetylsalicylic acid alone leads to a significantly more pronounced reduction in the risk of developing cardiovascular events with no difference in the number of life-threatening bleedings.
Blockers of IIb/IIIa platelet receptors have the strongest antiaggregation effect
(abciximab, eptifibatide, tirofiban, lamifiban), which are able to block platelet aggregation caused by any physiological inducer. According to numerous studies (EPILOG, EPISTENT, EPIC, CAPTURE, PRISM–PLUS, PURSUIT, PARAGON, etc.), intravenous administration of these drugs to patients with ACS without ST segment elevation in addition to acetylsalicylic acid and UFH significantly improved the results of CBA both in combination , and without combination with stent installation. Abciximab was effective only in patients who underwent myocardial revascularization, tirofiban and eptifibatide, both during revascularization and during medical treatment. Additional reductions in adverse outcomes were particularly pronounced when glycoprotein IIb/IIIa receptor antagonists were added to standard antithrombotic treatment in patients with elevated cardiac troponin levels. At the same time, long-term oral use of these drugs, according to the OPUS-TIMI and SYMPHONY studies, did not have a positive effect on the results of treatment of patients with ACS. The main indication for the use of glycoprotein IIb/IIIa receptor antagonists in patients with ACS is the absence of persistent ST segment elevation in combination with a high immediate risk of death or the development of MI during a planned myocardial revascularization procedure in the next 24 hours.
Recommended doses of glycoprotein IIb/IIIa receptor antagonists: abciximab - intravenous bolus of 0.25 mg/kg followed by infusion of 0.125 mcg/kg/min for 12–24 hours; eptifibatide – intravenous bolus of 180 mg/kg followed by infusion of 2.0 mcg/kg/min for 72–96 hours; tirofiban - intravenous infusion of 0.4 mcg/kg/min over half an hour, then 0.1 mcg/kg/min for 48–96 hours.
Nitrates
At the initial stage of treatment of patients with ACS, nitroglycerin and isosorbide dinitrate preparations are used intravenously. The initial infusion rate is 10 mcg/min. Every 3–5 minutes, the injection rate is increased by 10 mcg/min. The choice of infusion rate and rate of increase is determined by changes in the severity of pain and blood pressure (BP) levels. It is not recommended to reduce systolic blood pressure by more than 15% of baseline in normotension and by 25% in hypertension. When the desired effect is achieved, the infusion rate stabilizes and then gradually decreases. In case of excessive reduction in blood pressure, the duration of drug administration at each dosage step and the intervals between them increase. In addition to lowering blood pressure, the most common side effect that interferes with effective antianginal therapy is headache. After completion of intravenous administration, organic nitrate preparations (preferably isosorbide dinitrate or isosorbide 5-mononitrate derivatives) are administered orally according to an asymmetric scheme, ensuring a “nitrate-free” interval.
b-blockers
Drugs of this group are recommended for use in all patients with ACS in the absence of contraindications, which include bronchial asthma, severe obstructive respiratory failure, bradycardia at rest less than 50 beats per minute, sick sinus syndrome, atrioventricular block II-III degree, chronic heart failure IV functional class, severe arterial hypotension. It is preferable to start treatment with intravenous administration of beta-blockers with constant ECG monitoring
. After intravenous infusion, it is recommended to continue treatment with beta-blockers by oral administration. According to a meta-analysis of studies performed to date, long-term treatment with beta-blockers in patients who have had a Q-wave MI can reduce mortality by 20%, the risk of sudden death by 34%, and the incidence of non-fatal MI by 27%. B1-selective compounds without their own sympathomimetic activity are considered the most effective and safe.
Application regimens: propranolol
– intravenously slowly 0.5–1.0 mg, then orally 40–80 mg every 6 hours;
metoprolol
- intravenously 5 mg over 1-2 minutes three times with intervals between injections of 5 minutes, then (15 minutes after the last injection) orally 25-50 mg every 6 hours;
atenolol
- intravenously 5 mg over 1-2 minutes twice with an interval between injections of 5 minutes, then (1-3 hours after the last injection) orally 50-100 mg 1-2 times a day. The individual dose of beta-blockers is selected taking into account the heart rate, the target value of which is 50–60 beats per minute.
Calcium antagonists
Derivatives of dihydropyridine, benzodiazepine and phenylalkylamine, the most widely used representatives of which are first-generation drugs - nifedipine, diltiazem and verapamil, respectively, differ in the severity of vasodilating effects, negative inotropic and negative dromotropic effects. Meta-analyses of the results of randomized trials revealed a dose-dependent negative effect of short-acting nifedipine on the risk of death in patients with UA and MI. In this regard, short-acting dihydropyridine derivatives are not recommended for the treatment of patients with ACS. At the same time, according to some studies, long-term use of diltiazem (MDPIT, DRS) and verapamil (DAVIT II) prevents the development of recurrent MI and death in patients who have had an MI without a Q wave. In patients with ACS, diltiazem and verapamil are used in cases when there are contraindications to the use of beta-blockers (for example, obstructive bronchitis), but in the absence of left ventricular dysfunction and atrioventricular conduction disorders. Recommended doses of drugs are 180–360 mg/day.
Angiotensin-converting enzyme inhibitors
The positive effect of angiotensin-converting enzyme (ACE) inhibitors on the survival of patients who have had myocardial infarction (especially complicated by congestive heart failure) has been proven in a number of controlled studies - GISSI-3
,
ISIS-4
,
AIRE
,
SAVE
,
TRACE
, etc. Extensive MI with a pathological Q wave is an indication for the use of ACE inhibitors even in the absence of clinical and echocardiographic signs of left ventricular dysfunction. The earlier treatment with ACE inhibitors begins, the more pronounced their inhibitory effect on the process of post-infarction cardiac remodeling. On the other hand, as shown by the results of the CONSENSUS II study, which was interrupted early due to the fact that mortality in the group of patients receiving enalapril exceeded mortality in patients in the control group, ACE inhibitors should be used in the treatment of patients with MI with great caution. If possible, therapy should be started after hemodynamic stabilization in the first 48 hours from the onset of MI. The following initial doses of drugs are recommended: captopril - 25 mg/day, enalapril and lisinopril - 2.5 mg/day, perindopril - 2 mg/day. The dose should be increased gradually under the control of blood pressure and renal function. Once the optimal dose is reached, therapy should be continued for many years.
Non-drug treatment
CBA or CABG is performed in patients with recurrent myocardial ischemia to prevent MI and death. The choice of myocardial revascularization method depends on the degree, extent and localization of coronary artery stenosis, the number of affected vessels, which are determined based on the results of angiography. CABG surgery for UA and in the acute period of MI is associated with an increased risk of operative mortality. This technique of myocardial revascularization is justified in cases of damage to the trunk of the left coronary artery or multivessel disease. In patients with damage to one, or less often two vessels, myocardial revascularization is usually achieved by CBA.
As stated above, improvement in the results of CBA, as well as the coronary artery stenting procedure (EPISTENT study), can be achieved using IIb/IIIa receptor blockers. CBA is increasingly used in the treatment of patients with ST segment elevation instead of TLT. This allows not only to obtain an additional reduction in hospital mortality, but also to significantly reduce the risk of complications caused by drug effects on the blood coagulation system.
Tactics of medical care for patients with ACS
The scope of instrumental and laboratory tests, as well as the choice of methods of drug and non-drug treatment of a patient with ACS symptoms is determined by the conditions of medical care and the capabilities of a particular medical institution. A preliminary diagnosis is established based on the patient’s complaints. It should be emphasized that the absence of pathological changes on the ECG does not exclude ACS. If a connection between chest pain and acute coronary insufficiency is suspected, the patient should be urgently hospitalized - if possible, in a specialized department (ward) of intensive observation and therapy, where the necessary diagnostic tests are performed.
The algorithm for medical care for patients with ACS is presented in Figure 2. The first medications that should be used if ACS is suspected are acetylsalicylic acid - 325 mg orally (to speed up absorption, the tablet should be chewed) and nitroglycerin - 0.5 mg sublingually (if necessary You can take up to 3 tablets with an interval of 5 minutes). Patients with persistent ST segment elevation or the appearance of left bundle branch block receive TLT or undergo primary CBA. Patients with ST segment depression, T wave inversion or no ECG changes receive heparin therapy, beta-blockers, and if pain persists, intravenous nitrates. In cases of intolerance to beta-blockers or the presence of contraindications to their use, calcium antagonists are prescribed. All patients are provided with multichannel ECG monitoring. After receiving additional information (the results of clinical observation, ECG data in dynamics, analysis of the content of cardiac troponins, CPK and MB-CPK in the blood), the diagnosis is clarified and the risk of negative developments is assessed, on the basis of which further tactical decisions are made. Patients who have developed MI, but have not undergone CBA in the acute period, undergo an exercise test before discharge from the hospital to determine the prognosis and indications for surgical treatment.
Rice. 2. Algorithm of medical care for patients with ACS
Patients with a high immediate risk of developing MI and death, if possible, should begin IIb/IIIa receptor blockers, undergo coronary angiography, CBA, and continue therapy with IIb/IIIa receptor blockers. In cases where the administration of drugs of this group and the procedure for myocardial revascularization is impossible, heparin therapy (UFH or low molecular weight heparins) is carried out in combination with acetylsalicylic acid, beta-blockers and, if necessary, nitrates intravenously. After stabilization of the condition of this category of patients, a test with physical activity is indicated to determine the prognosis and indications for CBA or CABG. Treatment of patients at low risk of developing MI and death includes oral acetylsalicylic acid, beta-blockers or calcium antagonists and nitrates. In the absence of ECG changes and an increase in the blood level of biochemical markers of myocardial necrosis according to the results of two determinations, the administration of UFH or low molecular weight heparins can be discontinued. After 5–7 days, patients in this category are advised to perform an exercise test to clarify the diagnosis of coronary artery disease, prognosis and further treatment tactics.
Most adverse events occur in the first months after the development of ACS. In the treatment of patients who have suffered an ACS, in addition to the means of directly influencing the coronary circulation, it is necessary to carry out measures aimed at weakening the effect of modifiable risk factors for the progression of coronary artery disease. Patients should stop smoking. In cases where the use of beta-blockers or calcium antagonists and ACE inhibitors in moderate therapeutic doses does not correct high blood pressure, the doses of the drugs used should be increased or additional antihypertensive drugs should be prescribed. Patients should follow a lipid-lowering diet. Statins, according to modern concepts, are indicated for patients who have undergone ACS, even in the absence of an increase in the level of atherogenic low-density lipoprotein cholesterol in the blood. The idea of using statins from the first day of the disease is receiving more and more compelling evidence.
Mortality rates for ACS in Russia are 2–3 times higher than in Western Europe and North America. The main reason for this difference is the inadequate application of effective methods for diagnosing and treating ACS in domestic clinical practice. Unfortunately, many healthcare institutions in modern Russia do not have the ability to ensure compliance with recommendations for medical care for patients with ACS. However, along with objective difficulties (primarily financial ones), the reasons for this include the lack of professional awareness of doctors. It is the lack of professional knowledge that is the prerequisite for the irrational use of financial resources allocated to provide medical care to patients with ACS, a significant part of which is currently spent on providing uninformative diagnostic techniques and purchasing ineffective drugs. Acceptance by physicians of the main provisions of the recommendations for the diagnosis and treatment of ACS is the most important condition for their successful implementation in clinical practice, and the implementation of agreed standards represents a proven opportunity to significantly improve the results of medical care.
St. Petersburg State Medical Academy named after.
I.I. Mechnikova References:
1. ACC/AHA guidelines for the management of patients with acute myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Pratice Guidelines (Committee on Management of Acute Myocardial Infarction). J Am Coll Cardiol 1996;28:1328–1428.
2. Update: ACC/AHA guidelines for the management of patients with acute myocardial infarction: executive summary and recommendations: a report of the American College of Cardiology/American Heart Association Task Force on Pratice Guidelines (Committee on Management of Acute Myocardial Infarction). Circulation 1999;100:1016–1030.
3. ACC/AHA guidelines for the management of patients with unstable angina and non–ST–segment elevation myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Pratice Guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol 2000;36:970–1062.
4. Management of acute coronary syndromes: acute coronary syndromes without persistent ST segment elevation. Recommendations of the Task Force of the European Society of Cardiology. Eur Heart J 2000;21:1406–1432.
5. Treatment of acute coronary syndrome without persistent ST segment elevations on the ECG. Russian recommendations. Developed by the Committee of Experts of the All-Russian Scientific Society of Cardiologists. M 2001;23.
Prevention
Prevention of coronary insufficiency essentially comes down to preventing the development of atherosclerosis and avoiding chronic stress. The importance of preventive measures increases greatly with age. Here's what you can do to significantly reduce the risk of progression and development of severe consequences of the pathology:
- Regular blood tests for lipid levels and cholesterol levels;
- Reducing the consumption of fatty foods;
- Regular moderate physical activity - at least 150 minutes per week;
- Getting rid of bad habits;
- Timely consultation with a doctor if appropriate cardiac symptoms appear;
- Minimizing stressful situations.
First aid for exacerbation
In the event of an acute attack, you should immediately call an ambulance. The patient's heart can stop at any moment, and it is impossible to resume its work without specialized equipment.
When the main task is completed, attention must be paid to stabilizing the patient’s condition. While waiting for an emergency team, you must:
- Provide peace. The patient should be immediately placed on a bed or sofa. If severe shortness of breath or cough occurs during an attack, the patient should be seated in a chair.
- Eliminate possible chest tightness. During heart attacks, even small loads, including clothing, have an impact on the chest area. The patient needs to completely expose the upper part of the waist, remove not only things, but also jewelry (beads, chains, pendants). If possible, measure your blood pressure
Provide fresh air. In acute coronary insufficiency, a squeezing sensation occurs in the chest area, making breathing difficult. By opening all windows, you can increase the flow and circulation of oxygen in the room. This will ease the patient's breathing and the stress on the heart.- Give medicine. The most common and effective remedy is Validol. It is able to reduce pain until the ambulance arrives. Validol is placed under the patient's tongue, and its effect begins within a few minutes.
Nitroglycerin is the second option for a heart attack. It also needs to be placed under the tongue. It acts faster, already within the first minute. If the pain has not decreased or the changes were insignificant, then after 10 minutes the tablet must be given again. This drug is contraindicated in people with low blood pressure.
There are many causes of coronary insufficiency. It can be triggered by both serious internal damage to the body and external factors. To maintain heart health, you need to take care of yourself, take preventive measures and give up bad habits.
Sources
- Coronary Heart Disease - nhlbi.nih.gov.
- Cardiovascular Therapy and Prevention, 2016; 15(2): 93–99 https://dx.doi.org/10.15829/1728-8800-2016-2-93-99.
- Kurdgelia T. M., Kislitsina O. N., Bazarsadaeva T. S. Sudden cardiac death: epidemiology, risk factors and prevention // BMIK. 2014. No. 3.
- Guide to faculty therapy: textbook / S. A. Boldueva, I. V. Arkharov, E. L. Belyaeva, E. G. Bykova, T. V. Ermolova, M. I. Ivanova, I. A. Leonova, A. P. Makhnov, N. S. Shvets, O. Yu. Chizhova; edited by S. A. Boldueva. — 3rd ed., add. and processed - St. Petersburg: Publishing house of North-Western State Medical University named after. I. I. Mechnikova, 2021. - p. 6-32; 64-76.
- Picard F., Sayah N., Spagnoli V., Adjedj J., Varenne O. Vasospastic angina: A literature review of current evidence. //Arch Cardiovasc Dis - 2021 - Vol.112 - No. 1 - p.44-55
Tests and diagnostics
Electrocardiography plays an important role in the diagnosis of acute and chronic heart failure , which is carried out at rest and under conditions of dosed physical activity. A characteristic sign indicating the presence of a pathology with coronary circulation in a patient is the registration of ST segment depression during maximum physical activity or 2-5 minutes after it. Arrhythmia that occurs during a stress test is also an indirect sign of cardiac circulatory pathology.
The condition of the coronary vessels can be assessed by performing coronary angiography , which allows one to identify areas of stenotic or occlusive vascular damage. The essence of the method is to administer an X-ray contrast agent and subsequently assess the patency of the arteries of the heart.
Laboratory diagnosis is based on determining blood levels of creatinine kinase , glucose, electrolytes, triglycerides, ALT, AST, total cholesterol and lactate dehydrogenase . Crucial importance is given to determining the level of markers of myocardial damage as a result of hypoxia and the concentration of troponins I and T. Detection of high concentrations allows one to suspect myocardial infarction or other damage to the heart muscle.
Differential diagnosis is carried out with the following diseases:
- esophagitis;
- esophageal spasm;
- ulcerative lesions of the digestive tract;
- pulmonary embolism;
- osteochondrosis of the thoracic spine;
- osteoarthritis of the shoulder joint;
- aortic dissection , etc.
List of sources
- Ageev F.T. , Skvortsov A.A. , Mareev V.Yu., Belenkov Yu.N. “Heart failure against the background of coronary heart disease: some issues of epidemiology, pathogenesis and treatment,” Regular issues of “RMZh” No. 15 dated May 26, 2000
- Lupanov V.P. “Algorithm for diagnosis and treatment of patients with chest pain and normal coronary angiogram (cardiac syndrome X)”, article in the journal “Breast Cancer”
- Akchurin R.S., Shiryaev A.A., Galyautdinov D.M. “Indications for coronary bypass surgery in patients with various forms of coronary artery disease,” Regular issues of “Breast Cancer” No. 19 dated 10/03/2002