Microcephaly is a congenital anomaly, which is characterized by a significant reduction in the size of the brain (and, as a result, the skull) as a result of disruption of the growth processes of brain tissue during the period of intrauterine development of the baby.
It can be an independent defect or a manifestation of any other genetic diseases (in this case we are talking about true microcephaly), and it can also develop as a consequence of various diseases the mother suffered during pregnancy (secondary, or false, microcephaly). However, in any case, this pathology is accompanied by a lag in the child’s mental development of varying degrees of severity and the presence of other neurological symptoms.
Statistical information
The incidence of the defect ranges from approximately 1:2000 to 1:10000 among all newborns. As an independent disease, true microcephaly is much less common and is detected in one out of 50 thousand children, both girls and boys. If this pathology occurs as a manifestation of another hereditary disease, then its frequency in the population is determined by the frequency of the underlying disease.
Pathogenesis and causes of the anomaly
According to the form of the disease, microcephaly can be divided into primary and secondary.
The primary cause is most often genetic disorders or an unfavorable course of the first and early second trimester of pregnancy in the mother.
In cases of a secondary form of the disease, the patient's condition is more severe, and cerebral palsy usually occurs. The secondary form of microcephaly is caused by unfavorable factors during the second and third trimester of pregnancy, during childbirth or in the first months of a child’s life.
The main reasons that can result in microcephaly are:
- infectious diseases of the mother during pregnancy;
- disorders in the endocrine system of a pregnant woman;
- abuse of alcohol, cigarettes, drugs by the expectant mother;
- taking certain medications during pregnancy;
- poor ecology and radiation exposure;
- toxic effects of harmful substances on the body of a pregnant woman, poisoning;
- genetic disorders;
- birth injuries in a child.
In addition, rubella, measles, mumps and other infectious diseases suffered by the expectant mother during the period of gestation can also cause abnormal development.
However, there are cases where a completely healthy woman gives birth to a child with a similar anomaly and the cause cannot be established.
Anatomy of the brain
The brain is the main organ of the human nervous system; its formation and development begin in the earliest stages of the embryonic period.
The first rudiments of nervous tissue are formed already on the 18th day of intrauterine development. They are a neural plate, which consists of a small number of neurons (nerve cells). As the embryo forms, their number increases, as a result of which the brain and spinal cord and other elements of the system are formed from the neural plate.
A neuron is a highly specialized cell that consists of a body and many processes through which it communicates with a huge number of other cells. Thanks to this structure, the main function of the nervous system is ensured, namely the reception and processing of information, including the regulation of the vital functions of the entire organism as a whole. Through some neurons (they are called afferent), information in the form of nerve impulses enters the brain, where it is processed and a response nerve impulse is formed, which is sent to organs and tissues through other neurons (they are called efferent).
The formation of nerve cells in the brain is completely completed only at the time of birth, on average reaching about 150 billion neurons. However, throughout a person’s life they are not able to reproduce (divide), and at the same time they gradually die due to so-called apoptosis (a genetically programmed process of death of malfunctioning or damaged cells).
The brain is anatomically divided into three sections.
- Large hemispheres of the brain (right and left). Being the higher parts of the brain, they consist of the cortex and subcortical structures (hypothalamus, thalamus, etc.). The cerebral cortex contains neurons that are responsible for the formation of personality, the processes of self-knowledge and learning (higher nervous activity of a person). Subcortical structures ensure the formation of instinctive and behavioral reactions (sexual, food, etc.). It is also worth noting that the cerebral cortex under normal conditions has an inhibitory effect on subcortical structures; in other words, a person’s consciousness can suppress his instinctive reactions.
- Brain stem. It includes the medulla oblongata, the pons, and the midbrain and diencephalon. They provide reflex activity of the human body, and also maintain communication between the brain and spinal cord. In addition, the trunk contains various nerve centers (for example, vasomotor, respiratory, etc.). They, in turn, ensure the performance of those physiological functions that are not controlled by consciousness (for example, a person breathes automatically, without thinking about it).
- The cerebellum is a small structural formation that is responsible for coordinating human movements, maintaining muscle tone and maintaining balance during complex movements (walking, running, etc.).
The human skull is divided into the brain and facial sections. The latter includes the bones of the face. The development of the skull comes from embryonic tissue called ectoderm. It surrounds the rudiments of the brain from the very beginning of their formation.
There are three stages in the formation of the skull bones:
- membranous - a layer of cells that surrounds the future brain, becomes soft membranous tissue, simultaneously increasing with the growth of brain tissue;
- cartilaginous - from about the sixth to seventh week of embryonic development, this tissue in the area of the base of the skull gradually turns into denser cartilaginous tissue;
- bone - already from the eighth to tenth week of the intrauterine period, ossification points are formed in various parts of the skull, which are zones of the beginning of the growth of bone tissue.
By the time of birth, some areas of membranous tissue (fontanelles) remain in the roof of the skull of a newborn child, which ensure bone mobility during childbirth or when the brain enlarges for any reason.
The large (anterior) fontanelle has a diamond shape and is located at the junction of the frontal and parietal bones. It completely ossifies and closes by the age of two years.
The small (posterior) fontanel has the shape of a triangle and is located in the occipital region at the junction of the parietal and occipital bones. As a rule, it becomes overgrown by the second month of life.
The lateral fontanels are paired and small in size, they are located on the side surface of the head, slightly in front and behind the ears, and are also completely overgrown by the second month of life.
The bones of the facial skull are formed from the so-called gill arches, which are derivatives of mesoderm (another embryonic tissue). Thus, the development of the brain and facial parts of the skull occurs independently of each other. In addition, the formation of the facial skull is practically independent of the development and growth of the brain; however, the size of the cerebral skull normally always corresponds to the volume of the cerebral hemispheres.
At the end of the 19th and beginning of the 20th centuries in Europe and North America, children with microcephaly were sold to the circus. There they took part in the so-called “freak show”.
What does it look like?
One of the main symptoms of microcephaly in children is a reduced head circumference. Over time, the child’s skull stops growing, but its facial part continues to develop according to age. A disproportion between the brain and facial parts of the skull develops and becomes more and more obvious.
Other fairly common signs of microcephaly include the following disorders:
- muscle tone is impaired;
- the child is lagging behind in mental development;
- the large fontanel closes earlier than expected (in some cases this happens already at the time of birth);
- there are serious disturbances in motor and speech development;
- presence of hyperactivity;
- paresis and paralysis are observed;
- coordination of movements is impaired;
- convulsions;
- short stature or dwarfism.
Among children born with such an anomaly, there are also those whose intellectual development corresponds to their age, and whose head circumference increases as they grow. But even in these cases, the head size of such children is smaller than normal.
What microcephaly in children looks like in real life can be seen in the photo and video material:
Reasons for the development of the anomaly
Taking into account the causes and time of occurrence, primary microcephaly (true or hereditary) and secondary (syndromic) are distinguished.
Primary microcephaly in children is a manifestation of hereditary diseases; it accounts for about 7–34% of all types of this anomaly.
Primary microcephaly
The following diseases are independent forms.
Giacomini syndrome is a hereditary microcephaly, which is predominantly manifested by mental disorders in combination with the occurrence of convulsive conditions, as well as the progression of paralysis.
Payne's syndrome - this disease is also hereditary. It affects only boys and is manifested by constant convulsive conditions of the lower extremities, nervous disorders and abnormalities in the functioning of the heart.
Microcephaly can be a manifestation of the following pathologies:
- Down syndrome - the appearance of an extra chromosome in the XXI pair, clinically manifested by impaired mental development of the child, a decrease in the size of the brain and cerebellum, as well as other characteristic symptoms;
- Patau syndrome - the appearance of an extra chromosome in the XIII pair, characterized by low birth weight of the newborn, microcephaly and other anomalies of the skull and internal organs;
- Edwards syndrome - the appearance of an extra chromosome in the XVIII pair, while children have a small or long and narrow skull, low birth weight, underdeveloped brain and cerebellum, as well as developmental defects of the facial skeleton, legs (mainly feet) and internal organs;
- cat cry syndrome is a chromosome defect in the V pair, which is manifested by microcephaly, low body weight, retardation in physical and mental development, as well as a characteristic cry in a child, similar to the meowing of a cat (due to damage to the cartilage of the larynx);
- Prader-Willi syndrome - damage to chromosome XV, characterized by microcephaly, delayed psychomotor development and various anomalies of internal organs and skeletal bones;
- Miller-Dieker syndrome is a defect in the XVII chromosome, leading to disruption of the development of brain neurons in the embryo, as a result of which the brain of a newborn child is reduced and devoid of convolutions, in addition, there is severe muscle weakness, delayed physical and mental development and defects of internal organs;
- phenylketonuria is a hereditary disease characterized by impaired processing and use of one of the amino acids - phenylalanine; the resulting toxic substances have a damaging effect on the central nervous system of the pregnant woman, and also inhibit the development and growth of the fetal brain.
Secondary microcephaly develops due to the influence of unfavorable factors on the fetus in the embryonic period, when the formation and formation of all brain structures occurs. In this case, the genetic apparatus of the parents is not damaged.
Causes of secondary microcephaly
- viruses and infections (rubella, cytomegalovirus, measles, toxoplasmosis);
- alcohol abuse - ethanol almost freely penetrates from the mother’s blood through the placenta into the fetus’s body, the most severe manifestation is the so-called fetal alcohol syndrome, manifested by mental retardation and defects in the development of internal organs;
- drug abuse - they can also easily penetrate the placental barrier and adversely affect the fetus;
- taking certain medications that are contraindicated during pregnancy (for example, anticancer drugs such as colchicine or busulfan);
- intrauterine hypoxia - insufficient oxygen delivery to the tissues and organs of the fetus, which leads to a delay in its growth and development, as well as the occurrence of mental retardation and various anomalies;
- fasting - if the expectant mother fasts for a long time or does not take the required amount of protein food, then the fetal organs cannot form normally, which can be fraught with the development of congenital dystrophies and pathologies;
- mechanical injuries in the early stages of pregnancy can lead to disruption of the development of the brain and internal organs, often even incompatible with life;
- exposure to radiation - in the embryonic period, very intensive growth of all tissues occurs, therefore the damaging effects of radiation on the fetus lead to irreversible changes in the brain.
Folk remedies
Photo: avrorra.com
Traditional medicine is used as an additional measure in the treatment of microcephaly. For example, the well-known dark chocolate is not only a favorite treat for children and adults, but also, due to its richness in flavanols, has a beneficial effect on a person’s mental abilities and mood. The action is realized through the interaction of antioxidant molecules that stimulate brain perfusion.
The effects of ginseng have been known in Chinese medicine for a long time. This amazing plant affects almost all processes of brain activity. It is taken to improve short-term memory, improve attention, improve mood, and also reduce fatigue.
There is another unique plant - Rhodiola rosea. Thanks to research, it has become known that this plant can enhance performance by increasing the threshold of mental fatigue and fatigue caused by stress. In addition, actions such as strengthening associative thinking, improving short-term memory, and increasing the ability to concentrate on various objects and phenomena have been identified.
The diet should contain foods containing sufficient amounts of omega-3 fatty acids (walnuts, flax seeds, herbivore meat, legumes). In addition, you can buy fish oil capsules at the pharmacy that are rich in omega-3 fatty acids. This substance is considered absolutely deservedly useful, since increased mental activity is observed not only in people with reduced intellectual ability, but also numerous studies have led to the conclusion that healthy people also experience increased mental activity. You should also give preference to complex carbohydrates when choosing between simple and complex ones. The main source of complex carbohydrates is cereals. Moreover, it is worth noting that we are talking about whole grain products, and not about their processed products. That is, it is recommended to use oats, buckwheat, wheat, and brown rice. But oatmeal, buckwheat flakes, and semolina porridge can be excluded from the diet. Also, special attention is paid to the amount of vegetables eaten per day. Almost all vegetables are a source of complex carbohydrates. It should be remembered that to preserve the beneficial properties of vegetables, it is recommended to consume them raw.
The information is for reference only and is not a guide to action. Do not self-medicate. At the first symptoms of the disease, consult a doctor.
SEARCH FOR TREATMENT AROUND THE WORLD WITH YELLMED
Symptoms of microcephaly
In most cases, it appears immediately after the baby is born. If concomitant pathologies are compatible with life, then as the child grows older, the skull may undergo some changes and even increase slightly in size, but will always lag behind the age norm.
The usual appearance of such a newborn is characterized by the following features:
- noticeable predominance of the facial part of the skull over the brain;
- reduction in the vertical dimensions of the skull;
- prominent brow ridges;
- the presence of skin folds in the occipital region;
- the forehead is narrow and, in the case of a pronounced form, can be inclined at the back;
- wide and short nose;
- large, low-set ears.
The large fontanel and cranial sutures with this anomaly heal already in the first months of the baby’s life. In the future, children with microcephaly, as a rule, are lagging behind in weight and height, have a disproportionate physique, large sparse teeth and a narrow, high (Gothic) palate.
Neurological disorders can be represented by severe muscle weakness and loss of coordination, spastic paresis, convulsions and strabismus. Often such children may suffer from cerebral palsy (CP) and epilepsy. They begin to hold their heads up, crawl, sit and walk late. In addition, there is a noticeable delay in speech development, limited vocabulary, unclear articulation and impaired understanding of speech addressed to them.
With mild mental retardation, such patients can be quite trainable, capable of self-care, as well as performing simple tasks. But, in most cases, a microcephalic child requires care and supervision from adults.
Depending on their temperamental characteristics, these children can be classified into the so-called torpid or eretic group. Patients in the first case are characterized by lethargy, inactivity, and indifference to the environment; in the second case - hyperactivity, fussiness and unstable attention. The emotional sphere in patients with microcephaly is relatively preserved: children are good-natured and friendly, much less often they are emotionally unstable and have a tendency to affective outbursts.
Depending on the postnatal course of microcephaly, 4 types of its clinical manifestation are distinguished.
- Type I is characterized by the absence of an increase in symptoms of the disease. At the same time, the child retains completely normal motor activity, convulsions and spasms are not observed, and the IQ level is within 60;
- Type II is characterized by frequent manifestations and rapid progression of convulsive syndrome. The death of patients with this form of pathology, as a rule, occurs mainly from respiratory infections at the age of 10–12 years;
- Type III manifests itself with rapid progression; convulsive syndrome develops quite early, while its spastic component is sharply expressed. There is also a delay in psychomotor development;
- Type IV is an autosomal recessive pathology (unclassified microcephaly). It is characterized by the complete absence of convulsive and spastic syndrome.
WHO activities
Since mid-2015, WHO has been working closely with the Americas to investigate and respond to the outbreak.
The Strategic Response Program and Collaborative Action Plan outlines the steps WHO and partners are taking to address the Zika virus and its potential complications:
- Working closely with affected countries to investigate the Zika virus outbreak and respond to an unusual increase in microcephaly cases.
- Engage with local communities to communicate the risks associated with Zika virus disease and how they can protect themselves.
- Provide guidance and mitigate the potential impact on women of childbearing age and pregnant women, and on families affected by the Zika virus.
- Provide assistance to affected countries to improve health care for pregnant women and families with children born with microcephaly.
- Investigation into the reported increase in microcephaly cases and possible links to Zika virus infection, with the participation of experts and partners.
Consequences and quality of life
The quality of life of children with microcephaly is primarily determined by the severity of mental development disorders, which determines their future ability to self-care and learning.
Debility is a mild degree of mental retardation. In this case, children can be taught basic self-care skills, simple work, as well as speech, reading and writing. Such patients get along well in society, however, they cannot master the regular school curriculum, so they must go to special schools designed for children with mental disabilities. In this case, the prognosis for life is relatively favorable - these people can live up to 30 years, and in the most rare cases even into old age.
Imbecility is severe mental retardation. In such children, the ability to self-care is sometimes preserved, but often they still require constant care. Their intellectual abilities are extremely underdeveloped, and they are quite difficult to train. In this case, the prognosis for life is also less favorable - in quite rare cases, such patients even survive to adulthood. The cause of death, as a rule, is infectious diseases of the upper respiratory tract (pneumonia) or malformations of other internal organs, which are very often detected in children with microcephaly.
Idiocy - severe mental retardation. Such children are not able to care for themselves and cannot be taught. Their survival directly depends on the care of those around them. In this case, the prognosis is unfavorable - death occurs already in the first years of the child’s life due to disruption of the functioning of internal organs, concomitant developmental defects or infectious complications.
Description
Microcephaly is a developmental defect of the central nervous system, characterized by a decrease in brain mass and skull circumference.
Microcephaly is a cause of mental retardation and neurological abnormalities. It occurs with equal frequency among both boys and girls. It is believed that for every 10,000 newborns, there is 1 child with microcephaly. With microcephaly, a decrease in brain mass is detected (normally approximately 400 g), the circumference of the newborn’s head is reduced to 25–27 cm (normally 35–37 cm).
It is quite difficult to establish the exact cause of the formation of pathology. Possible factors are:
- alcohol, drug or nicotine addiction of the mother, leading to intoxication of the fetus;
- infectious diseases of the mother during pregnancy (for example, toxoplasmosis);
- serious toxic poisoning of the mother during pregnancy;
- exposure to radiation;
- taking toxic doses of certain medications (for example, some antibiotics that have a teratogenic effect);
- various genetic defects.
Unfortunately, there are no effective treatments for microcephaly. The main treatment is aimed at reducing the severity of symptoms of the pathology. For this purpose, nootropic, sedatives, anticonvulsants and decongestants, therapeutic exercises, and manual therapy are used. Methods of upbringing, training and development of the child’s personality develop elementary self-care abilities and motor skills. Often children with a similar diagnosis attend a special boarding school. The outcome of the disease is unfavorable, the pathology cannot be completely cured. The average life expectancy of a child is 15 years; in rare cases, patients live up to 30 years.
Diagnostics
Prenatal diagnosis of microcephaly includes ultrasound examination (ultrasound). During this procedure, the doctor compares the data obtained on the size of the fetus's head and torso with normal values. The most reliable information can only be obtained if you know exactly the duration of pregnancy.
Determining mutations of genes and chromosomes is the so-called invasive diagnostics. This method is carried out with a puncture of the fetal bladder, because the material for research is fetal villi, amniotic fluid, and also particles of epithelium.
Prenatal screening also includes a biochemical blood test. In addition, the pregnant woman is asked to fill out a special form, which, among other questions, contains a column about the timing of pregnancy. All information received and test results are processed in a special computer program that shows the likelihood of developing brain microcephaly.
A newborn baby is examined by a neonatologist in the delivery room in the very first minutes of his life through an external examination. If the diagnosis is confirmed, then an additional comprehensive examination is required.
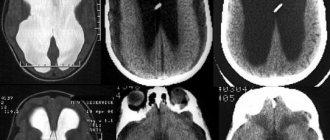
Children with microcephaly must be consulted by a geneticist to identify concomitant hereditary diseases. In order to determine the degree and prognosis, it is also important to conduct a full instrumental examination: ultrasound of the brain (neurosonography), electroencephalography (EEG), radiography of the skull, as well as computed and magnetic resonance imaging (CT and MRI).
In addition, in order to identify defects in the development of other organs and systems, the child should receive consultations from specialized specialists: otolaryngologist (ENT), ophthalmologist, cardiologist, neurologist, neurosurgeon, orthopedist.
Diagnostic features
Diagnosing microcephaly is not particularly difficult; it is based on determining morphological parameters and identifying signs of intellectual underdevelopment in a child.
Diagnosis is also carried out during pregnancy, this makes it possible to identify concomitant pathologies in fetal development and the risk of an anomaly such as microcephaly.
This is detected by obstetric ultrasound, when the biometric parameters of the fetus corresponding to a certain stage of pregnancy are compared. However, signs of an abnormality in the fetus can be detected only at 27-30 weeks of pregnancy.
In this regard, if there is a suspicion of the development of such a pathology due to genetic or chromosomal disorders, it is necessary to conduct additional examinations.
The degree of development of pathology can be determined using methods such as neurosonography, MRI of the brain area, EEG, and radiography.
Treatment
Medical care for microcephaly comes down mainly to symptomatic support for patients, since it is impossible to restore normal brain activity, but there are ways to correct it. Treatment implies an integrated approach aimed at the physical and intellectual development of the child with the goal of maximizing his adaptation in society. It is carried out in three directions.
- Drug therapy. It is used to stimulate metabolic processes in the brain. For this, nootropic, sedative, anticonvulsant and dehydration drugs, as well as B vitamins, are prescribed.
- Physiotherapeutic procedures, physical therapy and massage.
- Therapeutic measures aimed at correcting the mental development of the child. In the event that mental retardation does not reach a severe degree (idiocy), then it is quite possible for such a patient to be taught basic self-care skills, performing simple work, and sometimes even speech and writing. For this purpose, long-term classes with specialists, special training programs and other necessary activities are held.
There is a so-called conductive pedagogy. Its essence is to create conditions that encourage the child to mental, motor and emotional activity, which creates the prerequisites for the further development of his intellect and psyche. During this treatment, the patient learns both simple and complex movements, learns to think and make decisions. At the beginning, the child develops motor behavioral stereotypes, which, as a result of long and hard work with teachers, gradually become meaningful and automated, that is, he does not just learn and repeat certain movements, but realizes the purpose for which he does this.
For each patient, an individual training program is drawn up, which in turn includes therapeutic exercises and physical education, exercises with various sports equipment, classes with a speech therapist, audiologist, psychotherapist and other specialists. This technique allows one to achieve fairly good results in children with various forms of mental retardation, including microcephaly.
Treatment of children with the primary form of pathology is sometimes successful. However, it should be remembered that even with timely and well-chosen therapy, the baby will never be completely healthy, but he will be able to lead a more simplified social life.
Medicines
Photo: pp.userapi.com
The main medications prescribed for microcephaly are aimed at improving metabolic processes in the brain. Due to this, a weakening of symptoms is achieved, which leads to a temporary improvement in the child’s condition.
Piracetam is a nootropic drug that has a beneficial effect on blood circulation and metabolic processes in the brain. According to researchers, the drug can have the following effects:
- stimulates intellectual activity;
- improves memory;
- facilitates the learning process;
- increases mental performance.
The drug is well tolerated and has virtually no contraindications for use. Side effects that occur while taking the drug include: dyspeptic symptoms, general weakness, dizziness, anxiety, sleep disturbance.
Gromecin (glycine) is also a nootropic drug. Capable of increasing mental performance, memory, concentration, normalizes mood, and regulates minor sleep disturbances. Side effects while taking the drug are rare. More often they are associated with individual intolerance and manifest themselves in the form of skin rashes and itching.
Cerebrolysin helps increase the rate of glucose penetration when the blood-brain barrier is disrupted, influencing the level of its consumption in damaged parts of the brain. In addition, this drug has a positive effect in cases of disruption of oxidative processes in the structure of brain metabolism and reduces the level of cerebral concentration of lactic acid. This leads to improved brain function.
B vitamins (neurobex, borivit) are also prescribed to improve the conduction of nerve impulses.
With microcephaly, epilepsy often develops, so an indispensable component of therapy is the prescription of anticonvulsants. The selection of a specific drug from this group, dosage and frequency of administration is made individually for each patient. This takes into account the type of seizures, the frequency of their occurrence and sensitivity to drug treatment. The most appropriate drug, prescribed by a qualified neurologist, is taken by the patient continuously. This is necessary to prevent the development of a seizure, during which the child may be injured. If an epileptic attack does occur, diazepam is immediately administered. This drug has many therapeutic effects, including being used to relieve seizures. It is important to understand that this drug is under no circumstances used as maintenance therapy, as there is a risk of developing addiction, as well as other undesirable effects.
Mental retardation, or oligophrenia
21171 November 18
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Mental retardation (oligophrenia): causes, symptoms, diagnosis and treatment methods.
Definition
Mental retardation is a group of conditions caused by congenital or early acquired mental underdevelopment with severe intellectual deficiency. Patients experience impairment of cognitive, speech, motor and social abilities. The term “oligophrenia” is used less and less these days.
Mental retardation in the world occurs from 3.04 to 24.6 and higher per thousand of the population.
Causes of mental retardation
Mental retardation is the result of severe organic damage to the brain during the period of intrauterine development of a child and/or in the first months of his life. Particularly dangerous is the impact of pathological factors on the fetus in the first trimester of pregnancy, when the formation and intensive formation of brain systems occurs.
Identifying the causes of mental retardation presents certain difficulties, since this mental illness is the result of the combined influence of external and hereditary factors at different stages of the formation of the nervous system. These factors include:
- genetic disorders that occur during the fertilization stage and lead to underdevelopment of the brain;
- hereditary defects combining dementia with damage to the muscular, bone, skin, cardiovascular systems, vision and hearing;
- microcephaly – congenital or acquired reduction of the brain with limited possibility of its growth;
- hydrocephalus – an increase in the amount of fluid in the cavities of the brain with changes in the neurodynamics of brain processes;
- immunological incompatibility of the blood of mother and fetus;
- inflammatory processes in the brain (meningitis, meningoencephalitis, severe somatic infections);
- brain injuries (birth trauma, application of obstetric forceps or the use of other mechanical methods of childbirth, compression of the baby’s head when passing through the birth canal, prolonged asphyxia during childbirth);
- toxic effects on the fetus of alcohol, psychoactive substances, certain medications used by the mother, intoxication, radioactive and x-ray irradiation of the reproductive cells of the parents and the fetus itself;
- severe somatic diseases (with intoxication, dystrophy);
- inborn errors of metabolism (amino acids, metals, salts, fats and carbohydrates), which lead to changes in the functioning of the brain.
The following main variants of hereditary metabolic defects accompanied by mental retardation are distinguished:
- amino acid metabolism disorders: phenylketonuria, homocystinuria, histidinemia, etc.;
- metabolic disorders of organic acids and carbohydrates: galactosemia, fructosuria, etc.;
- storage diseases: mucopolysaccharidoses (Hurler, Gunter syndromes, etc.); lipidoses (Tay-Sachs disease, Gaucher disease, Niemann-Pick disease, etc.); glycogenosis (Pompe disease, etc.);
- leukodystrophy;
- metabolic and hormonal disorders: non-endemic forms of hypothyroidism, Albright's pseudohypoparathyroidism, etc.;
- other metabolic disorders of mineral, bilirubin and other types of metabolism.
Mental retardation can occur in combination with any other mental disorder.
Classification of the disease
There are clinically differentiated and clinically undifferentiated forms of mental retardation.
The group of differentiated mental retardation includes diseases with a specific clinical picture, for which mental underdevelopment is one of the main manifestations. Most often these are genetically determined disorders.
Clinically undifferentiated forms of mental retardation include disorders the cause of which cannot be accurately determined and there is no specific clinical picture of the disease.
Classification of differentiated forms of mental retardation
Hereditary forms:
- Syndromes with multiple congenital anomalies:
- chromosomal diseases;
- genetic syndromes with an unclear mode of inheritance;
- monogenically inherited syndromes.
- Hereditary metabolic defects.
- Phakamatoses (systemic congenital diseases affecting the skin, nervous system and eyes).
- Neurological and neuromuscular diseases, which are characterized by the presence of mental retardation.
Mental retardation of mixed (hereditary-exogenous) nature:
- Microcephaly.
- Hydrocephalus.
- Craniostenosis.
- Congenital hypothyroidism.
Exogenously caused forms of mental retardation:
- Alcoholic fetopathy.
- Infectious embryofetopathies.
Symptoms of mental retardation
Despite the variety of causes of mental retardation, common developmental mechanisms lead to a similar clinical picture. Mental retardation is characterized by mental underdevelopment with insufficient intelligence, impaired abilities and skills, which complicates the patient’s adequate social adaptation.
Clinical signs of mental retardation:
- mental underdevelopment of varying degrees of severity;
- underdevelopment of not only the patient’s intellectual activity and personality, but also the psyche as a whole;
- signs of underdevelopment not only of thinking, but also of perception, memory, attention, emotional-volitional sphere, etc.;
- insufficient ability for generalization and abstraction.
Depending on the level of intellectual development, there are four degrees of severity of mental retardation.
Lightweight
(IQ from 50 to 69 units): most patients, when studying in specialized schools according to specially designed programs, master the skills of reading, writing, counting, and acquire labor skills that do not require high qualifications.
Moderate
(IQ from 35 to 49 units): from early childhood, children are delayed in development, do not fully master self-care skills, and need outside control and care throughout their lives.
Heavy
(IQ from 20 to 34 units): the level of speech development allows only to communicate their needs, they are not capable of detailed speech statements. They have only basic self-care skills, are helpless in everyday life, and need outside control and care.
Deep
(IQ less than 20 units): no speech skills or speech consists of separate words, often do not understand speech addressed to them, do not have simple self-care skills, are unkempt, need constant care and supervision, left to their own devices remain motionless or are in a monotonous, meaningless excitement.
Intellectual underdevelopment is combined with disturbances in the processes of excitation and inhibition. At different periods of life, excitation processes can prevail over inhibition processes and vice versa. Patients with a predominance of excitation processes are characterized by motor disinhibition and increased impulsivity. Persons with a predominance of inhibition processes are sluggish and inert.
Intellectual abilities and social adaptation may improve slightly over time as a result of training and rehabilitation.
Mental retardation may be:
- with no or mild behavioral disorders;
- with significant behavioral disorders requiring care and treatment.
Behavioral disorders can be relatively compensated (non-exacerbation phase) or decompensated (exacerbation phase).
The transition to the exacerbation phase is caused by a stressful situation, somatic illness, traumatic brain injury, endocrine changes in the body, and a combination of several factors.
Diagnosis of mental retardation
The diagnosis of “mental retardation” is purely clinical and is established on the basis of complaints, anamnestic data, clinical and psychopathological examination (external examination, genetic research, pathopsychological and instrumental methods).
There are three diagnostic criteria for mental retardation:
- clinical criterion (presence of organic brain damage);
- psychological criterion (persistent impairment of cognitive activity);
- pedagogical criterion (low ability to learn and absorb knowledge).
To make a diagnosis, objective facts of life are clarified:
- data on hereditary burden of mental illness;
- information about the blood relationship of the parents;
- data on the mother’s obstetric and gynecological history, her state of health before and during pregnancy, information on pathogenic biological effects during the period of intrauterine and perinatal development of the patient, and previous diseases.
From the place of study or work (if the patient studies or works) the following is specified:
- data on the patient’s early psychomotor development, characteristics of speech formation, school skills, the patient’s personality, family and social status, exogenous exposures suffered, characteristics of psycho-emotional response, mental trauma;
- data on the characteristics of the patient’s mental state and behavior in adulthood, self-care skills, the ability to establish and maintain contact with people around him, build his behavior taking into account existing moral, ethical and cultural traditions, cope with his social responsibilities, etc.
During a conversation with the patient, the following is revealed:
- degree of orientation in the environment, in time;
- the ability to maintain a dialogue with a doctor, provide coherent and consistent information, and understand complex logical and grammatical structures;
- the formation of mental operations (analysis, synthesis, establishment of cause-and-effect relationships);
- the level of knowledge about the surrounding world, the degree of orientation in matters of community life, the society surrounding the patient;
- features of the motivational-need sphere;
- features of memory, attention, performance;
- features of emotional manifestations;
- concomitant mental and psychoneurological disorders present at the time of examination.
The doctor performs a general examination of the body, which includes identifying signs of intrauterine development disorders, identifying traces of various injuries, examining the condition of organs and systems of the body and the presence of somatic diseases during life.
Neurological examination reveals dysfunctions of the cranial nerves, reflexes, extrapyramidal disorders, disorders of motor coordination, sensitivity, and functions of the autonomic nervous system.
Using special tests, tables and scales (Wechsler test, Schult tables, Kraepelin counting, Bourdon proof test, Toulouse-Pieronai test, Dembo-Rubenstein scales, projective tests, Rosenzweig, Wagner tests, drawing techniques, etc.) the study is carried out attention, memory, mental performance, individual psychological characteristics, determining the level of learning ability and assessing the level of intelligence development.
Instrumental research methods are aimed at searching for possible organic lesions of the central nervous system:
- rheoencephalographic study;
- echoencephalographic study;
- MRI of the brain;