- Author:
Dentist-orthodontist Yulia Yakovlevna Naumovich - Category:
Doctor of the highest qualification category - Experience: More than 12 years
Cleft palate is a pathology of the hard and soft palate. Occurs in approximately 1 in 1000 newborns (2 times more often in girls) and is often combined with other abnormalities of the jaw formation
SYMPTOMS OF CLEFT PALATE
Symptoms of cleft palate are noticeable immediately upon birth. Breathing in such newborns is difficult, the air does not have time to warm up, so there is a predisposition to respiratory tract diseases. Due to the inability to suck, the baby has to be fed using additional devices. Pathological changes in the maxillofacial apparatus do not allow speech development. As a result of fluid accumulation, otitis media occurs, which can lead to hearing loss. With the appearance of teeth, their curvature, malocclusion, and extra teeth overlapping each other are noted. There is no physical or mental retardation in development, but children experience psychological discomfort and withdraw into themselves.
We know how to cure Cleft Palate
In the near future, a medical coordinator will contact you and advise you on the conditions and cost of treatment, select a doctor and make an appointment for you.
| Make an appointment | Or call us +375 29 699-03-03 +375 33 319-03-03 |
Cleft lip - symptoms and treatment
A multidisciplinary team is involved in the treatment of patients with clefts, since even a well-performed operation does not guarantee the absence of other complaints. Team members: pediatrician, dentist, orthodontist, plastic or maxillofacial surgeon, nutritionist, speech therapist, ENT, ophthalmologist and neuropsychiatrist. The ENT doctor works to prevent concomitant pathology of the middle ear, which often develops with clefts, and, if present, treats it. Orthodontists make orthodontic structures (obturators), thanks to which the child can eat normally. Obturators are prosthetic devices that close a cleft and can be used for children of all age groups.
Dentists Hubener D.V. and Liu J.R. classified means for orthopedic treatment of the cleft into preoperative and postoperative, active and passive, extraoral and intraoral [14]. There was a long debate about how these methods affect the growth of facial bones and whether they worsen the prognosis, until naso-alveolar plates were invented, which were made first of acrylic, then of rubber. The plates closed the cleft, and the child could suck normally; in addition, the pressure of the plate helped support the wings of the deformed nose, improved the ratio of the lengths of the columella, the cleft parts of the lip, and gently moved the triangular bone [11].
Many types of surgical treatment have been described for the treatment of cleft lip and palate, although the possibility of performing such operations has arisen relatively recently.
Since early times, people have tried to find a way to get rid of this defect. They tried to connect the crevice with sharp sticks, then they used metal needles that were wrapped with thread. Due to the lack of means for pain relief, the operations were primitive and ineffective. Since the 16th century, they have tried to use special caps for external impact on the cleft, trying to cause the edges to stick together. The protruded premaxillary bone in the case of bilateral clefts was simply cut off, which most often led to worsening deformation of the midface.
Surgery to correct a cleft lip is called cheiloplasty . With the beginning of surgical corrections, cheiloplasty methods began to change and improve. The first operations were perceived as a miracle; they created a linear incision. Over time, they began to make incisions of increasingly complex configurations in order to correct associated deformities and prevent the appearance of new ones. Now, in order to correct the complex deformity that occurs in the midface area and create conditions for the normal development of the facial part of the skull, it is necessary that the operation fulfill the following conditions:
- Was safe for young children.
- I corrected the maximum in each specific case in 1 stage.
- Formed the correct line of the red border and Cupid's bow.
- Correct formation of the filtrum is desirable.
- Provided sufficient depth of the vestibule of the oral cavity.
- It eliminated improper attachment of the fibers of the orbicularis oris muscle and created a continuous layer of muscle, which will help in the correct formation of the bones of the facial skull.
- Lengthened the short medial part of the cleft lip.
- Corrected the shape and position of the nasal cartilage.
In 1938 A.A. Limberg described and in 1952 expanded the method of unilateral cheiloplasty. This method became the leading method in the USSR for a long time, because in most cases it made it possible to correct the concomitant deformation of the nasal wing on the cleft side.
In 1952, Tennyson C.W. in the USA and in 1955 Obukhova L.M. in the USSR they described a cheiloplasty method of a more complex configuration. The method is still used today; in addition, cheilorhinoplasties have been developed on its basis to reduce the likelihood of developing associated deformities. The techniques are interesting primarily for their historical significance: for the first time, complex-shaped incisions began to be made and the lip was lengthened. However, lengthening the lip on the cleft side was also a limiting factor because it itself created a recognizable deformity. Techniques are now being used to solve this problem.
The most used technique for suturing unilateral clefts in the world now is the Millard technique and its modifications. In our country this is a modification of I.A. Kozina.
Millard cheiloplasty involves simultaneous restoration of the continuity of the upper lip and correction of the nasal cartilage. On the medial fragment of the upper lip, point 1 is marked - the center of the cupid's bow. On the healthy half of Cupid's bow, look for limiting point 2 (apex of the arc), located approximately 2-4 mm from the midline. This distance is laid on a white roller on the shortened side, obtaining point 3. The length of the lateral fragment of the lip on the healthy side is measured between the limiting point 2 and the commissure of the mouth (point 6). The resulting distance (approximately 20 mm) is laid on a white roller on the damaged side of the commissure (point 7) and a limiting point 8 is obtained. Point 8 will be the top of the cupid's bow on this side; it should connect to point 3 on the medial segment. Measure the distance from point 2 to the base of the nasal wing of the healthy side (point 4), the same distance is set aside from point 8 to the base of the nasal wing of the affected side (point 10). On the shortened side, from the middle of the base of the columella (point 5) to point 3, an arcuate rotational incision is made, symmetrical to the arc of the philtrum on the healthy side. If necessary, extend the incision to point x (reverse incision towards the healthy philtrum). On the lateral (side) fragment, according to the length of the section x-5-3, point 9 is found medially from the base of the flattened wing of the nose. Modifications are mainly used to expand the intervention to the nose, with secondary cheiloplasty, hidden and incomplete clefts.
The advantages of this method of primary cheiloplasty:
- maximum tissue preservation;
- moving all elements of the upper lip to the correct position;
- formation of the bottom of the vestibule of the nasal cavity and the deep vestibule of the mouth.
The method simultaneously corrects the position of the deformed wing of the nose, and some modifications are supplemented with one-stage rhinoplasty. In addition, the arcuate scar is hardly noticeable and can be used for corrective cheiloplasty in adulthood.
Closure of a bilateral cleft can be one-stage or two-stage. This depends on the volume of the cleft, the experience and confidence of the surgeon in his techniques. Each option has its pros and cons, but it is believed that with the help of one-step closure of the cleft, it is more likely to fully create a sphincter of the orbicularis oris muscle.
Sometimes it is practiced to connect the edges of the cleft. This is not a full-fledged cheiloplasty, but only the transfer of a complete cleft into an incomplete one in the expectation that the pressure of the connected part of the lip will have an orthopedic effect on the edges of the cleft, which will lead to their convergence. In most Western countries, the Millard method of cheiloplasty remains the leading one [12].
With a two-stage closure, one side of the cleft is first closed using any method, and after some time the other side is closed.
The debate about at what age to perform surgery still continues to this day. There are those who urge treatment to be carried out as early as possible. Even operations on the fetus are offered, due to the lack of scarring in the prenatal period. Many insist on surgery in the first days and even hours of life. On the one hand, there are advantages to this (parents are not afraid of the child’s appearance, there are no intra-family conflicts, there are no problems with nutrition), but there are also disadvantages (imperfect thermoregulation of newborns, high sensitivity to blood loss, very small anatomical basis). In the 60s of the last century, a large-scale analysis of the results of operations performed in the maternity hospital in the first days of life was carried out. The result showed in almost all children much worse results than in patients who were operated on as adults [1]. N.M. Mikhelson, in one of the oldest Russian manuals on plastic surgery, advises performing the operation at the age of 5-6 months, when the child is sufficiently strong and developed. He believed that cosmetic success was easier to achieve during this period. It is also described that such operations should be performed under local anesthesia, due to the danger of anesthesia [10]. Now there are safe drugs for anesthesia, so it is difficult to imagine performing an operation on young children under local anesthesia. Most surgeons believe that primary cheiloplasty is indicated at the age of 6-12 months.
The extent of the operation depends on the degree of the cleft. Many modern authors believe that in case of a complete cleft, primary cheiloplasty (when only the cleft is sutured) should be used in exceptional cases, since it does not correct the condition of the nose. Therefore, now the primary rhinocheiloplasty technique should be used, when, together with suturing the cleft, the position of the alar cartilages, septum, and vomer is corrected. The quality of the primary operation should be maximum, since repeated corrections are more difficult to perform in conditions of soft tissue deficiency and extensive scarring [4].
Complications during surgery
When performing surgery, the danger is aspiration (inhalation by the patient) of blood and mucus, which can cause asphyxia. To prevent this, you should prevent bleeding and carefully suck out the contents of the oral cavity (blood, saliva, mucus). Possible complications also include collapse, shock, laryngospasm and other conditions.
Mortality on the operating table and shortly after surgery is usually associated with improper selection of patients. You cannot operate on malnourished and premature children, those who, even before surgery, suffer from inflammatory conditions of the respiratory system, hearing, and decompensated abnormalities in the development of the brain, heart, and blood vessels. Also, surgery is prohibited in the presence of thymic-lymphatic status (enlarged thymus). The possibility of surgery should be decided together with the pediatrician.
Complications after surgery
In the coming days after surgery, stenosis (narrowing) of the larynx, bronchitis, pneumonia, urinary retention and other somatic complications may occur, the prevention and treatment of which should be carried out with the participation of a pediatrician. The most common local early complication is suture dehiscence, which is usually associated with technical errors in the operation:
- excision of a significant amount of tissue in the area of the edges of the cleft;
- insufficient tissue preparation;
- incorrect layer-by-layer suturing of the wound;
- tissue tension in the wound area, inflammation and swelling in the operation area.
Sometimes the sutures come apart due to injury (a child’s fall, an accidental blow to a hard object), infection, or the child’s illness with ARVI, rhinitis and other inflammatory pathologies. If the sutures diverge, the issue of applying secondary sutures is decided according to the patient’s condition.
When examining a patient who has undergone surgery, the height of the upper lip, the degree of its deformation, the depth of the vestibule of the mouth and its tightness (the presence of oronasal anastomoses and palate defects) are checked. You should pay attention to lip mobility, phonation, and changes in the structure of the dental system. The integrity of the orbicularis oris muscle can be tested by having the patient stretch his lips into a smile and purse his lips into a tube [1].
Severe psychological trauma is caused by scar changes after an unsuccessful first operation. One of the most unpleasant long-term complications of cheilorhinoplasty is deformation of the upper lip, nose and upper jaw, which can occur for various reasons [9].
After surgery, the patient may have a lack of soft tissue of the upper lip, its lengthening or shortening, stiffness due to extensive scarring, or an aesthetic defect. Alveolar cleft leads to the formation of crowding of teeth, the growth of dystopic (improperly positioned) and supernumerary (extra) teeth, which can support inflammation or, due to their location, form an oronasal fistula (an opening between the oral cavity and the nasal cavity). In general, such a fistula can also be due to excessive tension, cutting sutures, a defect in suturing, etc. Through it, the discharge of liquid part of food into the nasal cavity can persist, which in turn helps to maintain chronic rhinitis, sinusitis, etc.
Possible insufficiency of the muscle ring of the orbicularis oris muscle, which develops with defects in muscle alignment or insufficient separation of muscle fibers from the pyriform opening. Deformation of the vestibule of the mouth in the form of its flattening complicates further orthodontic treatment, which is so necessary for patients, and aggravates the retrusion of the midface (backward displacement). Deformations of the external nose and septum lead to a significant deterioration in the aesthetic result and disruption of nasal breathing, and breathing through the mouth in such patients aggravates the deformation of the facial skeleton.
TREATMENT
Treatment for cleft palate is only surgical. In early childhood, veloplasty (stitching of the soft palate) is indicated due to the small size of the oral cavity. Further, with the growth and development of the jaws, Limberg uranoplasty is performed. The postoperative regimen recommends careful oral care, eating exclusively pureed food, alkaline drinking, bed rest, and breathing exercises. After two weeks, a set of exercises and massage of the soft palate begin. To exclude postoperative infection, antibiotics are prescribed, and in case of severe pain, analgesics are prescribed.
Features of caring for a baby with facial clefts
Carefully clean the nose using damp cotton swabs soaked in oil (sterile olive, sea buckthorn) or herbal infusions (chamomile).
With cleft lips and palate, part of the oral mucosa is in constant contact with air. This leads to the formation of cracks and crusts on the mucous membrane of the upper lip. Toilet your upper lip, especially in the cleft area: carefully remove pre-soaked crusts and treat the surface with sterile oil.
When walking in the cold season, use gauze masks on the area of the wide cleft of the upper lip to warm the incoming air.
Stages of uranoplasty
Before surgery, your baby needs to learn how to feed from a spoon. Sucking after surgery for a cleft soft and hard palate in a child causes pain, impairs wound healing and scar formation. The correction is performed under general anesthesia due to the proximity of the airways and the need for complete immobility of the patient. If it is impossible to close the gap with local tissues, plastic surgery is performed with flaps taken from the cheeks or tongue. Repeated surgical interventions are possible no earlier than six months later, necessary to restore tissue and blood supply.
The operation for cleft of the hard and soft palate is carried out in several stages:
- The peeling away of plastic material on both sides of a gap to close the hole.
- Lengthening of soft tissues by cutting off the mucous membrane of the nasal cavity.
- Stitching the gap at the midline.
- Reducing the pharynx in the middle section by moving its lateral tissues to the middle.
- Step-by-step suturing (first on the nasal mucosa, then on the muscle tissue and oral mucosa) with treatment with an antiseptic solution.
- Attaching a plate that protects against infection.
Types and manifestations of anomalies
The defect in newborns is manifested by a complete cleft of the soft and hard palate, passing through, or a small crack only in the soft tissues. According to the degree of bifurcation, the defect is classified into:
- complete – with splitting of soft and hard tissues up to the incisive foramen;
- incomplete - with a cleft only in the soft palate or with partial cleft of the hard palate;
- through – one- or two-sided clefts of the hard and soft palate with the inclusion of the alveolar process;
- hidden - the gap cuts only the muscles while preserving the oral mucosa.
“Cleft palate” in newborns, in addition to a cosmetic defect, is accompanied by a number of symptoms indicating disorders of the vital functions of the body. From the moment the baby is born, disturbances in sucking and swallowing of food appear. Shallow breathing develops, leading to oxygen deficiency and a tendency to inflammation of the middle ear, which negatively affects hearing. With the active growth of the baby, disorders of the speech apparatus (pronunciation of sounds through the nose) and delayed development of all body structures are detected.
Diagnosis of the defect
The intrauterine development of the fetal facial bones suggests their fusion at the 7-8th week of pregnancy. The formation of the oral and nasal cavities occurs in parallel. Disruption of these processes can become a turning point in normal development, causing abnormalities, and the cause of cleft palate in children. By 2 months, the embryo’s upper jaw is finally formed from halves growing towards each other. A delay in their fusion leads to a defect that is diagnosed in the womb.
A routine ultrasound examination reveals the defect at 14-16 weeks of pregnancy. The volume, shape of the lesion and the complexity of the disease can only be assessed after the baby is born. The diagnosis of “cleft palate” in a newborn child is clarified by examination of the pharynx and a number of additional studies. Their goal is to determine possible pathologies of skull development, breathing disorders, smell, hearing and sound production.
Material and methods
The patients were examined jointly by a neurologist and an orthodontist. The study was carried out in 2 stages: the task of the first stage was to describe specific neurological disorders in patients with RHN; The task of the second stage was a comparative analysis of the frequency of identified neurological disorders in patients with RHN and in the control group.
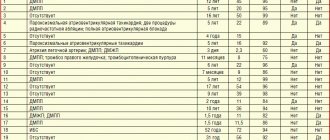
The main group consisted of 21 patients with RHN (13 females and 8 males, aged from 6 to 24 years; average age 12.0±4.7 years). The control group included 11 young people, 9 females and 2 males, who did not have RGN.
Based on the results of the examination, neurological symptoms were reflected in a specially designed questionnaire.
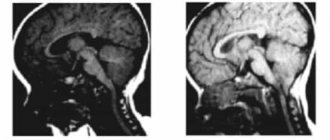
When examining patients, magnetic resonance imaging (MRI) of the brain was also used. It was carried out on MRI systems Signa HD (General Electric, USA) and Magnetom Espree (Siemens, Germany) with obtaining T1- and T2-weighted images (T1WI and T2WI, respectively) in orthogonal projections using standard pulse sequences of fast spin echo (Turbo or Fast Spin Echo - TSE or FSE, respectively) and T2VI based on a pulse sequence of fast inversion-recovery with signal suppression from free fluid (Fluid Attenuated inversion Recovery - FLAIR).
Statistical analysis of the data was carried out according to generally accepted rules; Fisher's exact test was used to assess intergroup differences. p were accepted as significant
<0,05.
Causes of cleft palate formation in humans
Experts do not have a consensus on the question of why children are born with a cleft palate. The appearance of the defect is associated with the presence of one or more provoking factors:
- inferiority of the germ cells of the parents: age over 40 years, hereditary gene mutations;
- infections and chronic diseases of the mother: rubella, chicken pox, herpes, syphilis, chlamydia, etc.;
- chemical intoxication: alcohol, drugs, smoking, chemicals, etc.;
- physical impact: amniotic fluid pressure, body overheating, radiation, falls, blows to the stomach, etc.
Often the cause of cleft palate is a metabolic disorder in the early stages of pregnancy, when it is accompanied by a lack of vitamins and minerals, toxicosis, lack of oxygen, and the threat of miscarriage. Taking antibiotics, sleeping pills and sedatives, medications for thyroid diseases, tumors, and arthritis can provoke a cleft palate in newborns. Psychological factors increase the risk of developing a defect: stress, prolonged experiences, lack of rest.