Various unforeseen situations can happen in our lives. No one can be insured against an accident. Often, in case of accidents, falls from a height, domestic injuries, or when engaging in combat sports, the chest is damaged.
This is a fairly broad group of injuries, which includes not only rib fractures, but also various injuries to internal organs. Often such injuries lead to significant blood loss, traumatic shock, and respiratory failure, which, in turn, can lead to serious health complications and even death.
All chest injuries can be divided into open and closed
Closed chest injuries
The main distinguishing feature is the absence of a wound. Let's look at the types of injuries and their clinical picture.
- Rib fractures:
- Chest pain that gets worse with breathing;
- Cyanosis of the skin and mucous membranes;
- Cardiopalmus;
- Both halves of the chest participate unevenly in the act of breathing;
- The chest is deformed;
- Localization of pain at the fracture site;
- Pathological mobility and bone crepitus.
You can read about how to provide first aid for fractures in our article.
- Chest concussion:
- Tachycardia, arrhythmia;
- Cyanosis;
- Frequent, shallow breathing;
- Changes in the depth and rhythm of breathing.
- Hemothorax:
Symptoms often vary depending on the degree. The most common sign of any hemothorax is an increase in body temperature after a chest injury. Hypoxia and shortness of breath may also increase.
- Pneumothorax:
- A sharp deterioration in general condition;
- Increased heart rate, increased shortness of breath;
- The skin is cold and cyanotic.
- Traumatic asphyxia.
- Increasing hoarseness of voice;
- Cyanosis of the upper half of the body;
- Swelling of the jugular veins;
- Increase in neck volume;
- Rapid development of cardiovascular failure.
- Traumatic asphyxia.
- Sharp blueness of the skin, especially the nasolabial triangle;
- Numerous pinpoint hemorrhages of the upper half of the body;
- Cough with bloody sputum;
- Hearing, vision, hoarseness.
Since vital organs are concentrated in the chest, damage to which can lead to serious consequences, emergency assistance to victims should be provided immediately.
Providing first aid for closed chest injury
- Call an ambulance;
- Place the victim in a semi-sitting position;
- Prohibit talking and breathing deeply;
- Carefully free the victim from constricting clothing (unbutton, cut);
- If the victim is unconscious, tilt his head back, slightly to one side;
- If the victim is conscious, take a painkiller (analgin, baralgin, etc.);
- Until the doctor arrives, do not leave the victim, monitor consciousness and pulse.
Types of chest bruises
Depending on the location of the lesion, chest contusions can be divided into:
- right-sided - risk of lung damage with possible rupture and bleeding;
- left-sided - risk of heart damage and death.
A bruise can be open with superficial wounds or closed, in which internal damage to soft tissues, bones, and organs is noted.
Doctors distinguish 3 degrees of bruises :
- Mild - treatment is possible at home.
- Moderate - complications are possible, so treatment must be carried out on an outpatient basis.
- Severe - hospitalization of the victim is required.
Open chest injuries
All open chest injuries are divided into: penetrating and non-penetrating.
Non-penetrating - usually applied with some object (knife, stick). The victim's condition is satisfactory, the skin is dry, there is slight cyanosis of the lips, no air suction is observed during inhalation, there is no cough or hemoptysis.
Such injuries do not pose a threat to life unless vital organs are damaged.
First aid for non-penetrating chest wounds
- Calm the victim;
- Call an ambulance;
- Apply a pressure bandage from any available material to the wound;
- Before the ambulance arrives, monitor the condition of the victim.
Penetrating – significantly worsen the victim’s condition. Appears:
- Severe chest pain;
- Shortness of breath, feeling of lack of air;
- The skin is pale, with a cyanotic tint, especially in the area of the nasolabial triangle;
- Sticky, cold sweat;
- The fall in blood pressure progresses, tachycardia increases;
- Both halves of the chest participate unevenly in the act of breathing;
- During inhalation, air is sucked into the wound;
- Foamy, bloody sputum and hemoptysis may appear.
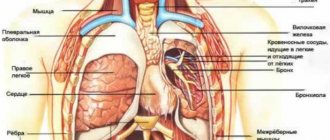
Most often, penetrating chest injuries can be accompanied by injuries to such organs as:
- Lungs;
- Intercostal vessels;
- Heart;
- Diaphragm;
- Mediastinal vessels;
- Trachea, bronchi, esophagus;
- Abdominal organs.
Emergency first aid for penetrating chest wounds
MUST BE PROVIDED IMMEDIATELY!
- Call an ambulance immediately;
- Do not leave the victim a single step, calm him down, sit him in a semi-sitting position;
- Prohibit deep breathing, talking, eating, drinking;
- For the first time, after identifying the patient, the wound should be covered with your hand;
- Next, they begin to apply an occlusive dressing from scrap materials. Before applying the bandage, the victim is asked to exhale deeply .
- The area adjacent to the wound is treated with a solution of skin antiseptic (iodine, chlorhexidine, brilliant green);
- The skin around the wound is lubricated with Vaseline or any greasy cream (if available);
- The first layer is any piece of clean bandage, gauze or any fabric so that the edges of the bandage are 4-5 cm from the edge of the wound; secure along the edge with adhesive tape.
- The second layer is any oilcloth, a bag folded several times. It is also secured with adhesive tape.
- Several rounds of bandage are made around the body from above.
- If there is a foreign object in the wound, under no circumstances should you try to pull it out. It needs to be fixed by covering the edge with napkins and securing with a bandage or adhesive plaster.
- If the wound consists of 2 holes (entrance and exit), the bandage is applied to both wounds.
- If help is provided to the victim after 40 - 50 minutes, then before the doctors arrive, the occlusive bandage is applied in the form of a U-shaped pocket, that is, it is attached only on 3 sides.
Any chest injuries are considered quite serious and dangerous injuries. Therefore, the correct, clear actions of the person who provides assistance to the victim will help preserve health and even life.
Publications in the media
Chest injuries account for 10–12% of traumatic injuries. A quarter of chest injuries are severe injuries requiring emergency surgical intervention. In peacetime, closed injuries predominate over open ones and account for more than 90% of all chest injuries.
Classifications • The classification of chest injuries accepted in Russia divides them into closed wounds and penetrating wounds of the chest •• Closed injuries ••• Soft tissue injuries ••• Damage (fractures) of bones ••• Injuries to internal organs •• Open injuries (wounds) ••• non-penetrating: injuries (wounds) of soft tissues, injuries (open fractures) of bones ••• penetrating: injuries of the pleura and lungs with hemothorax and/or pneumothorax, heart injuries, injuries of the esophagus •• Combined injuries ••• thoracoabdominal injuries •• • other injuries (damage to the chest in combination with injuries to the head, spine, etc.) • Classification of the College of Traumatology of the American Society of Surgeons. Injuries to the chest are divided into emergency conditions that directly threaten the life of the victim, and potentially life-threatening conditions.
Immediately life- threatening injuries can be fatal within minutes. Despite the significant diversity in the nature and intensity of disorders, first of all they must include: disorders of external respiration (respiratory), circulatory disorders (circulatory), shock • Obstruction of the respiratory tract quickly leads to hypoxia, acidosis and cardiac arrest. It is necessary to immediately ensure and maintain patency of the airways: remove secretions, blood, foreign bodies, perform tracheal intubation, cricothyroidotomy or tracheostomy (as indicated) • Pneumothorax and hemothorax • Cardiac tamponade occurs with the rapid accumulation of blood in the pericardial cavity (under the cardiac membrane), accompanied compression of the heart, a decrease in its filling in diastole and a decrease in cardiac output •• Clinical manifestations: arterial hypotension, tachycardia, a sharp weakening of the apical impulse, expansion of the borders of the heart, significant expansion of the veins of the neck. Localization of the wound in the projection of the heart makes it possible to timely suspect injury to the pericardium and myocardium •• Treatment: sternotomy or left anterolateral thoracotomy and rapid decompression of the pericardium. A left-sided anterior thoracotomy and pericardiotomy are performed, and the blood that has spilled into the pericardial cavity is evacuated. The myocardial injury is sutured. The pericardium is also sutured with separate rare sutures to ensure free outflow of the contents of the pericardial cavity into the pleural cavity • Pathological mobility of the chest wall - see Rib fractures.
Potentially life - threatening injuries are usually fatal if not treated promptly. However, the condition of the patients allows an accurate diagnosis to be made within a few hours and the necessary treatment tactics to be developed.
• Ruptures of the trachea and main bronchi usually occur within 2 cm of the tracheal bifurcation. More often observed with blunt chest injuries. Injury to the trachea and bronchi rarely occurs in isolation, usually in combination with damage to other organs of the mediastinum and thoracic cavity • • Diagnosis is made clinically, by radiography or bronchoscopy. Characteristic signs include severe respiratory distress, pneumothorax, mediastinal emphysema, subcutaneous emphysema, pneumothorax, hemothorax and hemoptysis. Suspicion of rupture should arise in the following cases: ••• The collapsed lung could not be expanded after drainage of the pleural cavity (decompression failure) ••• A large volume of air continues to enter the pleural cavity ••• Massive mediastinal and subcutaneous emphysema in the early stages after injury ( 1–2 hours) • • Treatment: restoration of the wall of the trachea and bronchus. If it is not possible to restore the integrity of the ruptured main bronchus with the vessels intact, both ends of the bronchus should be tightly sutured and the patient should be transferred to a specialized thoracic surgery center.
• Aortic rupture usually occurs due to acute and blunt trauma to the chest or sudden stoppage of body movement (car accident). When large vessels of the chest are injured, less than half of the victims reach the hospital: there are few conditions for thrombus formation, the wound usually gapes, which is accompanied by heavy bleeding. As a result, about 2/3 of the victims die • • Clinical manifestations: hemorrhagic shock, localization of the injury in the upper half of the chest, intense pulsating hematoma, noise on auscultation above it, hemopneumothorax • • X-ray ••• Widening of the mediastinum ••• Blurred contour of the aortic arch ••• Downward displacement of the left main bronchus ••• Shadow at the apex of the lung ••• Deviation of the trachea to the right ••• Fluid (blood) in the left pleural cavity • • Aortography: confirm the diagnosis • • Treatment. Emergency thoracotomy, restoration of the integrity of the aorta by suturing the wound or interposition of the graft. Usually performed using a heart-lung machine.
• Injury to the diaphragm usually occurs with open and closed injuries to the chest and abdomen. In this case, the pleural and abdominal cavities communicate with each other •• The diagnosis is established using radiography, revealing the displacement of the stomach or colon into the chest. All penetrating wounds of the chest below the level of the VII rib are dangerous due to possible damage to the diaphragm. Therefore, if the clinical picture is unclear, these patients are indicated for diagnostic thoracoscopy •• Treatment. Immediate insertion of a nasogastric tube (if one has not previously been placed) prevents significant gastric dilatation, usually accompanied by severe, life-threatening respiratory distress. Then, ruptures in the diaphragm are urgently sutured (via transabdominal access) and at the same time the associated injuries to the abdominal organs are eliminated. The pleural cavity is drained.
• Damage to the esophagus most often occurs with penetrating wounds of the chest or with iatrogenic damage during esophagoscopy •• Clinical manifestations: immediate development of subcutaneous emphysema in the neck and rapidly progressing mediastinitis •• Diagnosis: X-ray examination of the esophagus with water-soluble contrast •• Treatment. Wide drainage of the mediastinum and suturing of the rupture should be performed as soon as possible. Access depends on the location of the rupture: either through the soft tissue of the neck or by performing a thoracotomy. The sutures are usually covered and reinforced with surrounding tissue (pleura, intercostal muscles).
• Cardiac contusion occurs with direct blows to the sternum. The severity of the manifestations of cardiac tissue contusion ranges from minor subendocardial or subpericardial petechiae to damage to the entire thickness of the myocardium • • Clinical picture: pain in the heart area, rarely relieved by validol, nitroglycerin, anxiety, fear, feeling of suffocation, weakness. The skin is earthy-gray in color, cold sweat, weak pulse, arrhythmic, tachycardia up to 140–150 per minute. On auscultation - dullness of tones, arrhythmia, arterial hypotension. On the ECG - decreased voltage, increased, flattened, biphasic or inverted T wave, deformation of the QRS complex • • Complications ••• Arrhythmias (including ventricular extrasystoles, supraventricular tachycardia and atrial fibrillation) ••• Ruptures of the myocardial walls ••• Ruptures of the interventricular septum • •• Left ventricular failure • • Diagnosis is based on the results of ECG and two-dimensional echocardiography • • Treatment: constant monitoring of cardiac activity and hemodynamics using monitoring equipment, treatment of arrhythmias with appropriate drugs, and with the development of cardiogenic shock - appropriate intensive care.
• Pulmonary contusion is the most common injury, accompanying extensive chest injuries in 30–75% of cases •• Causes. Closed injury causing intra-alveolar hemorrhages, edema and bronchiole obstruction •• Diagnosis is based on chest x-ray data (shading of lung tissue in the first hours after injury), gas composition in arterial blood and clinical signs of respiratory distress •• Treatment: restriction of fluid intake , oxygen inhalation, physiotherapeutic procedures, adequate pain relief (including epidural analgesia). If complications occur (pneumo- and hemothorax), emergency drainage of the chest cavity is performed.
• Mediastinal emphysema and subcutaneous emphysema •• Subcutaneous emphysema most often occurs with tension pneumothorax and rupture of the parietal pleura, which corresponds to a typical injury - a lung rupture with rib fractures or penetrating injury. With an intact parietal pleura, air enters the soft tissues of the chest from the mediastinum through the superior thoracic aperture. It is possible to develop extensive subcutaneous emphysema with a closed rupture of the bronchus or lung and preserved parietal pleura. It is necessary to distinguish between limited, widespread and total subcutaneous emphysema • • Mediastinal emphysema (pneumomediastinum) occurs when a bronchus (less commonly the trachea) ruptures while maintaining the integrity of the mediastinal pleura (air spreads through the paratracheal and mediastinal spaces). Another cause of pneumomediastinum is a complication of laparoscopy (when the insufflated gas, instead of the abdominal cavity, enters the preperitoneal tissue and then into the anterior mediastinum) ••• Clinical manifestations. Symmetrical swelling in the supraclavicular areas, quickly spreading to the neck and face. Hoarseness, extrapericardial cardiac tamponade. On palpation - a symptom of “crispy snow” (crepitus) ••• Treatment. With progressive mediastinal emphysema with dysfunction of the cardiovascular system and respiratory system, emergency suprasternal mediastinotomy is indicated: local anesthesia, procaine is sequentially injected into the skin, subcutaneous tissue and retrosternal space. A horizontal incision is made above the manubrium of the sternum and, sliding along the posterior wall of the sternum, carefully penetrates the mediastinum. Then drainage is installed and guiding sutures are applied.
• Chest compression (traumatic asphyxia). With prolonged and strong compression of the chest, almost complete or partial holding of breath occurs, entailing an increase in intrathoracic pressure with a sharp increase in pressure in the intrathoracic blood vessels. The outflow of venous blood through the system of the superior vena cava to the right side of the heart is disrupted •• Clinical picture: consciousness is often impaired, patients complain of chest pain, tinnitus, hoarseness, often aphonia, bleeding from the nose and ears is possible. The patient's appearance is characteristic: the skin of the head, neck, and upper half of the chest is bright red with multiple pinpoint hemorrhages spreading to the mucous membranes of the oral cavity, eardrums, conjunctiva and retina. In places where clothing fits tightly, there may be no bleeding on the skin. In severe cases - shortness of breath, weak rapid pulse, arrhythmias, arterial hypotension. On auscultation - a large number of moist rales, on the radiograph - various darkening of the pulmonary fields •• Treatment. For mild traumatic asphyxia - rest, cervical vagosympathetic novocaine blockade according to A.V. Vishnevsky, oxygen therapy. For severe traumatic asphyxia - mechanical ventilation, resuscitation, intensive care.
ICD-10 • S20 Superficial injury to the chest • S21 Open wound of the chest • S22 Fracture of the rib(s), sternum and thoracic spine • S23 Dislocation, sprain and damage to the joints and capsular ligament apparatus of the chest • S24 Trauma to nerves and spinal cord in the thoracic region • S25 Injury to the blood vessels of the thoracic region • S26 Injury to the heart • S27 Injury to other and unspecified organs of the thoracic cavity • S28 Crushing of the chest and traumatic amputation of part of the chest • S29 Other and unspecified injuries of the chest
Rib fractures
Single rib fractures, as a rule, occur as a result of direct trauma - at the point of application of force (impact, pressing against a certain object). Double rib fractures occur. When the chest is compressed in the anteroposterior direction, several ribs break along the axillary line, and in the lateral direction, along the paravertebral and midclavicular lines. Multiple bilateral rib fractures occur in severe road traffic injuries, rubble, etc. Sometimes a sharp fragment of a rib can damage intercostal vessels, perforate the parietal pleura and even injure the lung.
Symptoms . The patient complains of sharp pain at the fracture site, which increases with inspiration. The general condition of the patient depends on the severity of the injury (number of damaged ribs, degree of lung failure, hypoxia, blood loss, pleuropulmonary shock, etc.).
With single rib fractures, the patient's general condition remains satisfactory. The patient spares the chest and breathes shallowly. Due to the pain, he cannot cough up the mucus that accumulates in the upper respiratory tract, and therefore gurgling appears, and over time, pneumonia can develop. Hemoptysis indicates lung damage.
During palpation, the points of maximum pain are determined. If you squeeze the chest lightly, local pain increases, and the patient points to the fracture site. With double fractures of the ribs (fenestrated fracture), when inhaling, this area sinks, and when exhaling, it levels out. Such flotation of the chest wall with each breath is very painful, which affects the nature of breathing, the function of the organs of the mediastinum, which also floats, and the general condition of the patient.
Multiple and especially bilateral rib fractures cause severe respiratory distress, hypoxia and traumatic pleuropulmonary shock. The examination of the patient includes chest x-ray, percussion and auscultation to identify rib fractures and possible complications - hemothorax, pneumothorax, etc.
Treatment for uncomplicated rib fractures
If individual ribs are damaged, treatment is limited to pain relief, improvement of breathing conditions and prevention of pneumonia.
The patient is placed in a semi-sitting position in bed. A local or paravertebral blockade is performed with a 1% novocaine solution, and analgesics are prescribed. After anesthesia, chest excursion improves, and breathing becomes smooth and deep, the patient can even cough up sputum, which prevents the occurrence of pneumonia. The blockade is repeated 2-3 times. In addition, patients are prescribed breathing exercises and symptomatic therapy. Fractured ribs heal in 3-4 weeks, performance is restored in 5-6 weeks.
In case of multiple rib fractures (four or more), complex treatment is carried out, which is determined by the severity of the patient’s condition. In order not to disturb a seriously ill patient with repeated blockades and to maintain constant pain relief, a thin tube (vascular catheter) is inserted into the paravertebral area through a needle, which is left, glued with an adhesive plaster to the chest wall, and its second end (catheter cannula) is brought out to the shoulder girdle. When pain occurs, without moving the patient, 15-20 ml of a 0.5% novocaine solution is injected into the catheter (4-5 times a day).
Patients with severe breathing disorders are also treated with cervical vagosympathetic blockade according to A.V. Vishnevsky and undergo intensive therapy, and sometimes resuscitation measures (intubation, mechanical breathing, etc.).
In case of double fenestrated fractures of the ribs, in order to eliminate flotation, under local anesthesia, the ribs are fixed with Kirschner wires passed percutaneously, or they are applied to the sinking area of extraction (stitching behind the soft tissues and periosteum of the middle rib with a coarse Mylar thread or using bullet forceps). Ribs fixed using the following methods fuse in normal time. Open osteosynthesis of ribs is used extremely rarely.
Complex treatment also includes oxygen therapy, suction of mucus from the trachea, antibiotic therapy, etc.