Osteoplastic operations are becoming more and more improved every year, as their demand increases. According to statistics, bone deficiency due to one reason or another occurs in every second dental visitor. In the vast majority of cases, insufficient jaw volume is detected before dental implantation. One of the most popular and reliable operations to restore the amount of bone in the upper jaw is considered to be a sinus lift.
Indications for its implementation:
- Long-term absence of anterior premolars and molars, which leads to resorption of bone tissue;
- Resolved inflammatory processes affecting bone tissue;
- Traumatic injuries to the jaw (most often surgical tooth extraction);
- Congenital structural features of the upper jaw and maxillary sinuses (physiological deficiency of bone tissue).
Depending on the severity of the bone tissue deficiency, open or closed volume restoration surgery is performed. The essence of the surgical intervention is to separate the mucous membrane lining the maxillary sinus, followed by filling the resulting cavity with bone grafts of various types. However, in the process of preparing for surgery, and sometimes during its implementation, obstacles to the procedure may be discovered. Most often, such unfavorable factors are cysts in the maxillary sinus.
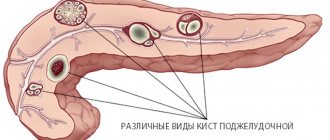
What is a cyst in the maxillary sinus called?
A maxillary sinus cyst is a benign formation that has a hollow structure containing fluid inside. Cysts of the maxillary sinuses are quite common, but are almost always found at random. Their location and origin may differ, which will determine the characteristics of the clinic and even treatment.
Odontogenic cyst
Among the many benign tumors of the jaw tissue, the cyst is found most often and represents a pathology quite dangerous for the bone structure. Odontogenic formations in the vast majority of cases remain undiagnosed for a long time, and therefore reach enormous sizes. The growth of the cyst provokes atrophic processes in the bone tissue, which thins, becomes fragile, and then disappears completely.
Such formations are characterized by a long latent course until the cavity grows to gigantic proportions. Then a characteristic crunch begins to be noted in the jaw, especially during chewing loads. Ignoring the problem leads to spontaneous fractures of the jaw, compression of the maxillary sinus with disruption of its functions, exacerbation of the inflammatory process with damage to the structures of the maxillary sinus and the formation of sinusitis.
Tooth cyst growing into the maxillary sinus
Damage to the dental canal involving the root and surrounding tissues is a consequence of an infectious process of bacterial origin. In the absence of adequate and timely treatment, a gradual delimitation of the inflammatory reaction from healthy tissues by a wave of cellular structures occurs.
This creates a cavity called a dental cyst. It gradually increases and destroys the bone tissue of the jaw. When localized in the anterior part of the upper jaw, gradual penetration into the maxillary sinus occurs.
Retention
The most common form of neoplasm in the maxillary sinus, which is also called a true cyst. It is located in the lower wall of the sinus and has an epithelial lining - a distinctive feature of true cystic cavities. The formation is clearly determined by X-ray examination randomly, as it does not manifest itself clinically.
When the cyst reaches a significant size, problems begin with the functioning of the maxillary sinus. The structure and physiology of the microvasculature is disrupted, resulting in the formation of edema. This symptom is manifested by nasal congestion, often without pronounced discharge from it. Due to the lack of specificity of the clinical picture, even the presence of subjective signs of the disease is not a reason to consult a doctor.
results
The classification of cysts, which has not lost its relevance today, was proposed by M.I. Kadymova [7]: true or retention cysts; false or cyst-like formations; odontogenic cysts; cysts associated with developmental defects.
In the English-language literature, a distinction is made between secreting cysts (retention cysts) and non-secreting cysts (pseudocysts).
Retention cysts are formed as a result of obstruction of the excretory ducts of the glands of the mucous membrane [8]. Histological examination shows that retention cysts are bilaterally lined with ciliated columnar epithelium; the cyst wall consists of connective tissue with the presence of coarse collagen fibers [9]. On spiral CT (SCT), such cysts appear as round, homogeneous soft tissue formations on a broad base, with clear boundaries, without signs of bone destruction, and without connection with the roots of the teeth.
False (lymphectatic) cysts are located intramurally in the mucous membrane and do not have an internal epithelial lining, which is their only histological difference from retention cysts.
Presumable causes of the formation of false cysts are barotrauma, allergic and inflammatory diseases of the sinuses [3, 10, 11]. According to the results of a study by O. Berg et al. [10] revealed a high content of immunoglobulins, complement and antiproteases in aspirates from intramural cysts, which, along with the bacterial microflora present in them, supports the inflammatory theory of their origin, however, the content of immunoglobulin E (IgE) and eosinophils was within normal limits. The identity of the detected bacterial flora with the oral microbiota allowed the authors to assume that the basis for the formation of intramural cysts is formed by the residual part of the dental leaf.
Several prospective comparative studies have examined the associations between sinus cysts and sinus mucosal pathology and drainage disorders. J. Kanagalingam et al. [12] found no correlation between the occurrence of intracranial cysts and allergies, asthma, or ostiomeatal complex block. The lack of correlation between intracranial cysts and the state of the ostiomeatal complex was confirmed in other studies [13–15].
However, R. Harar et al. [14] noted that in the presence of a cyst, changes in the sinus mucosa, characteristic of chronic rhinosinusitis, are detected on SCT more often than in its absence (52.7 and 41.3%, respectively). The authors concluded that it is theoretically possible for a cyst to form due to transient obstruction of the ostiomeatal complex with subsequent preservation of the ICP after restoration of its patency.
Possible clinical manifestations of an upper lip cyst described in the literature are very diverse: headache and facial pain, difficulty in nasal breathing, postnasal drip, rhinorrhea, sudden discharge of amber fluid from the nose (which is associated with spontaneous rupture of the cyst), numbness of the upper lip, pain in the teeth, etc. [16-19]. However, in many cases the description of symptoms does not contain evidence of their connection with the cyst.
In this regard, the study of F.V. is of interest. Semenova et al. [16]. The authors assessed the dynamics of complaints from 67 patients operated on for upper-crural cysts by questioning patients before and after the intervention, followed by data processing using mathematical statistics methods. Of the 14 symptoms indicated by patients as a reason to see a doctor, 4 disappeared after removal of the cyst: headache (mainly in the frontal region), a feeling of pressure in the projection of the affected sinus, difficulty in nasal breathing and clear nasal discharge/postnasal drip ( p
<0.01). The authors concluded that these symptoms can most likely be associated with the presence of large cysts of the cervical cavity.
If anatomical abnormalities are present, ICP cysts may cause unusual symptoms. N. Sharma et al. [20] described transient paresthesia in the facial area in a patient with a cyst of the upper jaw and dehiscence of the infraorbital nerve canal. The association of paresthesia with the cyst was confirmed by its disappearance after removal of the cyst.
However, in a number of prospective comparative studies, no correlation was found between ICP cysts and sinonasal symptoms [12, 15]. S. Albu [15], in a prospective randomized study of 80 patients, found no correlation between cyst size and facial pressure or nasal obstruction or nasal discharge.
Often, VCP cysts do not manifest themselves at all and are an accidental finding. In a study conducted by the author of this review [21], asymptomatic cysts were identified in 37 out of 177 apparently healthy people (20.9%) who underwent SCT of the SNP for the purpose of occupational selection.
Patients with cysts of the upper jaw often undergo surgical interventions in the absence of any complaints. This is apparently due to concerns among some doctors that the cysts may grow larger and cause complications over time. In this regard, long-term observations using modern imaging methods that evaluate changes in the size of SNP cysts over time are of particular interest (see table).
Changes in the size of intracranial cysts during long-term follow-up
As follows from the summary table of the studies, an increase in the size of the cyst was observed only in 12.7% of patients, in 18.3% it disappeared, in 12.2% it decreased in size, and in 56.8% it remained unchanged.
Based on long-term observation of 18 patients, J. Wang et al. [24] came to the conclusion that if the size of the sinus cyst did not change over 48 months, then they will remain unchanged in the future, although P. Casamassimo and G. Lilly [25] did not note a dependence of the change in the size of the cyst on the observation time.
The most extensive of the studies listed in the table is the work of I. Moon et al. [2] - describes the dynamics of changes in the size of SNP cysts in 133 patients who underwent MRI of the brain for the purpose of preventive examination more than 2 times with a follow-up period of at least 24 months.
The average follow-up period was 40.38±16.09 months (from 24.0 to 109.8 months). In 119 out of 133 patients, during the initial study, cysts were found in the upper jaw, ranging in size from 13.35±9.22 to 15.49±6.94 mm. During follow-up from 24 to 36 months, the size of the cysts remained unchanged in 73% of patients, in 22% they decreased or disappeared, and only in 5% of cases there was an increase in the size of the cyst. Subsequently (more than 48 months), changes in the size of the cysts occurred in a greater number of cases: the sizes of 42% of cysts remained unchanged, 43% decreased or disappeared, and in 15% of cases the cysts increased.
Obstruction of the sinus anastomosis was detected only in 6 (4.5%) patients. The addition of rhinosinusitis during observation was registered in 4 (3.0%) of 133 patients, and in 3 of them there was an increase in the size of the cyst.
Summarizing the data from the studies presented in the table, it should be emphasized that spontaneous regression (reduction or disappearance) of the cyst occurred in 30.5% of cases. The results of the study by I. Moon et al. [2], which had the longest observation period and the maximum number of patients included in it, showed that over time, an increasing number of cysts underwent regression, and the addition of complications was insignificant (3%).
Taking into account these data, the opinion of many researchers [12, 15, 25—28], who believe that the majority of patients with cervical cysts do not require surgical treatment, is quite justified. I. Moon et al. [1] believe that only large cysts that cause obstruction of the sinus anastomosis require removal.
The development of modern rhinosurgery was marked by the introduction into practice of gentle methods for removing cysts of the upper jaw, which replaced the Caldwell-Luc method.
Today, the three most common surgical approaches are:
— gentle opening of the sinus through the anterior wall using a bur or trocar;
- endoscopic endonasal access through the middle meatus,
— endoscopic antrostomy through the lower nasal passage, as well as a combination of these approaches [26, 29—31].
In recent years, a few publications have appeared on the use of the balloon sinuplasty method for the removal of cervical cysts [32, 33].
To select an adequate surgical approach, SCT of the SNP is of great importance, allowing to determine the localization of the cyst, while an important role is played by sagittal reconstruction, which makes it possible to assess the relationship of the cyst with the anterior and posterior walls of the sinuses [26, 34, 35].
In 70% of cases, cysts of the upper sinus are localized on the postero-superior wall, in the lateral parts of the upper wall and in the area of the natural sinus anastomosis, which makes it possible to remove them using the endonasal approach through the middle meatus [26]. In cases where the cyst is localized on the anterior and medial walls of the upper jaw, as well as in the alveolar bay, the endonasal approach through the middle meatus often does not allow complete removal of the cyst and, therefore, other options or a combined approach are required.
A number of authors prefer antrostomy through the lower nasal meatus, explaining its advantage by the preservation of the natural anastomosis [28, 36], as well as convenience, simplicity of surgical technique and good visibility of the sinus [37].
Unfortunately, in the available literature, only a few studies have been found on the frequency of recurrence of intracranial cysts after the use of various sparing access techniques. One of these studies was published by T.V. Banashek-Meshcheryakova, F.V. Semenov [37]. The authors conducted a comparative analysis of the results of removal of intracranial cysts in 120 patients. The patients were divided into 3 groups of 40 people each and operated on via endonasal access through the middle and lower nasal meatus (2 groups) and extranasal access. During a postoperative observation period of 6 months, cyst recurrence was recorded in only 3 (7.5%) patients operated on through the middle meatus. There were no relapses with other access options.
How to identify a cyst in the maxillary sinus?
Since cystic cavities are benign neoplasms, they do not cause any systemic manifestations. The local clinical picture manifests itself several months after the onset of the pathological process. But even its occurrence does not always become a reason to go to the doctor. Most often, maxillary sinus cysts are discovered by a dentist during a preliminary examination to perform a sinus lift or implantation.
The main clinical manifestations of cysts in the maxillary sinus:
- Painful sensations in the infraorbital region of a pressing nature (pain intensifies when changing body position);
- Discharge from the nasal passages is purulent or mucopurulent in nature, the amount of which depends on the presence and severity of the inflammatory process;
- Gradually increasing facial asymmetry (when the cyst reaches a large volume);
- Constant exacerbations of infectious lesions of the maxillary sinus;
- Swelling of the nasal passages (severe nasal congestion);
- Pain in the upper jaw (as well as: a characteristic crunch when pressed or loaded);
- Headaches (most often in the forehead or temples).
The clinical picture of cystic formations is practically indistinguishable from acute sinusitis, so doctors always differentiate these two pathologies using instrumental studies. For dental specialists, it is especially important to make the correct diagnosis, since the presence of a cyst is not always a contraindication for sinus lifting, but an acute infection does not allow surgical intervention.
Identification of cystic formations occurs by performing x-rays of the sinuses or in the process of studying the bones of the skull on a computed tomography scan. Additionally, an endoscopic examination may be prescribed, which is both diagnostic and therapeutic. Histological examination using targeted biopsy is mandatory, which allows us to have an idea of the origin of the tumor and exclude malignant oncology.
Contraindications
The operations for removing sinus cysts are quite simple. Patients recover quickly after the intervention, and complications are rare. Contraindications are only general for any surgical interventions:
- acute infection;
- diabetes mellitus (severe);
- increased bleeding (blood does not clot well);
- pregnancy;
- epilepsy;
- oncology.
Before surgery to remove a cyst from the sinus, you need to take tests (for HIV, syphilis, hepatitis B and C, general blood test).
Treatment of maxillary cysts
There are no conservative methods for treating cystic formations in the maxillary sinus. The doctor chooses one of the options for surgical intervention, which depends on the type of cyst, its location, the professional qualities of the specialist and the individual characteristics of the patient.
In modern medicine, the following operations are widely used to treat cysts:
- Open surgery. A manipulation that involves general anesthesia and has many complications and risks. The anterior wall of the maxillary sinus is opened, and the cyst is removed through the resulting hole. The main problem is the overgrowing of the access with scar tissue. This completely contradicts the physiology of the body and does not allow sinus lifting and dental implantation in this area in the future.
- Endoscopic treatment. One of the most advanced and successful in modern medicine. Using a special instrument, the doctor enters the maxillary sinus through its natural opening without damaging the bone tissue. The cyst is then sucked out or desquamated.
- Classic removal. A typical open sinus lift approach is performed, through which the cyst is removed. The operation is performed in cases where the cause of the development of the formation is a diseased tooth.
Since cystic formations are most often discovered during the preliminary examination for sinus lift, the doctor must choose a treatment method that will not interfere with further bone grafting. The final decision always belongs to the patient, so he needs to be told the advantages and disadvantages of each therapeutic technique.
List of sources
- Zakharova, G.P. Clinic, pathogenesis and surgical rehabilitation of patients with cyst-like formations of the maxillary sinuses / G.P. Zakharova // Sat. scientific tr. XV Congress of Otorhinolaryngologists of Russia. - St. Petersburg, 1995.-T. 1.-S. 96-102.
- Daynyak, L.B. Nose and paranasal sinuses / L.B. Daynyak // Guide to otorhinolaryngology. M.: Medicine, 1994. - P. 222.
- Guryev I.S., Dolzhikov A.A. Features of patho- and morphogenesis of cysts of the paranasal sinuses. Russian rhinology. 2002; 2:53-54.
- Allahverdiev S.A., Lopatin A.S. Choosing the optimal surgical approach for maxillary sinus cysts. Russian rhinology. 2010;(1):34-35.
- Kulakov A. A. Surgical dentistry and maxillofacial surgery. National leadership / ed. A. A. Kulakova, T. G. Robustova, A.I. Nerobeeva. - M.: GEOTAR-Media, 2010. - 928 p.
Cyst in the maxillary sinus and sinus lift
Many patients are interested in the question of whether it is possible to simultaneously extract a cystic formation and perform bone grafting of the upper jaw. The answer to this question depends on several factors, which include:
- The degree of severity of bone tissue atrophy at the site of the cyst (in some cases, the deficiency is so pronounced that sinus lifting becomes impossible, and patients can only hope for the installation of removable dentures);
- The presence of an active inflammatory process (cysts are often complicated by infectious pathologies, especially sinusitis, which are a direct contraindication for surgery);
- The size of the cystic formation (small cavities can be removed immediately before sinus lifting, but if the cyst occupies the entire space of the sinus, then bone grafting is out of the question);
- The location of the cyst (if it is located on the lower wall, then problems with removal during sinus lifting usually do not arise, but if the formation is located higher, the dentist simply will not be able to reach it without injuring the walls of the sinus).
Performing a sinus lift with preliminary removal of a cystic formation is performed quite rarely and only in cases where the process has just begun to develop and was accidentally discovered by instrumental studies. The doctor must correctly weigh the benefits and risks of future surgery. Most often, patients are transferred for treatment to ENT specialists, and the sinus lift is postponed to a later time.
Diagnostic methods
If you suspect this pathology, you should consult a doctor - a dentist or otolaryngologist. The doctor will listen to your complaints, conduct an examination and prescribe additional tests. Based on the clinical picture, one can only suspect the presence of a pathological process in the projection of the upper quadrant. To clarify the diagnosis, additional examination is necessary.
| Research method | Explanation |
| Survey radiography | Plain radiography is the most accessible diagnostic method. It is carried out in two projections (direct and lateral). Plain radiography allows you to identify changes in the upper jaw, but this is not enough to determine the nature and localization of the pathology. |
| Contrast radiography | To clarify the location and size, contrast radiography is prescribed. A contrast agent is injected into the sinus through a natural opening, then an image is taken. |
| Probing | Probing makes it possible to penetrate the sinus cavity without opening it. |
| Computed tomography (CT), magnetic resonance imaging (MRI) of the brain | CT and MRI are the most informative research methods. They allow you to accurately determine the location of the cystic formation, its size and contours. |
Computed tomography and magnetic resonance imaging are the most accurate methods for diagnosing an intracranial cyst.
Possible risks
A cyst in the maxillary sinus and sinus lifting can be complicated in different ways and seriously interfere with any dental interventions by the doctor. When a cystic formation is removed, the risk of perforation of the mucous membrane of the maxillary sinus only increases, as do subsequent associated problems. It is also possible for the cyst to accidentally open and spill its contents into the sinus. This threatens further infection and the development of acute or chronic sinusitis.
When performing a sinus lift for a maxillary sinus cyst, the doctor must remember that the formation promotes the resorption of bone tissue. The thinner the alveolar bone, the less load it can bear. Therefore, any careless movement can lead to a fracture of the bone crest.
During the sinus lifting process, a barrier membrane is necessarily installed that will protect the operated area from unfavorable external factors and the additional impact of osteoclasts (cells that destroy bone).
In addition, only the safest and highest quality grafts are used in the bone grafting process with minimal risk of rejection. This precaution is due to the fact that a significant deficiency of bone tissue will not suffer additional problems in the form of poor engraftment. The doctor will not be able to perform a second operation, and he will have to look for alternative solutions.
Rehabilitation period
Figure 4. A cyst removed from the maxillary sinus with a tooth in it.
Source: Indian journal of ophthalmology / Open-i (Attribution 2.0 Generic) After surgery to remove a sinus cyst, no special recovery or treatment is usually required. Full recovery takes only a few days. With a small amount of intervention, patients feel well within a few hours after the intervention.
For the first time after surgery, it is advisable to avoid physical activity. You cannot visit the pool and sauna, you must not allow injuries. To avoid inflammation and other complications, you need to ensure high-quality oral hygiene and follow your doctor’s prescriptions.
Our doctors
Debryansky Vladimir Alekseevich
Doctor - otorhinolaryngologist, doctor of the highest category
33 years of experience
Make an appointment
Zharova Galina Gennadievna
Doctor - otorhinolaryngologist, member of the European Society of Rhinologists, doctor of the highest category
Experience 39 years
Make an appointment
Gogolev Vasily Gennadievich
Doctor - otorhinolaryngologist
19 years of experience
Make an appointment
What can you do to avoid getting sick?
You can reduce the likelihood of developing the disease by following simple rules:
- Brush your teeth twice a day. Use a high-quality brush and paste during hygiene procedures. Don't forget about the role of dental rinses and dental floss.
- Once a year, remove tartar in the dental office using an ultrasonic scaler. Professional hygiene is the best prevention of most dental ailments.
- Eat a balanced and healthy diet. Eat less sweets. Eat plenty of fresh fruits and vegetables.
- Check your dental health once a year. You need to visit a doctor, even if nothing bothers you.
- Always follow your dentist's instructions.
- Avoid traumatic injuries to the face. When engaging in potentially dangerous sports, always wear special protective equipment.
A jaw cyst is a dangerous tumor. Initially it is benign, but under certain conditions it can become malignant. Fortunately, this happens extremely rarely.
If the tumor grows very quickly, even a jaw fracture is possible. It shouldn't come to this. Treatment must be timely and competent.
Symptoms of the disease
In the first days of development of the pathology, there are no subjective symptoms. But the larger the cyst becomes, the stronger and more vividly it declares itself. Then a kind of gumboil may form in the gum area. At first, the protrusion does not hurt during palpation and hardly bothers the patient.
On an orthopantomogram, the doctor observes a spherical cavity with clearly defined contours. On an x-ray, you can see the root of the affected tooth with inflamed periodontium.
In advanced cases, when a large amount of purulent mass accumulates inside the cavity, the patient experiences the same symptoms as with osteomyelitis. Then the tumor volume increases. The gums swell and become very painful. Periodically, a small hole appears in its wall through which pus is released.