When carrying out diagnosis and treatment, it is necessary to establish the location of the damage, the degree of stenosis and its causes. Therefore, patients are prescribed a wide diagnostic program, as well as treatment methods - today they are varied and effectively eliminate the problem.
Most often, the disease affects extracranial vessels, but pathology of intracranial arteries also occurs. This condition is responsible for half of the clinical cases of cerebral ischemia and about 30% of strokes. There are complete and incomplete obstruction (blockage) of the vascular lumen, which lead to disruption of the blood supply.
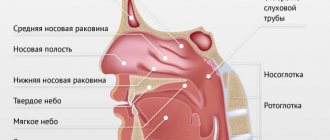
Normally, the common carotid arteries arise: the left one from the aortic arch, and the right one from the brachiocephalic trunk. They are directed vertically and are located on either side of the cervical spine. Next, it divides into the external and internal carotid arteries. The branches of the arteries supply blood to the intracranial parts, parts of the face, and organs of the head and neck.
What's happened
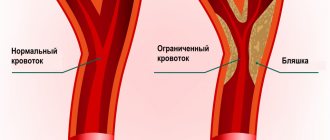
First, it’s worth understanding what a carotid artery is: in the human body there are two carotid arteries, running from the chest through the sides of the neck to the head. Their main task is to nourish the brain. Like any artery, they are confirmed by atherosclerosis - a serious disease, the nature of which is not fully understood, as well as the causes. This disease manifests itself in the deformation of the walls of blood vessels, when the tissues lining the vessel grow, cholesterol deposits appear between them, and the lumen of the vessel becomes smaller and smaller until it becomes completely blocked (obstruction). Oxygen-enriched blood flows through the carotid arteries for brain cells, so narrowing the lumen of the vessel is very dangerous - it can cause a stroke.
References
- "Medihaler Ergotamine." drugs.com
. Retrieved 2016-05-20. - Michael P. Walsh; et all (August 2005). "Thromboxane A2-induced contraction of rat caudal artery smooth muscle involves activation of Ca2+ entry and Ca2+ sensitization: Rho-associated kinase-mediated phosphorylation of MYPT1 at Thr-855 but not Thr-697." Biochem.
J. _
389
(Pt 3): 763–74. Doi:10.1042/BJ20050237. PMC 1180727. PMID 15823093. - Yagiela Y.A. (1995). "Vasoconstrictors for local anesthesia." AnesthProg
.
42
(3–4): 116–20. PMC 2148913. PMID 8934977. - Moodley, D.S. (2017). “Local anesthetics in dentistry. Part 3: Vasoconstrictors in local anesthetics" (PDF). South African Dental Journal
.
72
: 176–178. - ^ a b c
Unless otherwise noted in the box, ref: Walter F. Boron (2005).
Medical Physiology: A Cellular and Molecular Approach
. Elsevier/Saunders. ISBN 1-4160-2328-3. Page Reshebnika 479 - ^ a b c d f g g hour i j
Wand Flower;
Humphrey P. Rang; Maureen M. Dale; Ritter, James M. (2007). Pharmacology of Rang and Dale
. Edinburgh: Churchill Livingstone. ISBN 978-0-443-06911-6. - Walter F. Boron (2005). Medical Physiology: A Cellular and Molecular Approach
. Elsevier/Saunders. ISBN 1-4160-2328-3. Page Reshebnika 771 - Richard Milsten and Julian Slowinski, Sexy Masculine
, bc, highlight WW Norton Company, New York, London (1999) ISBN 0-393-04740-7
Causes and prevention
The causes of vasoconstriction are being actively studied, but there is still no clear understanding. A hereditary cause is identified, and everything else can be attributed to risk factors. Among them:
- arterial injuries,
- obesity,
- smoking,
- diabetes,
- sedentary lifestyle,
- older age,
- high level of “bad cholesterol” in the blood (low-density lipoproteins are a combination of cholesterol and protein that do not take excess cholesterol from the vessels, but, on the contrary, attach them to the walls, forming cholesterol plaques).
Prevention of carotid artery stenosis, like any other arteries, consists of maintaining a healthy active lifestyle and a balanced diet to prevent an imbalance in the ratio of low- and high-density lipoproteins, and therefore the development of atherosclerosis.
Screening for asymptomatic carotid artery stenosis
Prophylactic endarterectomy is indicated in patients who have a low risk of surgical complications and high-grade atherosclerotic stenosis of the carotid artery. However, no consensus has been reached on how best to screen these patients. The presence of a murmur over the carotid artery is a poor predictor of severe carotid artery stenosis. For example, in the third of 330 consecutive patients who were admitted to the cerebrovascular clinic, there was a small murmur over the carotid artery, and its positive predictive value was less than 37% for the detection of carotid artery stenosis of the middle artery this is an important step. Patients with multiple risk factors, such as smoking, hypertension, and ICS, have a high likelihood of demonstrating atherosclerotic disease in the carotid arteries even before they undergo a blood level test. Therefore, it is important to carry out screening of the carotid arteries in patients, if there may be evidence of vascular risk factors and noise over the carotid arteries.
Symptoms of carotid artery stenosis
The disease is dangerous because the symptoms are practically invisible, and only when stenosis becomes the cause of other pathological conditions does a person consult a doctor. Among such conditions, ischemic attacks (mini-stroke, small stroke) are primarily distinguished, when the blood supply to the brain is disrupted for a short period of time. This condition manifests itself as follows:
- numbness of hands/arms,
- speech distortion,
- temporary loss of vision, visual acuity,
- temporary disorientation,
- numbness of the face.
And more general symptoms
- headache,
- nausea,
- weakness.
Carotid artery stenosis develops slowly, often asymptomatically, and people attribute general fatigue and increased fatigue to excessive stress or the weather. Therefore, doctors recommend carefully monitoring your condition, and, if you experience prolonged general weakness without obvious reasons, contact a specialist. Some diseases are so dangerous if not diagnosed promptly that the risk of their presence justifies an unplanned trip to the doctor, who will reassure you if there is no cause for concern, or carry out the necessary diagnostics if suspicions arise.
Infusion of information and practical tips on clinical research
Most, but not all, publications have shown that the evidence and practical skills of surgeons have a significant impact on the risk of complications after endarterectomy of the carotid arteries. When examining the Canadian administrative data base, it was revealed that if an endarterectomy is performed on a patient by a surgeon who performs few such operations and performs in the hospital, who ends up receiving few such operations, then the risk is the decrease in internal hospital stroke and death increased by 3.5 times, equal with the surgeon, who receives a lot of such deliveries and works at the hospital, where a lot of such operations are carried out. These findings allow the framework to develop assumptions, which is the main connection between the surgeon’s knowledge and low sickness during the final operation, and therefore they must be interpreted carefully, so that the selection of patients can be applied to the results. Results at 30 days from the NASCET (the Asymptomatic Carotid Atherosclerosis Study) and other randomized clinical studies show a lower incidence of sagging at 30 days in asymptomatic younger patients, as and there are few comorbid conditions, equal with symptomatic older patients , like a bunch of comorbid conditions.
Diagnostics
Diagnosing a narrowed blood vessel may require one or more types of tests because the location of the narrowing is not always easy to find. For this purpose, our center uses:
- ultrasound - as the main method - since modern equipment provides maximum information not only about the presence of stenosis, but also the degree of deformation of the vessel, while being a non-invasive safe diagnostic method;
- MRI or CT;
- angiography - thanks to the introduction of a contrast agent, a complex diagnostic device monitors blood flow throughout the body, noting even minor deviations from the norm).
To diagnose atherosclerosis (which is the cause of narrowing), a laboratory method is also used - a blood test.
Diagnosis of important carotid artery stenosis
Traditional angiography is increasingly being used to identify carotid artery stenosis in patients with murmurs over the artery or symptomatic ischemic cerebrovascular disease, but it is not treated invasive methods, which include computer tomographic angiography, magnetic resonance angiography and duplex ultrasonography of the carotid arteries.
When performing angiography of the carotid arteries, physicians can use different techniques to assess the size of the artery diameter stenosis. Therefore, when interpreting a digital display, you need to know how it was indicated.
One-hundred-year-old duplex ultrasonography of the carotid arteries The Fellowship of Radiologists of Northern America proposes, in assessing the importance of carotid artery stenosis, to compare the criterion of peak systolic fluid (PSV) with hemorrhage through the internal the carotid artery is greater than 230 cm/s and the diameter of the artery lumen is approximately 50%. Secondary criteria for the importance of stenosis include a PSS of the internal carotid artery/hilar carotid artery greater than 4.0 and terminal diastolic fluidity (CDS) and bleeding through the internal carotid artery b more than 100 cm/s. Other authors found a 95% positive predictive value for arterial diameter stenosis of 60% or greater when combining the criteria of PSS over 290 cm/s and DFS over 80 cm/s.
When non-invasive investigations are conducted correctly, they produce more accurate results. A systematic review of 63 publications of MRA, carotid ultrasonography, and both methods is consistent with MRA having an overall sensitivity of 95% and an overall specificity of 90% for diagnosing stenosis of 70–99%, consistent with and stenosis less than 70%. For duplex ultrasonography of the carotid arteries, a sensitivity of 86% and a specificity of 87% were obtained. In both situations, angiography with digital processing of information was used as the gold standard. Magnetic resonance angiography has significant discriminatory power when diagnosing stenosis of 70–99%, while ultrasonography and MRA has significant advantages when diagnosing occlusion of the carotid artery.
Currently, the optimal methods for assessing carotid artery stenosis are Doppler ultrasonography and contrast-enhanced MRA.
Treatment of carotid artery stenosis
The most common treatment for stenosis is artery stenting. Stenting is a surgical treatment method, therefore, like any other surgical intervention, it requires a highly qualified doctor in diagnosis, deciding on the need/possibility of surgery and direct insertion of the stent. A stent is a metal frame inserted directly into an artery. At the point of narrowing, it unfolds and expands the walls of the vessel as necessary. The stent remains in the artery. Only in the first days its presence can be inconvenient due to changes in blood flow, but over time the patient stops feeling it and returns to normal life without the risk of a stroke. But of course, the doctor will give certain recommendations for further lifestyle in order to prevent re-stenosis.
Our doctors understand the importance of high-quality patient management and postoperative monitoring, so by contacting us, you can count on an integrated approach to diagnosis, treatment and the postoperative period. To implement this approach, the neurology department of the Federal Scientific Research Center has a powerful diagnostic base and a strong team of specialists with extensive experience in the treatment of stenosis, who additionally undergo advanced training courses on a regular basis. The department closely cooperates with the cardiac surgery service and the department of vascular surgery, which is separated into a separate unit.
The advantage of our center is the provision of a full range of services to our patients in one place, starting with an initial consultation, which you can sign up for by phone or through a special form on the website.
Angioplasty and stenting of the carotid arteries
Only a number of completed randomized studies have been published, which directly compared ESA with angioplasty and carotid artery stenting. Nowadays there will be much more evidence for the usefulness of stenting and against this method. The SAPPHIRE study center randomized 334 patients with asymptomatic carotid artery stenosis of either greater than 50% or greater than 80% to the ECA stenting procedure. The primary outcome measures were death, stroke or myocardial infarction within 30 days of the procedure and ipsilateral stroke and death between 31 days and 1 day after the procedure. The primary end point was recorded in 20 patients in the stenting group (cumulative incidence 12.2%) and 32 patients in the endarterectomy group (cumulative incidence 20.1%). There was no statistically significant difference between the two procedures (p = 0.053), but non-inferiority for stenting was equal to endarterectomy. It is important to note that a high incidence of perioperative complications was avoided both for endarterectomy and for stenting in this high-risk cohort. The incidence of stroke and death at 30 days for asymptomatic patients was 10.2% for endarterectomy and 5.4% for stenting (p = 0.20). These results provide information about the benefits that drug therapy may have in this group of patients.
The SPACE study was the first large randomized controlled study to compare endarterectomy versus stenting in symptomatic patients. The incidence of ipsilateral stroke and death at 30 days was similar—6.3% for endarterectomy and 6.8% for stenting.
The results of the EVA-3S follow-up on the 30th day have been published. This study included patients who had recently (within 120 days) hemispheric or retinal transient ischemic attack (TIA) or non-disabling stroke and minor stenosis of symptomatic carotid artery in 60 years. % to 99%. Patients were randomized to endarterectomy (n = 262) or stenting (n = 265). The incidence of stroke and death at 30 days was higher in the stenting group (9.6%) and lower in the endarterectomy group (3.9%). However, the investigation could have been compromised due to a lack of information about the various centers in which the stenting took place. In addition, in 8.1% of the cohort, the stenting procedure was completed without distal embolic closure. The terminal points were less likely to occur in patients in whom stenting was performed with an embolic stent, but equally so in those in whom stenting was performed without a stent.
In people with atherosclerotic lesions of the carotid arteries, a variety of embolic mechanisms have been tested. In typical cases, these structures contain 50 to 70% macroscopic embolic material. Microscopic material that leaks through these devices includes red blood cells, white blood cells, platelets, and fibrous hyperclinite tissue fragments. No clinical significance was identified for this material.
In the United States, we recommend clinical stenosis of the carotid arteries only in patients who have symptomatic carotid artery stenosis of 70% or greater, and only in cases where the clinical evidence does not provide adequate evidence for diagnosis and the sickness of this illness. Stents and embolic protection devices are thoroughly cut, therefore clinical investigations are necessary in order to carry out their straightening.