In most cases, the cause of deterioration in health is enlarged adenoids (nasopharyngeal tonsils), which consist of lymphatic tissue and help the immune system protect the child’s body from various types of infections. In inflammatory diseases, they swell and increase in size, which causes obvious physical discomfort and complicates the functioning of the respiratory system. Surgical removal of adenoids in children is carried out if conservative treatment does not produce the desired result or a severe stage of hypertrophy is diagnosed.
What are adenoids?
Strictly speaking, the adenoids are the pharyngeal tonsil, which, like other numerous lymphoid formations, is part of the so-called “lymphopharyngeal ring”.
It is located in the nasopharynx, every child and even an adult has it. However, in childhood, it takes a greater part in ensuring general and local immunity, and, apparently, this is why problems with adenoids arise most often between the ages of 2 and 10 years. After 13 years of age, their role in pathological processes decreases sharply, but before this age they manage to cause a lot of trouble for many children. The essence of these troubles is that the adenoids can increase in size and interfere with nasal breathing. Depending on the size, there are 3 degrees of hypertrophy (growth). First degree – the tissue size is minimal and there is no breathing disorder. This is considered normal and does not require any treatment. The second degree can be considered the norm only conditionally, if this does not lead to the appearance of complaints and symptoms. The third degree is an absolute pathology and requires mandatory measures aimed at restoring nasal breathing.
Enlarged adenoids
Adenoids of normal size
Functions of the adenoids
Adenoids are not some useless organ that can be removed without indication - at the request of the patient. They perform an important protective function in the body. Adenoids are part of the lymphatic pharyngeal ring, which belongs to the peripheral organs of the immune system.
Healthy tonsils perform a protective function. They, like a wall, do not allow infectious pathogens entering the nasopharynx into the respiratory tract. But with hypertrophy of the pharyngeal tonsils, they become a source of infection and cause exacerbation of respiratory tract diseases.
What does adenoid hypertrophy lead to?
During childhood, growth of the facial skeleton occurs. Long-term (more than 3 months) difficult nasal breathing not only greatly complicates life, but also leads to serious problems. The shape and structure of the face changes, it becomes elongated downwards, the lower jaw moves back, an incorrect bite is formed, the tongue is visible through the slightly open mouth, the child becomes unlike the parents. These changes, unfortunately, are irreversible. A nasal tone of voice appears, snoring during sleep, hearing loss, fatigue, weakness, frequent runny noses and colds. Changes in the composition of the blood, curvature of the spine, enuresis, nervous tics, impaired renal function and other problems may occur much less frequently. Moreover, usually these signs appear gradually, and parents do not notice them immediately, but only when they become pronounced.
Prevention of recurrence of adenoids
Adenoids often grow in children with chronic ENT diseases and acute respiratory infections. In childhood, the risk of adenoid vegetations appearing again after surgery is high. Any inflammatory processes in the nasal cavity and pharynx can provoke a relapse of the disease. The best way to prevent adenoids is timely treatment of acute respiratory infections, flu, sinusitis, laryngitis and other pathologies accompanied by swelling and inflammation of the mucous membrane.
Pediatric otolaryngologists at our Clinic have extensive practical experience. We use innovative technology to diagnose and treat pathologies of the nose and throat, including adenoids and their complications. You can always ask specialists the necessary questions and get professional advice from an ENT doctor.
Find out more about the treatment of adenoids from an ENT specialist at the Constanta Clinic in Yaroslavl by making an appointment (4852) 37-00-85 Daily from 8:00 to 20:00
Sign up for a consultation
When should you be wary?
You should be wary if your child:
- often or constantly with an open mouth;
- wheezes or snores in sleep;
- nasally and speaks unintelligibly;
- often suffers from acute respiratory infections, suffered from pharyngitis, bronchitis, tracheitis, inflammation of the middle ear (otitis media), sinusitis and other colds;
- asks again when he is addressed (sometimes parents perceive this as inattention, become irritated and are unaware of hearing loss);
- gets tired quickly, begins to lag behind peers in development and learning.
Any of these signs should be a reason to contact an ENT doctor.
Diagnosis of enlarged adenoids
Hypertrophied tissues of the nasopharyngeal tonsils cannot be seen with the naked eye, so special techniques are used to confirm the diagnosis:
- radiography;
- endoscopy of the nasopharynx;
- tympanometry – assessment of the condition of the eardrum and middle ear;
- examination by an ENT doctor using special instruments.
Particular attention is paid to children with frequent relapses of adenoiditis. Based on the clinical manifestations of the disease and data obtained during the examination, the doctor decides on the need for surgical intervention.
How is diagnosis carried out?
Enlarged adenoids. Endoscopic picture
To establish a diagnosis, a simple examination is sometimes sufficient, but often it is necessary to “see” the adenoids. It is best to look directly into the nasopharynx using an endoscope. However, this procedure is possible in children only from 5-7 years of age, when the child understands how to behave when there is an instrument deep in the nasal cavity. At an earlier age, endoscopy is also possible using 2-3 minutes of superficial inhalation anesthesia.
A more accessible method is x-ray examination. The advantage of this method is that everyone can view the image, including parents, and not just one doctor. Therefore, this method is considered the most objective. One of the X-ray diagnostic methods is computed tomography. But using it only to examine the nasopharynx is absolutely irrational and expensive. I would like to warn parents about a very ancient method of examining the nasopharynx, the so-called “finger”, which was used in the “pre-radiological” era and which doctors sometimes use now. It involves feeling the adenoids with a finger bent and placed behind the soft palate through the mouth. Look at the location of the nasopharynx in the diagram, and you can understand what the unfortunate child experiences. We consider this an inhumane, psychologically traumatic, highly subjective, archaic and unacceptable method. Don't let your children get hurt like that.
Indications for adenoid removal
- Frequent respiratory viral infections, bronchitis, tonsillitis. Adenoids disrupt the outflow of mucus and interfere with normal tissue respiration, which creates the preconditions for the development of infectious processes and frequent exacerbations of ENT diseases. Infection from adenoid vegetations easily spreads to neighboring tissues and spreads through the bloodstream to other organs.
- Decreased quality of nasal breathing. Breathing through the mouth becomes habitual for a child with adenoids. In the nasal cavity, the air is warmed and purified with the help of mucosal villi. When breathing is carried out mainly through the mouth, unwarmed air with bacteria and viruses immediately enters the respiratory tract and can cause infectious diseases. Nasal breathing is complete, but when a child breathes incorrectly, organs, mainly the brain, suffer from a lack of oxygen. It can even lead to developmental delays, apnea and chronic headaches.
- Chronic otitis media, hearing loss. With the growth of adenoid vegetations, the functions of the middle ear are disrupted, tissue nutrition deteriorates, and hearing may decrease. All these signs usually occur with severe hypertrophy of the pharyngeal tonsil and the ineffectiveness of conservative therapy; they require surgery and professional monitoring of the condition of the nasopharynx even after surgical treatment.
- Asymmetry of facial features, malocclusion. With the growth of adenoids, facial expression may change, and the bite is often disturbed. If you notice these changes, you should urgently contact an otolaryngologist and undergo surgical treatment.
On the issue of the dangers of X-ray irradiation.
It all depends on the dose. The natural background radiation on the surface of our planet is not dangerous to health. In the city this background is somewhat higher. The total average annual dose in Moscow is 3 mSv per year, the permissible dose is 15 mSv. A single irradiation, subject to accepted standards for any diagnostic studies, is absolutely safe. “Dose accumulation” during repeated irradiation is dangerous. And this needs to be monitored. That is why in our clinic you cannot do an X-ray examination at your own request. Technological progress makes it possible to reduce the required dose with each new generation of devices. With tomography, the radiation dose ranges from 1 to 7 mSv, and with radiography of the nasopharynx using modern equipment – 0.8-1 mSv. Thus, you gain several times more in the city.
Methods for diagnosing adenoids
Classic methods for diagnosing hypertrophy of the nasopharyngeal tonsil are digital examination of the nasopharynx and examination of the posterior parts of the nasal cavity. But these procedures are difficult and provide little information, especially in the case of children. The most modern diagnostic method is endoscopic examination - a method of examining the mucous membrane of the upper respiratory tract with an endoscope. The advantage of endoscopy is that it is painless and safe; the doctor gets a complete picture of the size of the nasopharynx, the degree of enlargement of the adenoid tissue and the condition of the mouths of the auditory tubes. Together, these data make it possible to determine a treatment method and diagnose the disease at an early stage.
How to treat adenoids?
There are two possible ways to treat adenoid hypertrophy: conservative and surgical. There are many conservative methods. They all have their advantages and disadvantages. We quite widely use homeopathy, laser magnetic therapy, and traditional methods of treatment. The main thing to be guided by when choosing a method is to understand the difference between cause and effect. There is a misconception that the cause of numerous complaints and problems is large adenoids. In fact, it's the other way around. The child is constantly sick not because he has large adenoids, but they are so large because he is sick all the time. Knowing the causes of inflammation, you can select the necessary therapy and in most cases achieve complete recovery and reduction of adenoids to normal.
Methods of conservative treatment of adenoids
The adenoid is an organ of the immune system. Its tissue contains cells that produce antibodies to pathogens. If conservative treatment is successful, this protective barrier is completely preserved. Antibacterial drugs are prescribed, since adenoiditis (inflammation of adenoid tissue) occurs primarily due to exposure to pathogenic microflora. To remove bacteria from the mucous membrane of the nose and nasopharynx, courses of nasal rinsing are carried out using a vacuum pump. Physiotherapy procedures, such as CUV tube, laser and magnetic devices, quickly relieve inflammation, improve blood circulation and local immunity. In the treatment of adenoids, not only an otolaryngologist, but also an allergist-immunologist is involved; he prescribes general tonic drugs that stimulate the body’s defenses in order to reduce the number of acute respiratory infections. But the effectiveness of conservative treatment methods is about 50% and there remains a risk of repeated exacerbations when faced with an infection, which means that symptoms may recur.
When is surgery needed?
Surgical removal should be performed only if there are clear indications, which depend, first of all, on the degree of enlargement of the adenoids. This is the main condition, but not the only one. Under certain conditions and with the second degree of hypertrophy, such indications may occur. The decision to operate must be made by an experienced surgeon, and the parents must give their consent if they do not doubt the doctor’s correctness. It is always possible to obtain the opinion of several specialists who may or may not advise surgical treatment. So if in doubt, don't waste your time. And remember, if there is no positive dynamics within 3 months of conservative treatment, you need to change either the treatment methods or the doctor.
Types of operations
Adenoidectomy in children is performed in several ways:
- By radio waves. Radio wave exposure allows excision of adenoids without loss of blood quickly and painlessly;
- Laser therapy. The most effective method of adenoidectomy, in which the scalpel is replaced with a laser beam;
- Endoscopy. The endoscope allows the surgeon to fully control the surgical process. The technique can be combined with laser therapy and tissue excision using radio waves;
- Cold plasma method. During the procedure, adenoids are destroyed and removed with cold plasma, which makes it possible to quickly and painlessly eliminate their growths.
When choosing a clinic for adenotomy, parents should pay attention to the technical equipment of the ENT office and consult with a specialist to determine the optimal tactics for the operation.
Why is anesthesia needed during surgery?
Adenotomy
- Cost: 50,000 - 80,000 rubles.
More details
The answer to this question is very simple - because in the 21st century it is unacceptable to do otherwise in a civilized country. Now an explanation for those who still think it can be done differently. Firstly, neither lubrication nor spraying of painkillers onto the nasal mucosa provides the main thing - complete anesthesia. During surgery under local anesthesia, the child is always in pain. Secondly, “being present” at one’s operation itself is unacceptable. People who have undergone such an adenotomy remember it all their lives. The sight of blood and pain in a child can cause nothing but horror. The psycho-emotional trauma in this case is so great that it can cause mental and neurological disorders. It would never occur to anyone to perform surgery on the abdominal organs without anesthesia. Thirdly, pain relief affects the quality of the operation. Modern methods of removing adenoids require that the patient does not interfere with the surgeon’s very delicate work. Fourth, all vital functions of the patient must be continuously and carefully monitored. If anyone thinks that there are no problems with local “pain relief,” then he is deeply mistaken. An anesthesiologist-resuscitator has great technical capabilities and experience in this field; he is best able to help the child. Only under such conditions can the surgeon be calm about the patient’s life, can perform the operation correctly, stop the bleeding, etc. This is very important, because unremoved pieces of adenoid tissue are the cause of relapses. Properly selected and correctly performed general anesthesia does not leave any consequences.
Features of transoral adenotomy (classical method)
Classic adenotomy can be performed under general or local anesthesia. The main surgical instrument is Beckmann's adenot - a curved knife designed to remove hypertrophied mucosa. The operation is performed sitting or lying down. 30 minutes before surgery, the mucous membranes are treated with a local anesthetic in the form of a spray or drops. The tissues lose sensitivity, but slight discomfort remains during the direct removal of adenoid vegetations.
The doctor directs the instrument to the roof of the nasopharynx and cuts off the adenoids, and then removes the removed tissue through the mouth. The procedure is almost instantaneous, and if the child relaxes and closes his eyes, he will not feel pain or fear.
Adenotomy under local anesthesia takes just a few minutes. If the child is psychologically prepared for the operation and its purpose is explained, the impact of stress on the psyche will be minimized.
How is adenoid removal done in children?
The technique for removing adenoid tissue (adenotomy) remained unchanged for a long time and consisted of scraping the nasopharynx with a special curette inserted through the mouth. It is clear that the quality of the operation with such a “blind, touch” method depends on many factors: on the child’s behavior, on the experience of the surgeon and his dexterity, on the particular location of the adenoids and the structure of the nasopharynx. The most common complications were bleeding with the need for prolonged tamponade, relapses due to unremoved tissue areas, and neurotic disorders due to psychological trauma. A very rare, but extremely dangerous complication was the entry of pieces of tissue into the lower respiratory tract during surgery. The emergence of special methods of general anesthesia in the second half of the last century made it possible to completely eliminate such a danger. And the use of special optics in the late 80s made it possible to perform this operation under vision control and classify it as “aesthetic surgery.” For visualization, various types of endoscopes, a surgical microscope, and mirror optics are used. Different surgical instruments can be used to directly remove tissue, depending on the specific situation. In certain situations, you can use a traditional adenotome, a microdebrider, special forceps, and even a plasma knife. The more different instruments a surgeon has, the more convenient it is to solve various problems, but the choice of instruments always remains his.
Complications
This operation is usually well tolerated with no adverse effects. However, removal of the pharyngeal tonsil can still cause the following complications:
- allergic reaction to the anesthetic used;
- bleeding requiring repeated intervention, the use of general and local hemostatic procedures;
- infection of a postoperative wound with the development of purulent foci in the lymph nodes, retropharyngeal space, mediastinum; in severe cases - sepsis;
- inhalation of removed tissues with the development of asphyxia (suffocation) or aspiration pneumonia;
- injury to the soft palate or root of the tongue, which leads to changes in voice, difficulty swallowing, and heavy bleeding.
To avoid such adverse effects, the operation should be done only in a well-equipped clinic by an experienced surgeon.
How is adenotomy performed in our clinic?
- Only under general anesthesia. In our clinic we have been performing this operation for over 20 years. During this time, more than 6 thousand operations were performed.
- Only under visual control. We have been using endoscopic technology since 2001.
- The day surgical hospital, which is part of the multidisciplinary private clinic CELT, allows us to use all its capabilities. The organization of our work involves staying in the clinic during the day, but if necessary, the stay can be extended.
- The child is in the clinic with his parents.
Postoperative period
Adenotomy, performed under general anesthesia, ends with the child being transferred to the ward with his parents, where his condition is monitored by qualified specialists (attending physician, anesthesiologist and medical staff). In our Clinic it is possible to accommodate a parent and child in separate beds. For children from 2 to 10 years old, a special comfortable bed with a small side can be provided so that the child can feel at home. Add a photo from the attachment here.
After discharge, the little patient and his parents can go home. Specialists will tell you in detail about the rules of behavior in the postoperative period. During the first days, it is recommended to eat only soft foods that do not require long chewing. Following a diet will speed up your child’s recovery. The mode of physical activity in the first weeks after surgery should also be gentle. Warming procedures are prohibited, sunbathing and visiting the bathhouse are prohibited. Replace bathing with showering. Protect your child from active games, accidental injuries and falls. It is not necessary to force him to lie down and do nothing - he can calmly play, go for walks, and communicate with friends. Make sure that the baby does not touch his nose or try to get into the nasopharynx.
Usually, no additional medications are prescribed during the rehabilitation period, except for antipyretics, which are necessary to relieve pain and fever. The tissues gradually regenerate, after how many days the wound is covered with plaque, which is rejected without pain.
If a child feels pain and it bothers him greatly, it is recommended to consult a specialist, and any children’s medications prescribed by the doctor can be used as an anesthetic to relieve pain and reduce body temperature.
What happens on the day of surgery?
On the appointed day, you come to the day hospital at the agreed time. On the day of the operation, we strongly recommend giving a light breakfast at home in liquid form in a volume of 100-150 ml (yogurt, kefir, milk, very thin porridge or at least sweet tea). The surgeon examines the patient, checks tests, talks with the parents and decides on the possibility of performing the operation. The patient is asked to drink a soothing mixture and wait 20-30 minutes. Then he is invited to the operating room, where, while lying on the operating table, a breathing mask is applied to his face, and after 10-15 seconds the child falls asleep. All operations are carried out with mandatory monitoring of respiratory and cardiac activity. After the patient has fallen asleep, a catheter is inserted into the vein to administer the necessary medications. Removal of adenoids is carried out under visual control using special optics and an endoscope. The awakening occurs in the ward, where the little patient immediately sees his parents. After the operation, we monitor the child for 4-5 hours. If his condition does not cause concern, then the doctor will let you go home. The postoperative period lasts 7-10 days and requires special care for the patient at home. Upon discharge, you receive detailed instructions and the surgeon's mobile phone number, where you can contact the doctor 24 hours a day.
Contraindications
In addition to age restrictions, there are a number of other contraindications for adenoid removal:
- malignant neoplasms of any location;
- exacerbation of other chronic diseases;
- infections of any etiology – influenza, chickenpox and others;
- decreased blood clotting rates;
- some anatomical features of the structure of blood vessels in the nasopharynx;
- recently received vaccinations.
The decision on when to perform an adenoidectomy is made by the doctor, taking into account all possible risks and the likelihood of complications.
What is needed for elective surgery?
To remove adenoids or tonsils, the following conditions are necessary:
- consultation with an otolaryngologist who will perform the operation;
- do not get sick for a month;
- Avoid childhood infections for three months (measles, chicken pox, scarlet fever, rubella, mumps, whooping cough).
Documents required for hospitalization:
- general (clinical) blood test;
- blood test for HIV, RW, HBsAg, HCV;
- blood test for group, Rh factor and antibodies to Rh factor with phenotyping;
- general (clinical) urine analysis;
- certificate from the dentist about oral sanitation;
- conclusion of a pediatrician (and other specialists in the presence of diseases) about the absence of contraindications to surgery.
coagulogram (prothrombin time, aPTT, thrombin time, fibrinogen, antithrombin III) or hemosyndrome (platelets, blood clotting time, bleeding time);
All necessary tests can be performed in our clinic.
Contraindications to adenotomy
The operation is not performed on children under 2 years of age, except in emergency situations. General contraindications to adenotomy are:
- ARVI, influenza and other acute infections;
- exacerbation of allergies;
- blood clotting disorder;
- cleft lip and palate;
- malignant tumors of any location;
- intolerance to drugs for pain relief or anesthesia;
- concomitant pathologies (heart malformations) in specialized centers;
- anomalies of nasopharyngeal vessels.
A temporary ban may be the recent performance of other surgical interventions. Preventive vaccinations are also a reason to postpone surgery. It is recommended to wait at least 1-2 months after vaccination.
What if the tonsils are still enlarged?
Sometimes, along with the adenoids, the palatine tonsils, which are popularly called “tonsils,” grow. They are clearly visible when examining the pharynx. Unfortunately, in this situation there may be indications for additional surgical intervention. If both the tonsils and adenoids are enlarged, it is advisable to solve both of these problems at the same time, i.e. during one operation, remove the adenoids and partially remove the tonsils (to a physiologically normal size). In our clinic, this operation is performed using a bloodless technique, using radiosurgical instruments.
Degrees of enlargement of adenoids
Current classification according to the degree of enlargement of the adenoids (and it determines the indications for medical or surgical treatment):
Classification of adenoids according to the degree of enlargement
| I degree | II degree | III degree | |
| Adenoid size | The adenoids cover the upper third of the vomer*. | The adenoids are medium in size, covering two-thirds of the vomer. | The adenoids are large, cover the entire or almost the entire vomer, and completely cover the lumen of the nasopharynx. |
| Difficulty breathing | In this case, breathing through the nose may be free or slightly difficult, more often during sleep. | Breathing through the nose is quite difficult. | Breathing through the nose is severely difficult, the child constantly breathes through his mouth, his lips are dry, covered with cracks and crusts. |
| Method of treatment | A course of conservative treatment is indicated. We talk about adenotomy if the child is often sick, complications occur, for example, recurring otitis media. | Both conservative and surgical treatment are possible. Indications for surgery are determined individually, the main criterion being complications and the incidence of illness in the child. If the child does not receive any treatment at all, the adenoid may enlarge. | The adenoid must be removed. If the child is not operated on in time, an abnormal bite and an elongated “adenoid face” will gradually form, which is subsequently difficult to correct. Even long-term treatment by an orthodontist does not always completely restore the correct facial skeleton. |
| *The vomer is a small plate made from bone and placed vertically. Together with the ethmoid bone, it forms the bony septum of the nose. | |||
What kind of rehabilitation is needed after surgery?
After surgery, the child needs special care. He should not be allowed out of the house and left alone.
Mode. On the first day - strict bed rest, and in the next 7-10 days - at home. For at least 2 weeks, it is necessary to exclude any physical activity, etc. For a week, the child should not take a hot bath or undergo any thermal procedures (inhalations, compresses, warming).
Diet. Feed the child regular, non-rough food, excluding hot, very cold, spicy, salty, and sour foods. The duration of such a diet is from 3 to 10 days, depending on the doctor’s instructions.
Local anesthesia or general anesthesia?
Removal of adenoids is carried out mainly at the age of 3-10 years, when the child, due to psychological characteristics, cannot calmly accept the operation under local anesthesia. Children are afraid of blood and the painful sensations that are still present when removing adenoids in the classical way will cause physical discomfort and act as a stress factor.
When choosing an anesthesia method, the doctor takes into account the following factors:
- age and psychological characteristics of a particular child;
- direction of growth and number of adenoids;
- general health;
- degree of nasal breathing impairment.
General anesthesia ensures complete absence of sensitivity throughout the entire period of surgery and for some time after it. The child does not see what the doctor is doing and does not feel fear. Local anesthesia will dull sensation, but some pain will remain. As you know, children do not tolerate pain well, and fear increases sensations and anxiety. Therefore, general anesthesia is preferable for children under 8 years of age. Local anesthesia is possible at an older age, when the process and significance of the procedure can be explained to the child, and he can sit quietly for 10-20 minutes without making sudden movements.
Treatment results
Nasal breathing improves, as a rule, immediately after surgery, hearing is often immediately restored, and the mouth closes. With very large adenoids, after surgery the child may develop a nasal tone, which quickly disappears. The final effect of the operation can be assessed after a month. After it becomes easier for the child to breathe, and therefore to live, snoring, oxygen starvation and endless colds will disappear, appetite and mood will improve, and a feeling of joy and endless energy will appear.
Where to go?
If a child shows signs of adenoids, consultation and treatment with an ENT doctor is necessary. If necessary, surgical intervention is prescribed. Our clinic invites residents of Moscow and the regions to contact the paid services department for treatment. The price for adenoid removal is 16,000 rubles, excluding anesthesia and the cost of hospital stay.
In our clinic, in addition to the traditional one, laser adenotomy is performed using a holmium laser (Ho:YAG) with a radiation power of 4.8 W (energy - 0.6 J, frequency - 8.0 Hz). This modern technique is accompanied by a low risk of complications, absence of bleeding and pain.
You should not postpone the removal of adenoids, since in the future the disease will lead to slower growth and mental development, deformation of facial features and other irreversible changes. After surgery, most children experience better colds, less frequent otitis media, and normal breathing through the nose.
How much does it cost to remove adenoids in children at CELT?
The cost of an operation to remove adenoids in a child at the CELT clinic costs from 45,000 to 75,000 rubles, depending on the category of complexity. It is important for the patient’s parents to know that in the price list we always show the full financial costs, and not just the cost of the surgical intervention itself.
Make your main choice! If after removal of the adenoids there is no recovery, the child breathes poorly through the nose, and continues to get sick, it means that the cause of the inflammation remains. To prevent this from happening, the most important thing is to find an experienced doctor and a good clinic for your child. We hope this article will help you avoid mistakes. About all the advantages of adenoid removal at the Center for Endosurgery and Lithotripsy, read “Endoscopic removal of adenoids. Why choose us?
Endoscopic adenotomy
Endoscopic adenotomy is currently the best method of surgical treatment of adenoids. The operation is performed under general anesthesia and lasts 10-20 minutes. Thanks to the high technical characteristics and wide capabilities of endoscopic equipment, the surgeon removes hypertrophied adenoids with precision without damaging healthy tissue. Due to minimal trauma, there is no long rehabilitation period.
Endoscopic operations are easily tolerated by children. Adenoid vegetations may reappear and must be removed again. In this case, the endoscopic method of excision of adenoids is most preferable. It is indispensable for the growth of adenoid vegetations along the mucosa, when pathological growths are an obstacle to the passage of air along the auditory tube and can provoke hearing loss.
How is endoscopic adenoid removal performed?
After using an anesthetic drug, the doctor inserts an endoscope into the nasal cavity. At the end of the instrument there is a video camera that provides high-quality visualization and allows you to carefully examine the surgical field. Severing the hypertrophied pharyngeal tonsil can be carried out using various endoscopic instruments (resection loop, electric knife) - depending on the equipment of the installation used. In some cases, the doctor will excise the abnormal tissue through the mouth.
One of the types of endoscopic adenotomy is the removal of adenoids using a shaver, which is a micro-mill placed in a tube. There is a hole on the side of the tube, through which the instrument grasps and excises hypertrophied tissue. They are aspirated from the nasal cavity, which eliminates the risk of adenoid fragments entering the respiratory tract and causing aspiration.
In our Clinic, endoscopic adenotomy is performed under general anesthesia. But when using an endoscope equipped with a video camera and micro-instruments, tissue trauma is minimal. The effect of anesthesia on the child does not last long, since the operation itself lasts only 10-20 minutes.
Not all medical institutions have ample opportunities to use modern endoscopy in the treatment of adenoids. The CONSTANTA clinic employs experienced otolaryngologists and surgeons who are fluent in the technique of endoscopic removal of hypertrophied pharyngeal tonsils. The pediatric anesthesiologist calculates the dose of anesthesia and is constantly present during the operation, monitoring the child’s condition and the functioning of all body systems. The high professionalism of the Clinic’s team of specialists allows us to minimize any risks and remove pathological tissue as efficiently as possible.
Recommendations for maintaining health after adenoid removal
After surgery, restorative and restorative therapy is necessary to prevent relapse. General hardening of the body, breathing exercises, as well as treatment and observation by an allergist-immunologist, especially when it comes to children with concomitant diseases such as atopic dermatitis, bronchial asthma, allergic rhinitis. Normalizing the functioning of the immune system is very important - by increasing resistance to infections and colds, the likelihood of lymphoid tissue proliferation decreases.
Reasons for the formation of adenoids in childhood:
- hereditary immune pathology, which often occurs in parallel with reduced thyroid function;
- birth injury;
- difficult pregnancy (the most dangerous factor is viral diseases suffered by the expectant mother in the first trimester);
- mother taking toxic drugs and antibiotics during pregnancy;
- asphyxia or hypoxia during childbirth;
- immunodeficiency caused by poor living conditions, dangerous environmental conditions;
- childhood infections (measles, diphtheria, scarlet fever, etc.);
- low-quality food containing many chemical additives;
- frequent viral diseases of the child;
- allergy.
Under the influence of these factors, pathological hyperplasia of the adenoids occurs, which negatively affects the condition of both the nasopharynx, paranasal sinuses, and the middle ear cavity. The pharyngeal tonsil acquires the role of a kind of collector of pathogens; adenoid tissue may contain hemolytic streptococci, staphylococci, Haemophilus influenzae, Moraxella, and pneumococci. It is these microorganisms that most often cause severe respiratory diseases, including pneumonia and otitis media. Source: Orlova E.S. Adenoids in children / E.S. Orlova // Pediatric practice. - 2015. - No. 3. - P. 53-56. .
Zaichenko Vladislav Sergeevich
Otorhinolaryngologist, Head of the Department of Otolaryngology
Doctor of the highest qualification category
“Signs of enlarged adenoids in adults: sleep apnea and snoring, nasal congestion, mucus running down the back of the throat, stuffy ears, frequent runny nose, nasal voice, headaches, frequent sinusitis. Adenoid vegetations can be detected at any age.”
Postoperative rehabilitation
Patients may experience pain in the throat and difficulty breathing through the nose. Our specialist will prescribe pain medications and give recommendations on how to improve your well-being.
The temperature may rise on the first day. It is better for the child to lie down more for three days. For three to ten days, you must follow a diet based on food that does not irritate the tissue in the intervention area.
After a week, crusts and clots are removed from the nose, and breathing is restored. For children under 8 years of age, this procedure is performed in a state of “medicated sleep.”
Surgical treatment of hypertrophy of tonsils and adenoids
In the Republic of Belarus, the concept of informed voluntary consent to medical intervention is reflected in Articles 27, 28, 29 and 30 of the Law on Health Care, which lists the general rights of the patient, in particular: the right to choose a doctor, informed voluntary consent, refusal of medical intervention, the right to information about your health and all aspects of medical interventions proposed or carried out.
From the point of view of medical law, informed consent to medical intervention should be understood as the patient’s voluntary, competent acceptance of the proposed treatment option. This decision should be based on receiving complete, objective and comprehensive information about the upcoming treatment, its possible complications and alternative treatment methods.
In accordance with the above provisions, we invite you to familiarize yourself with the principles and methods of surgical treatment of hypertrophy of the tonsils and adenoids. The written information provided to you serves this purpose. Read it carefully to discuss any unclear points with your doctor.
General concepts about tonsillitis, tonsil hypertrophy and adenoids.
Every healthy child has lymphoid tissue in the pharynx, which is united into the so-called lymphadenoid pharyngeal ring. It includes the palatine tonsils - “tonsils” - they can be seen when examining the mouth - they look like balls protruding on the sides of the tongue, the pharyngeal tonsil - it cannot be seen during a direct examination of the oral cavity, it hides in the nasopharynx, behind the palate, lingual tonsil - located at the root of the tongue, and many lymphoid follicles scattered along the back wall of the pharynx, at the entrance to the larynx. These formations help the child defeat pathogenic bacteria that enter the throat during breathing and eating, and contribute to the formation of local immunity - protection against pathogens. By the way, in these organs there are no cells that affect the sexual development of the child, they do not produce sex hormones, therefore their diseases do not affect the sexual development of the child, and if they are removed if necessary (more on this later), sexual development is not disrupted.
Location of adenoid vegetations in the nasopharynx (adenoid vegetations are highlighted in red)
In early childhood - usually from 2 to 5-7 years - the described organs work very hard, as the child expands the scope of contacts with peers by attending kindergarten, and inevitably often becomes infected and develops respiratory diseases. Moreover, if the child’s immune forces are not strong enough due to congenital characteristics, environmental factors and other reasons, the lymphoid organs increase in volume. This enlargement of the palatine tonsils is called “hypertrophy of the palatine tonsils”; they can become inflamed - inflammation of the tonsils is called tonsillitis. An enlarged, chronically inflamed pharyngeal tonsil is called “adenoids.”
Adenoids have a significant impact on health and the development of nearby organs. What kind of influence is this? A chronic inflammatory process, constantly smoldering in the adenoid tissue, periodically exacerbating, contributes to protracted, recurrent diseases of the trachea and bronchi (bronchitis, obstructive bronchitis, tracheitis, pharyngitis), can independently cause or aggravate the course of allergies, in severe cases manifested in the form of bronchial asthma, allergic rhinopathy, atopic dermatitis.
Adenoids, filling the nasopharynx, cause difficulty in nasal breathing, impair the functioning of the auditory tubes, which cannot sufficiently deliver air to the middle ear, as a result of which secretory otitis media develops, which can lead to hearing loss, and if an infection enters the ear, to acute hearing loss. inflammation – acute purulent otitis media. A noticeable obstacle to the passage of an air stream through the nose leads to breathing through the mouth, and, consequently, to the fact that the nose cannot perform its functions, which, in turn, are very important. The consequence is obvious - untreated air enters the respiratory tract - not purified, not warmed and not humidified. And this greatly increases the likelihood of inflammatory processes in the pharynx, larynx, trachea, bronchi, and lungs (tonsillitis, laryngitis, tracheitis, bronchitis, pneumonia).
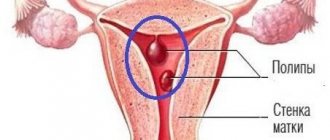
Poor breathing through the nose contributes to improper development of the maxillofacial area - the bite of the teeth is disrupted, the shape of the face changes (the so-called “adenoid face”), the paranasal sinuses develop poorly, which in primary school age leads to sinusitis - sinusitis (sinusitis, sinusitis). , ethmoiditis), and later – to chronic sinusitis, the growth of polyps in the sinuses and nasal cavity.
What factors contribute to the appearance of adenoids?
- Heredity - at least if the parents suffered from adenoids, the child, to one degree or another, will also encounter this problem.
- Inflammatory diseases of the nose, throat, pharynx - and respiratory viral infections, and measles, and whooping cough, and scarlet fever, and tonsillitis, etc.
- Eating disorders - especially overfeeding.
- Tendency to allergic reactions, congenital and acquired immunity deficiency.
- Violations of the optimal properties of the air that the child breathes - very warm, very dry, a lot of dust, an admixture of harmful substances (ecological conditions, excess household chemicals).
Thus, the actions of parents aimed at preventing adenoids come down to correction, and even better, to the initial organization of a lifestyle that promotes the normal functioning of the immune system - feeding according to appetite, physical activity, hardening, limiting contact with dust and household chemicals.
If the child, along with the adenoids, has enlarged tonsils
At the age of 8-9 years, when a child has enlargement (hypertrophy) of the palatine tonsils, but has not yet developed chronic tonsillitis (the child does not suffer from sore throats, purulent plugs do not accumulate in the lacunae), it is possible to reduce them using minimal surgical intervention on the tonsils volume and stop the pathological process. In this case, otolaryngologists suggest that when removing the adenoids, the palatine tonsils are also reduced in volume (“cut”) - this operation is called tonsillotomy. If this is not done, the child has a high probability of even greater enlargement of the palatine tonsils (so-called compensatory hypertrophy), which will negate the results of adenotomy - again the child will begin to breathe poorly through the nose, get sick often, snoring will not go away or will get worse. In addition, against the background of hypertrophy, a chronic inflammatory process often develops in the palatine tonsils, which subsequently requires their complete removal.
Tonsillitis can be acute or chronic. Acute tonsillitis - tonsillitis - is an infectious disease that requires conservative (drug) treatment at home or in an infectious diseases hospital under the supervision of a pediatrician. The causative agents of infectious diseases of the respiratory tract (most often streptococci) after a sore throat remain in the palatine tonsils, and their chronic inflammation develops - chronic tonsillitis. Under unfavorable circumstances (hypothermia, stress, viral infection), the process in the tonsils is activated. This occurs in the form of another sore throat with plaque on the tonsils or purulent plugs. What is very dangerous is that each exacerbation of tonsillitis can cause complications in the form of diseases of other organs and systems of the child’s body, most often rheumatic diseases of the heart and joints, kidney diseases (pyelitis, pyelonephritis, glomerulonephritis). In addition, exacerbation of tonsillitis or tonsillitis sometimes causes complications in the form of an abscess (ulcer) in the pharynx. This complication is called peritonsillar abscess.
In chronic tonsillitis, the course of the disease can go so far that the tonsils cease to perform their protective function; this form of tonsillitis is called “decompensated” and cannot be cured with medications; it requires surgical treatment - removal of the tonsils. The operation to remove the tonsils is called a tonsillectomy.
When should you consult an ENT doctor so that it is not too late?
If your child begins to get a “runny nose” frequently and it lasts longer than 10-12 days, the child, even in a state of relative health, begins to breathe worse through his nose, snores during sleep, and begins to be unable to hear (the child becomes inattentive, asks questions again, asks to increase the volume when watching TV programs ), you should visit an otolaryngologist to assess the condition of the pharynx, determine the presence of adenoids and the degree of their enlargement.
How does a doctor determine whether a child has adenoids and what size they are?
This is done using a small round mirror inserted behind the soft palate (this is difficult to do in young children), or by digital examination of the nasopharynx: the doctor feels the nasopharynx with his finger for 1-2 seconds. This is the most reliable, reliable and safe method for diagnosing adenoids. An X-ray examination is also used - a lateral radiograph of the nasopharynx using a contrast agent that is instilled into the nose, an endoscopic examination - examination of the posterior parts of the nose and nasopharynx with rigid or flexible endoscopes after anesthesia of the mucous membrane - a painful procedure for young children and therefore used in cases that are difficult to diagnose cases (for example, with congenital underdevelopment of the nasal passages, suspected tumor, etc.).
The size of the adenoids is assessed in degrees - there are three of them: the first - when the adenoids occupy a third of the volume of the nasopharynx, the second - two-thirds, and the third - when the adenoids fill the entire nasopharynx.
The grade is determined to evaluate changes in the adenoids during treatment, and not to decide whether to remove them or not. Indications for adenoid removal are determined by other criteria. More on this later.
Is it possible and necessary to “treat adenoids”?
We emphasize that it is not only possible, but also necessary to treat, but not the adenoids, but the chronic inflammatory process in them, called adenoiditis. Until the child develops the changes mentioned earlier, both local treatment should be used in the form of drops, irrigation of the nasal mucosa and nasopharynx with aqueous solutions that have anti-inflammatory, antiallergic and antimicrobial properties, as well as general treatment methods, including vitamin preparations, agents, those affecting the immune system, locally acting vaccine preparations, physiotherapeutic methods (magnetic and laser therapy, inhalation methods of drug administration have proven themselves well). Homeopathic methods of treatment are not contraindicated. However, when, during observation of a child, changes appear in the ears (recurrent otitis, dysfunction of the auditory tubes, exudative otitis), paranasal sinuses (recurrent sinusitis, chronic sinusitis), there are chronic or recurrent bronchopulmonary diseases, allergies, adenoids, regardless of the degree of their increase are subject to mandatory removal.
How urgently should the operation be performed?
Operations to remove adenoids and tonsils - adenotomy, tonsillotomy, tonsillectomy - are planned, that is, they are performed when the child is in full health or in remission of chronic diseases. It cannot be performed during acute illnesses (ARI) and 3-4 weeks after recovery. Thus, it is always possible to perform this operation in a period favorable for the child, which will minimize the risk of postoperative complications.
Is it possible to delay or not do the operation at all, because, they say, the adenoids are resolving, maybe they will “outgrow”?
Indeed, adenoid tissue atrophies over time, however, this process begins in adolescence and ends at 18-20 years of age. This process is long, and by the time it is completed, as a rule, a number of irreversible diseases requiring surgical treatment have formed (chronic otitis media, sinusitis, tonsillitis). Thus, it is obvious that it is more expedient to perform a minor operation in early childhood and improve the child’s health than to condemn him to long-term treatment, which often does not lead to full health, at an older age.
Do adenoids grow back, are relapses common?
Yes, adenoids can recur.
We draw attention to the fact that, regardless of the qualifications of the surgeon, it is impossible to completely remove the pharyngeal tonsil - at least something will remain. And there is always a possibility that adenoids will appear (grow) again. This happens quite rarely - in 4-5% of cases. However, relapse does not mean repeated surgical treatment. As a rule, adenoid tissue can reappear in the nasopharynx no earlier than after 7-12 months, during which time the function of the auditory tubes and nose usually has time to recover, the volume of the nasopharynx increases as the child grows, and the newly enlarged adenoids no longer have such a detrimental effect, as before the operation. Typically, conservative treatment methods can solve the problem. Repeated adenoid removal is required in 1-2 patients out of a thousand operated on.
The reappearance of adenoids is a reason for serious parental consideration. And it’s not at all about the fact that a bad doctor was “caught”. And the fact that all doctors taken together will not help if the child is surrounded by dust, dry and warm air, if the child is fed with persuasion, if TV is more important than walks, if there is no physical activity, if... If it is easier for mom and dad to take the child to otolaryngologist, than to part with your favorite carpet, organize hardening, sports, sufficient time in the fresh air.
Removed tonsils cannot grow back. Tonsillectomy allows you to radically and permanently solve the tonsillar problem.
How are adenoids removed?
This operation is performed in children under 8 years of age without local anesthesia; for children over 8 years of age, anesthesia is used by lubricating or irrigating the nasopharyngeal mucosa with a lidocaine solution. In young children this is prohibited due to the possibility of asphyxia (suffocation) developing in the child. This operation is unpleasant, but not painful; the sensations experienced by the child are comparable to lubricating the throat. It lasts a short time (5-6 seconds) and, with proper psychological preparation of the child, is tolerated satisfactorily. Under special circumstances - the presence of concomitant diseases in which local anesthesia is undesirable, the child’s pronounced negativism towards medical manipulations, emotional lability and psychological unpreparedness of the child and parents for surgery without anesthesia - adenotomy and tonsillotomy are performed under general anesthesia, which involves a more in-depth examination of the child.
The simplicity of the operation does not indicate the safety of the operation. Complications due to anesthesia, bleeding, and damage to the palate are also possible. But all this does not happen often. You can find a list of possible complications below.
Surgeons have long abandoned the removal of adenoids using ultrasound and laser due to the huge risk of complications.
How long does a child stay in the hospital after adenotomy and tonsillotomy?
Due to the high risk of bleeding in the postoperative period, we recommend staying in the hospital for 24 hours after surgery to remove adenoids. Usually the child is discharged home the next day. After tonsillotomy, the child is observed in the hospital for a day longer.
What should you do after your baby is discharged?
The child is discharged from the hospital under the supervision of an ENT doctor or pediatrician at the clinic at the place of residence. Home treatment is usually recommended for 3-5 days.
In this case, physical activity should be limited, however, there is no need to keep the child in bed. When eating during the first days, you should not eat hot, spicy foods, sour juices and fruits, carbonated drinks, or ice cream. After 3-5 days, the diet becomes normal. 3-5 days after discharge, if the child’s general condition is satisfactory, there is no elevated body temperature, and the wound in the pharynx is healing smoothly, you can visit the children’s group and go outside. You can’t just do sports or go to the pool. The wound in the nasopharynx heals completely in 2-3 weeks. A month after the operation, there are no restrictions in lifestyle or diet.
How to remove adenoids at the Children's City ENT Center?
To establish a diagnosis, if there is no ENT doctor in the clinic, you can make an appointment at the city ENT consultation office by calling 2-78-49-00 (inquiry). Consultative reception is carried out on weekdays, from 8.00. until 20.00.
If the diagnosis of “hypertrophy of the palatine tonsils, adenoids” has been established and the decision to operate on the child has been made, with a referral for surgical treatment issued at the clinic, you should go to the emergency department of the 3rd Children's Clinical Hospital at any time convenient for you. Your child will be registered for hospitalization on the day you choose and will be given an examination plan (a list of tests necessary to perform the operation). Hospitalization is carried out on Tuesday and Thursday, from 13.00. until 15.00. and on Sunday from 16.00. until 18.00. During hospitalization, the child is examined by an ENT doctor, who evaluates the examination performed in the clinic in accordance with the scope of surgical treatment and the method of anesthesia and, in the absence of contraindications to the operation, admits the child to the hospital. The operation is carried out the next day. Mothers with children under 5 years of age are hospitalized and issued a certificate of incapacity for work.