Myocardial infarction is always a great risk to a person’s life. The cause of almost every third death in our country is cardiac arrest due to insufficient blood supply (ischemia) to the heart muscle (myocardium), as a result of which the organ tissue begins to die. Up to 40% of people with this diagnosis die in the first 15-20 minutes after the onset of the disease. That is why it is so important for patients with pathologies of the cardiovascular system to undergo examinations, to know the first signs of the development of myocardial infarction in women and men, and to always be ready to call an ambulance. Your health and life, as well as the lives of your loved ones, next to whom you find yourself at the right moment, may depend on the ability to correctly identify the symptoms of the disease, competent and prompt actions.
Myocardial infarction: symptoms, signs of the need for first aid
Myocardial infarction in medicine is defined as the development of necrotic changes in the heart.
This is one of the most acute clinical forms of IHD (coronary heart disease). The disorder occurs due to acute insufficiency of blood flow due to a failure in the supply of oxygen to the heart muscle. A heart attack may be indicated by sudden sweating, nausea, pain in the sternum, forearm and other parts of the body. Heart attacks in men occur 5 times more often than in women, which is especially noticeable in young and middle-aged people. Heart attacks in women develop on average 10-12 years later than in men. Among the reasons is the later development of atherosclerotic changes, which is facilitated by less widespread bad habits and the protective effect of estrogens in women.
Causes of pre-infarction condition
The condition of pre-infarction is caused by a cessation of nutrition to the heart muscle due to blockage or spasm of blood vessels. Older women are most often affected by the following factors:
- hypertonic disease;
- IHD;
- diabetes;
- atherosclerosis;
- nervous fatigue;
- frequent stress;
- excessive physical activity;
- body hypothermia;
- bad habits: smoking, alcohol;
- excess weight.
The pre-infarction state can last for days or even weeks. It manifests itself in the form of squeezing pain or burning. Urgent measures are needed to normalize blood circulation in order to prevent the onset of the next phase of the disease - a heart attack.
Causes of myocardial infarction
Myocardial infarction develops for various reasons, some of which are contributed by the person himself, others by his environment. Let us highlight 3 main groups of provoking factors:
- Factors that directly depend on the person - eating large amounts of fatty foods, smoking, excessive alcohol consumption.
- Factors that indirectly depend on a person are obesity, menopause and postmenopause.
- Factors that do not depend on a person - old age, genetic predisposition.
Myocardial infarction develops with atherosclerosis and inflammation in the walls of the arteries resulting from trauma, radiation exposure, vascular embolism, congenital anomalies and disruptions of the hematopoietic apparatus.
Risk group
Character traits inherent in women such as caring for the family, worries about the fate of children, dedication and self-sacrifice contribute to their being at risk. Such women practically forget about themselves, do not care about their own health, ignore or simply forget about visiting a doctor for preventive purposes. Without paying due attention to the warning signs of the disease, they may end up in a situation where irreversible processes occur.
Women who live a lifestyle that is far from healthy are also at risk of having a heart attack. Those who engage in heavy (harmful) physical labor or suffer from chronic diseases are also not insured.
It is very important for women over 50 to see a cardiologist regularly.
Statistics show that the rate of cardiovascular disease is so high that women aged 30 or 40 may also be at risk. Therefore, preventive methods should be applied starting at an earlier age.
Heart attack: symptoms and first signs
- Patients do not always associate symptoms of a heart attack with the manifestation of this pathology. The patient’s feelings depend on what period of its development the disease is at. Common signs of a heart attack:
- severe dizziness, feeling of lack of air, shortness of breath;
- feeling of chronic fatigue, cold sweat on the body;
- uneven heartbeat, severe arrhythmia;
- pain impulses in the arms, forearms, shoulders, side, sternum;
- nausea, unpleasant heaviness in the stomach, loss of consciousness.
The first signs of a heart attack are not always obvious, but they attract attention. There are several periods of development of pathology:
- Pre-infarction stage - the first signs here are increased fatigue, weakness, fatigue, a feeling of squeezing and rapid heartbeat. There is no significant pain yet. In a patient with myocardial infarction, the lips and nail plates turn blue, the pulse becomes erratic and uneven. At this time, the severity of the disease increases, the duration of the period ranges from a couple of hours to a month.
- The most acute stage of heart attacks is pain. The patient begins to feel as if his chest is being squeezed in a vice. Behind the sternum there is a burning sensation, fiery heat, pulsating pain. With the development of an extensive heart attack, the pain is severe and prolonged. Strong and abrupt impulses are observed in young patients. Muffled pain, indicating myocardial infarction, is more often observed in patients with diabetes mellitus. The duration of the period is from half an hour to 2-4 hours. Complications that pose a direct threat to life are possible.
- Acute stage of a heart attack - among the first symptoms, the final formation of a focus of dead tissue and the occurrence of life-threatening conditions are noted. The duration of the period is 2-14 days.
- Subacute period - dead areas are replaced by connective tissue. The duration of the stage is 6-8 weeks.
- The post-infarction period lasts from two months to six months. During this time, the body adapts to new conditions.
If there are signs of a heart attack, you should not self-medicate; you should urgently consult a doctor, undergo an examination and get specialist recommendations.
Myocardial infarction is a disease accompanied by necrosis of one or more areas of the heart muscle as a result of acute disruption of blood flow in the coronary arteries supplying the myocardium. Acute non-ST segment elevation myocardial infarction and ST-segment elevation myocardial infarction are types of acute coronary syndrome, which also includes unstable angina.
Myocardial infarction is the leading cause of death in most countries, including Russia. Timely hospitalization in many cases helps prevent irreversible damage to the heart muscle, but often patients misjudge the symptoms that arise and try to cope with them on their own, which leads to late consultation with a doctor. Therefore, in case of acute chest pain or other alarming symptoms, it is necessary to consult a specialist as soon as possible.
The risk of myocardial infarction increases with age; people over 60 years of age are more likely to get sick. However, recently the number of early myocardial infarctions has increased - in people under 40 years of age. Among patients under 70 years of age, men predominate, but after 70 years, the number of men and women with myocardial infarction becomes the same. This may be due to the protective effect of estrogens (female sex hormones), which reduce the likelihood of atherosclerosis, the main risk factor for heart attack.
The prognosis of myocardial infarction depends on the extent of damage to the heart muscle, the presence of concomitant diseases, the time of seeking medical help and the age of the patient. The mortality rate for acute myocardial infarction reaches 30%.
Synonyms Russian
Heart attack, MI.
English synonyms
Heart attack, acute myocardial infarction, MI, myocardial infarction.
Symptoms
The main symptom of acute myocardial infarction is sharp chest pain, which most often feels like a sharp squeeze. It usually lasts longer than 15 minutes and is not relieved by taking nitroglycerin. The pain may spread to the left shoulder, shoulder blade, neck, lower jaw, and may be accompanied by cold sweat, nausea and vomiting, and loss of consciousness. In some cases, the pain has an atypical localization - in the abdomen, spine, left or even right arm.
Sometimes a heart attack is preceded by nonspecific symptoms: for several days before a heart attack, a person may feel weakness, malaise, and discomfort in the chest area.
A heart attack may not be accompanied by a characteristic pain syndrome and may manifest itself only by such symptoms as shortness of breath, rapid heartbeat, weakness, and nausea. Subtle symptoms of myocardial infarction are especially common in women.
Thus, the main symptoms of acute myocardial infarction are:
- chest pain,
- dyspnea,
- cold sweat,
- feeling of fear,
- loss of consciousness,
- nausea, vomiting.
General information about the disease
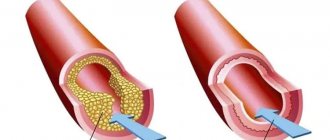
Myocardial infarction develops as a result of impaired blood supply to the heart muscle, which leads to a lack of oxygen and nutrients and necrosis (death) of the myocardium. The main cause of impaired blood flow in the vessels supplying the myocardium is atherosclerosis of the coronary arteries - the deposition of atherosclerotic plaques, consisting mainly of cholesterol, on the inner surface of the vessels. Then there is a proliferation of connective tissue (sclerosis) of the vessel wall and the formation of calcium deposits (calcification) with further deformation and narrowing of the lumen of the vessel until complete blockage. Subsequently, the so-called aseptic inflammation can develop in the atherosclerotic plaque, which, when exposed to provoking factors (physical activity, increased blood pressure, etc.) can lead to plaque rupture. In the area of damage, platelets accumulate, biologically active substances are released, which further enhance the adhesion (clumping) of blood cells, and as a result, a blood clot is formed, clogging the lumen of the coronary artery. Increased blood clotting also contributes to the formation of a blood clot. If blood flow in the vessels is not restored in the next six hours, irreversible changes occur in the myocardial tissue.
Rarely, myocardial infarction occurs with a sharp spasm or thromboembolism of pathologically unchanged coronary arteries, but this is observed only in 5% of cases.
Most often, myocardial infarction is localized in the anterior wall of the left ventricle, less often in the posterior wall of the left ventricle and the interventricular septum. Right ventricular infarction is rare. Transmural and subendocardial myocardial infarction are distinguished. With transmural pathological changes affect the entire wall of the heart, with subendocardial – from? up to ½ wall thickness. There is also a division into myocardial infarction without ST segment elevation and myocardial infarction with ST segment elevation. The presence of ST segment changes on the electrocardiogram suggests complete occlusion of the coronary artery and extensive myocardial damage with a higher risk of developing irreversible tissue necrosis. ST segment elevation is not observed when the artery is partially blocked - this may indicate myocardial infarction without ST segment elevation or unstable angina. However, only during myocardial infarction does the activity of cardiac enzymes change.
When the blood supply to the myocardium is disrupted, cell death begins, first of all, in the endocardium, and then the damage zone spreads towards the pericardium. The extent of the lesion depends on the degree of blockage of the artery, its duration, and the collateral circulatory system.
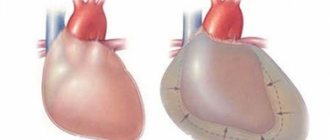
Necrosis in the tissues of the heart muscle causes acute pain. Extensive myocardial damage can lead to impaired contractile function of the heart, which is manifested by acute left ventricular failure with the development of pulmonary edema and cardiogenic shock. Cardiogenic shock, in turn, aggravates the course of myocardial infarction due to deterioration of coronary circulation. The result is severe heart rhythm disturbances, including atrial fibrillation.
Transmural infarction in some cases can lead to rupture of the heart wall or to an aneurysm - local thinning and protrusion of a section of the myocardium.
Who is at risk?
The main cause of myocardial infarction (up to 90% of all cases) is atherosclerosis. Therefore, risk factors for the development of atherosclerosis increase the likelihood of developing a heart attack. The risk group includes:
- men over 45 years of age and women over 65 years of age,
- suffering from obesity, dyslipidemia, arterial hypertension, diabetes mellitus,
- people whose relatives suffer from cardiovascular diseases and/or have suffered a myocardial infarction,
- smokers,
- leading a sedentary lifestyle,
- drug users (cocaine, amphetamines can provoke spasm of the coronary arteries),
- experiencing severe stress.
Diagnostics
Acute myocardial infarction in many cases is asymptomatic or atypical, which makes its diagnosis difficult. There are a number of diseases, the manifestations of which can often be similar to those of a heart attack: aortic aneurysm, angina pectoris, liver and biliary tract diseases, depression, esophagitis and others. Therefore, if a myocardial infarction is suspected, it is necessary to conduct a series of laboratory and instrumental studies to distinguish myocardial infarction from other pathologies and identify the extent and localization of damage, the duration of ischemia, and post-infarction complications. In addition, it is important to recognize the signs of concomitant diseases: pathology of the kidneys and respiratory system, diabetes mellitus, anemia. All this determines the further treatment regimen and prognosis of the disease.
Laboratory diagnostics
- General blood analysis. In acute myocardial infarction, leukocytosis may be observed. The number of leukocytes increases from the second hour after the onset of circulatory disorders and reaches a peak on the 2-4th day. It is important to pay attention to the number of red blood cells, since anemia worsens oxygen starvation of the heart muscle.
- Leukocyte formula. Leukocytosis with a shift of the leukocyte formula to the left and aneosinophilia is possible.
- Erythrocyte sedimentation rate (ESR). An increase in ESR indicates an acute inflammatory process.
- Troponin I (quantitatively) is a protein that is involved in muscle contraction. During a heart attack, its level usually increases starting from the 4-6th hour, maximum on the 2nd day, and normalizes within 6-8 days from the onset of the disease.
- Myoglobin. This is a protein found in muscle tissue, including the myocardium. During myocardial infarction, myoglobin levels increase within 4-6 hours.
- Alanine aminotransferase (ALT) and aspartate aminotransferase (AST). During myocardial infarction, the level of these enzymes is an indicator of the extent of damage to the heart muscle.
- Creatine kinase MB. An increase in its concentration is specific to damage to the heart muscle. Its level increases from the first hours and remains elevated for 2-3 days.
- General lactate dehydrogenase (LDH) is an enzyme that is found in almost all cells of the body and is involved in the utilization of glucose. The level of LDH increases with myocardial infarction, pathology of the liver, blood, and kidneys. During myocardial infarction, it remains elevated for 10-14 days.
- Lactate dehydrogenase 1, 2 (LDH, 1, 2 fractions). Forms of the enzyme lactate dehydrogenase, which are found mainly in the cells of the heart, renal cortex, and liver. These indicators can be used to assess the extent of damage during myocardial infarction.
- Antithrombin III. Synthesized in vascular endothelial cells and liver cells, it is involved in the inactivation of a number of blood coagulation factors. A decrease in the amount of antithrombin III indicates an increased risk of thrombosis. Its level is reduced in thromboembolism and atherosclerosis.
- Lupus anticoagulant screening test (LA1). Lupus anticoagulant is a complex of antibodies against phospholipids. Their presence may indicate autoimmune diseases and is also a sign of an increased risk of blood clots.
- Prothrombin index (PI), international normalized ratio (INR). The analysis is used to evaluate the extrinsic coagulation pathway and the activity of coagulation factors I, II, V, VII, and X. Hypercoagulability increases the risk of blood clots. During myocardial infarction, the prothrombin index may be increased.
- Glycated hemoglobin (HbA 1c, glycosylated hemoglobin, glycohemoglobin). Formed when glucose joins hemoglobin. This indicator allows you to estimate the amount of glucose in the blood over the last 120 days - this is the average lifespan of a red blood cell. A high level of glycated hemoglobin indicates a high glucose concentration over the past three months and indicates a high likelihood of complications of diabetes mellitus, which, in turn, increases the risk of myocardial infarction. The glycated hemoglobin test is used to assess the effectiveness of treatment and prognosis of myocardial infarction in patients with diabetes mellitus.
- Plasma glucose. Also used to diagnose diabetes.
- Iron in serum. Iron is part of cytochromes and is involved in cellular respiration. During myocardial infarction, iron levels may be elevated.
- Serum electrolytes. In acute myocardial infarction, the levels of sodium, potassium, magnesium, calcium, and chlorine may change. However, this does not always happen; with uncomplicated myocardial infarction, the level of electrolytes may not change.
- Serum uric acid. When the blood supply to the myocardium is disrupted, necrosis of cardiac muscle cells occurs with the breakdown of organic substances and the release of breakdown products, including uric acid. This, in turn, provokes the development of inflammation in the area of myocardial damage. Thus, uric acid levels may be elevated in large myocardial infarction.
- C-reactive protein, quantitative. During myocardial infarction, it is increased due to the inflammatory reaction.
- Triglycerides. Formed in the intestines from dietary fats. They are deposited in adipose tissue and consumed by cells as needed to obtain energy. Elevated triglyceride levels may indicate a high risk of atherosclerosis.
- Total cholesterol. These are compounds that are involved in the formation of atherosclerotic plaques. Its concentration can be increased during myocardial infarction resulting from atherosclerosis of the coronary arteries.
- Cholesterol – high-density lipoproteins (HDL) – is a fraction of total cholesterol that prevents the formation of atherosclerotic plaques.
- Cholesterol – low-density lipoproteins (LDL) is a fraction of cholesterol involved in the formation of atherosclerotic plaques.
- Cholesterol – very low density lipoproteins (VLDL). These are lipoproteins that are formed in the liver. They are carriers of phospholipids, triglycerides, and cholesterol. When released from the liver into the blood, they undergo chemical transformations with the formation of low-density lipoproteins
- Atherogenic coefficient. This is the ratio of “harmful” (LDL, VLDL, triglycerides) and “beneficial” lipoproteins (HDL). An increase in the atherogenicity coefficient indicates a high risk of developing atherosclerosis.
Other research methods
- Electrocadiography (ECG). Allows you to confirm the diagnosis of “myocardial infarction”, determine the location and degree of damage to the heart muscle, and identify signs of heart rhythm disturbances.
- X-ray of the chest organs. Used to detect cardiac aneurysm.
- Ultrasound examination of the heart. Allows you to identify the area of myocardial damage and evaluate the contractility of the heart.
Treatment
Therapy is prescribed individually depending on the patient’s age, the severity of the condition and the extent of damage to the heart muscle. Of great importance is the restoration of blood supply to the myocardium during the first 12 hours after the appearance of the first signs of myocardial infarction. This may prevent or reduce the degree of tissue necrosis. The main directions of therapy for acute myocardial infarction are pain relief, thrombolytic and anticoagulant therapy, reducing the load on the myocardium, prevention and treatment of complications that arise.
Prevention
Eat a healthy diet low in saturated fat and plenty of vegetables and fruits.
Sufficient physical activity.
Quitting alcohol and smoking.
Timely completion of preventive medical examinations to identify diseases that increase the risk of developing myocardial infarction.
Recommended tests
- General blood analysis
- Leukocyte formula
- Erythrocyte sedimentation rate (ESR)
- Troponin I (quantitative)
- Myoglobin
- Alanine aminotransferase (ALT)
- Aspartate aminotransferase (AST)
- Antithrombin III
- Lupus anticoagulant screening test (LA1)
- Coagulogram No. 1 (prothrombin (according to Quick), INR)
- Glycated hemoglobin (HbA 1c)
- Plasma glucose
- Serum iron
- Potassium, sodium, chlorine in serum
- Creatine kinase MB
- Lactate dehydrogenase (LDH) total
- Serum uric acid
- C-reactive protein, quantitative
- Triglycerides
- Total cholesterol
- Cholesterol – high density lipoprotein (HDL)
- Cholesterol – low density lipoproteins (LDL)
- Cholesterol – very low density lipoproteins (VLDL)
- Atherogenic coefficient
- Laboratory diagnosis of acute coronary syndrome and myocardial infarction (optimal)
- Laboratory diagnosis of acute coronary syndrome and myocardial infarction (minimal)
- Laboratory examination of the heart and blood vessels
Where is the pain hidden during myocardial infarction?
Pain during myocardial infarction is localized in the chest area, spreading mainly to the left side of the chest space or being fixed in the central zone. The patient’s appearance also attracts attention: the skin is pale, moist, blue discoloration is visible in the area of the nasolabial triangle.
Myocardial infarction is often characterized by pain spreading to the left or right arm. Patients often talk about unpleasant sensations in their wrists, so similar to being put on squeezing handcuffs. The pain can go to the left shoulder blade and spread around the neck. The abundance of such places often complicates diagnosis, especially since pain symptoms are cyclical, increase and disappear in waves, and then everything repeats again.
Sometimes symptoms are observed for several days, and people do not rush to see a doctor because they are not aware of the development of signs of a dangerous disease. Another interesting symptom of a heart attack is known, when a person experiences hallucinations against the background of acute intense pain.
Atypical forms of the disease attract attention when the symptoms and first signs of a heart attack are manifested not by pain, but by shortness of breath, a feeling of lack of air and an irregular heartbeat. Acute infarction develops when a focus of necrotic tissue is finally formed. At this time, the pain disappears, the pressure drops, and the pulse quickens. The pain may persist if the affected area during a heart attack expands.
The first signs of a pre-infarction condition in women
A clear understanding of the symptoms of pre-heart attack in women
, recognizing its first signs is important information that every person should have. This will prevent a heart attack.
In the body of an elderly woman, disruptions in blood circulation occur, and this is the main precursor to a heart attack. The sooner symptoms are recognized, the more effective methods of preventing an attack will be.
Severe pain appears in the chest area. It is often attributed to a manifestation of angina pectoris. However, after taking nitroglycerin or nitrosobid it does not stop
. In addition, attacks become more frequent - more than 20 times a day. The pain lasts up to 30 minutes and appears mainly at night. Urgent measures are needed, otherwise this may lead to myocardial necrosis. Often the pain radiates to the right side of the body, moving to the arm and collarbone area.
The main features of pre-heart attack in women over 50:
- sudden excitement;
- cold sweat;
- pain in the shoulder area;
- impaired coordination of movements;
- deep breath is impossible.
Each woman's body has different individual characteristics. It is useful to know about the presence of specific factors that precede myocardial infarction, inherent in individual women:
- increased weakness;
- sleep disturbance;
- nausea;
- dizziness;
- shortness of breath from the slightest physical exertion;
- increased emotionality;
- impulses of aggression.
Scheme of development of myocardial infarction
The atherosclerotic plaque loses its integrity and undergoes rupture. Its surface is corroded by erosion, which provokes inflammation. Plaque rupture is possible under the following circumstances: increased blood pressure, serious and exhausting physical activity, smoking, etc.
A blood clot forms that blocks the lumen of the coronary artery (thrombosis). The blockage occurs due to the clumping of platelets. A thrombus forms inside the plaque when its membrane ruptures, and only then comes out, closing the lumen of the coronary artery. If the blockage is sudden, a through myocardial infarction develops with necrotization of the entire thickness of the heart muscle. This is one of the most severe forms of the disease due to the high risk of death.
The coronary artery narrows sharply. With spontaneous or drug-induced dissolution of a blood clot and incomplete blockage of the artery, non-through infarctions are formed.
Typical symptoms
Signs depend on the individual characteristics of the patient’s body and the form of the emergency condition.
Classic situations, of which the majority are, are accompanied by the following moments:
- Chest pain is the first symptom of a heart attack. There are two options.
Unbearable in strength, pressing, burning, diffuse, diffuse localization. Nitroglycerin helps partially, but complete correction does not occur.
The discomfort may be moderate in intensity but last more than 30 minutes. Both cases require calling an ambulance and transporting to a hospital.
- Dyspnea. At rest. It intensifies against the background of physical activity, and other symptoms may worsen.
- Arrhythmia. Like bradycardia or increased contraction frequency. Usually both processes alternate within a short time.
- Cyanosis of the nasolabial triangle. It looks like a bluish ring surrounding the mouth and lips.
- Paleness of the skin, nails, mucous membranes.
- Impaired consciousness. Fainting, syncope. The patient finds it difficult to get out of them.
- Excessive sweating, hyperhidrosis.
- Coldness of the tips of the fingers, hands and feet.
Further, the manifestations are determined by the specific form of the pathological process.
Diagnosis and treatment for heart attack
An experienced doctor makes an accurate diagnosis at the first signs of illness. To help him - characteristic symptoms, a detailed clinical picture of a heart attack, electrocardiography indicators and identification of blood biomarkers indicating necrotic changes in the heart area. The first examinations upon treatment include a general blood test, biochemistry, echocardiography, and emergency selective coronary angiography.
Cardiologists deal with heart attacks; treatment depends on the severity of the pathology and how severe the symptoms are. The first signs of a heart attack in a woman or man indicate the need for urgent medical attention. The first and main tasks of doctors are to stop the development of necrosis of cardiac tissue, eliminate pain and associated complications.
In therapy, priority is given to the administration of painkillers, thrombolytic therapy, antiplatelet agents, and intravenous anticoagulants. In case of heart attacks, surgery of the heart muscle is possible - stenting and coronary artery bypass grafting.
Heart attacks are easier to prevent
The onset of a large heart attack can be fatal, so the importance of preventing it cannot be overestimated. What to do at the first symptoms? Of course, immediate medical attention is needed here. In addition to all the listed signs, special attention should be paid to such nuances
:
- an attack of pain appeared for the first time;
- increased frequency and duration of attacks;
- the onset of an attack is accompanied by a sharp pallor of the face;
- unexpected state of fatigue;
- cardiac arrhythmia;
- shallow breathing;
- I have a stomachache;
- pain in the chest in an immobilized state.
If symptoms of a pre-infarction condition are detected, medical first aid is needed. While waiting for a doctor's visit, the only methods of pre-medical assistance (DAP) are the following:
- put the patient to bed, be sure to place a pillow under her head;
- free the body from clothing that restricts breathing and movement;
- provide fresh air in the room;
- If the patient is diagnosed with coronary artery disease, give her a tablet of nitroglycerin or aspirin.
This completes the first aid. Further actions are carried out by the doctor. If the patient finds herself in extreme conditions where the ambulance may be delayed, chest compressions or artificial respiration are possible. It is advisable that this be done by a trained person.
Prognosis after heart attacks
In case of heart attacks, you should be observed by a specialized specialist. After an illness, the situation may be complicated by cardiac arrhythmias, acute heart failure, cardiogenic shock, pericarditis, mental disorders and other pathologies. A professional doctor will help reduce the risks of exacerbations after myocardial infarction.
Our clinic provides services to patients with all types of cardiac pathologies, including those who have suffered a cerebral infarction (ischemic stroke). It is these complications of brain damage that are considered one of the main causes of increased mortality throughout the world. Despite this, our doctors do everything possible to maintain and improve the quality of life of their patients.
Types of pathological process
Classification is carried out on several grounds.
Based on the form of functional impairment:
- Circular. It is one of the heaviest types. Several branches of the coronary circulation are blocked (there are two arteries in total, each branching along the path into the tissue).
Generalized malnutrition leads to the impossibility of adequate trophism. Mortality is about 80%; with timely assistance and transportation to a hospital within the first hour, the chances increase slightly.
Partial work of the affected area may remain; necrosis is not always complete.
- Transmural form. The exact amount of tissue involved is not known. But total necrosis of the area is observed, it is excluded from functional activity. Even with proper treatment and survival, severe heart failure develops for this reason.
- Actually large-focal MI. When a group of areas is involved in the pathological process. They are usually located asymmetrically.
Depending on the location, we can talk about an infarction of the anterior or posterior wall of the heart. The first option is less noticeable from a clinical point of view; false symptoms or the absence of a clear picture are possible.
Classification is carried out according to the prevailing symptom complex, the involvement of third-party organs and tissues:
- Cerebrovascular form. It can proceed in parallel with the classical one. The trophism of nerve clusters and cerebral structures is disrupted. The likely consequence is a stroke.
- Arrhythmic type. The main manifestation is a violation of heart rate. Tachycardia or a decrease in heart rate occurs in parallel with a change in the intervals between beats. The process is represented by extrasystole, fibrillation.
- Abdominal form. The clinical picture of an acute abdomen is typical. Nausea, vomiting, and unbearable pain in the abdominal cavity occur. Such patients are falsely mistaken for gastroenterological patients and sent to the appropriate department. Precious time is wasted and chances of survival are diminished.
- Asthmatic appearance. Shortness of breath, impaired consciousness, asphyxia and other “delights” are included.
All four are called atypical, and together they account for barely more than 10% of clinical situations worldwide.
Prognosis and complications
{banner_banstat10}
The outcome depends on the extent of the lesion. The larger the area, the lower the chances of survival (read more about the consequences and chances in this article).
If the necessary actions are taken in the first few hours, it is possible to prevent further necrosis. But even with the success of the measures, 60% of patients die in the first 2 years, another 20 within 5 years.
Attention:
A competent approach to rehabilitation does not guarantee life, but it significantly improves prognosis.
The main causes of death after a major heart attack:
- Heart failure. Leads to asystole (stop) or relapse of necrosis. The second episode is fatal in 95% of situations.
- Stroke. Acute circulatory disorder in the brain.
You can minimize risks by completely revising your lifestyle. Quitting smoking and alcohol is mandatory.
Physical activity is at a minimal level, although most patients with this diagnosis become disabled after suffering the condition (step-by-step rehabilitation is described here).
Symptoms of atypical forms of MI
Abdominal type:
- Acute pain in the abdomen, in the epigastric region. Partially relieved by Nitroglycerin, which indicates a cardiac origin.
- Nausea.
- Vomiting without signs of relief. It is a reflex, so the discomfort does not subside as with
- poisoning Heartburn, dyspeptic symptoms.
Cerebrovascular form:
- Strong headache. In the occipital, parietal regions. It may be diffuse and not have a specific localization.
- Vertigo. Up to the impossibility of orientation in space. The vestibular apparatus does not function normally due to damage to the cerebellum and its ischemia.
- Nausea without vomiting.
- Loss of consciousness. May be repeated during one emergency episode. Deep fainting requires urgent help.
Stroke becomes a natural result of cerebral ischemia.
Arrhythmic form:
- Tachycardia or decreased heart rate.
- Feeling of freezing in the chest, turning over, missing blows.
- Asthmatic type:
- Choking, asphyxia. It gets worse at night and when lying down.
- Increase in heart rate.
Pain syndrome is minimal or completely absent.
To limit conditions, the patient is urgently transported to the hospital. The following shows urgent actions.
Diagnostics
Carried out in a hospital. Immediately after moving the patient within the walls of the institution, a minimum of studies are prescribed. Measurement of blood pressure, heart rate, and auscultation.
Then the stabilization of the victim’s condition begins with the use of drugs based on organic nitrates and other means.
An extensive, large-focal infarction has an unfavorable prognosis in 70% of cases, therefore the chances of recovery and even bringing the person’s position to an acceptable state are low.
If successful, the patient is transferred to intensive care, and as he stabilizes, he is transferred to a regular ward. Then a thorough diagnosis is prescribed.
Activity:
- Oral interview and history taking to identify key points.
- Measurement of blood pressure, heart rate. After the fact, to establish the status and success of primary actions.
- Electrocardiography. To identify consequences and causes.
- Echocardiography. Makes it possible to see all complications and organic defects. It is considered the main diagnostic method.
- Daily Holter monitoring if indicated.
- MRI of the chest.
The differential technique requires special tests. Shchetkin-Blumberg and others (to identify damage to the digestive tract). The task of urgent differentiation lies with doctors.