Cardiosclerosis, or the development of connective scar tissue in the heart muscle, is an irreversible process that gradually impairs the contractility of the heart. Cardiosclerosis can occur not only after myocardial infarction, but also as a result of myocarditis. In this regard, it is necessary to know in which cases the formation of cardiosclerosis is more likely, and how to prevent these processes.
Myocarditis is a rather serious disease that can not only cause dangerous cardiac disorders, but also provoke the development of serious complications and long-term consequences.
In order to talk about the occurrence of complications after myocarditis, both in acute and long-term periods, it is necessary to understand what this nosological form is.
Myocarditis is an inflammatory pathomorphological change in the thickness of the heart muscle, causing disturbances in the activity of cardiac smooth muscle cells.
(cardiomyocytes) at the molecular level, as well as causing certain clinical manifestations.
Causes of cardiosclerosis
1. Functional disorders:
- Damage to the heart muscle as a result of inflammatory diseases.
- Hypoxia due to insufficient blood supply to the heart muscles due to narrowing of large cardiac vessels.
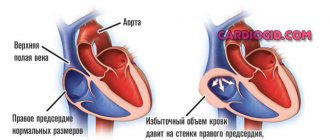
- Stretching of the walls of the heart, which leads to an increase in its volume.
2. Lifestyle and bad habits of the patient:
- Alcohol abuse and smoking.
- No, minimal or excessive physical activity.
- Repetitive stress.
- The habit of overeating and, accordingly, excess body weight.
Hereditary factors play an important role in the occurrence of the disease.
Forecast
With timely detection of AA, properly selected conservative therapy, as well as adherence to a special diet in combination with lifestyle correction, the prognosis is favorable. In cases where AA is detected at late stages, in which severe complications such as aortic aneurysm or thrombosis of the mesenteric arteries are noted, the prognosis is significantly aggravated.
Prevention involves strict adherence to diet, normalization of body weight and cessation of bad habits (primarily smoking). It is important to avoid a sedentary lifestyle, however, physical activity should also be dosed. To begin with, the patient is recommended to walk for at least 30 minutes a day, then their duration increases as endurance develops. After a few weeks, you can add complexes of therapeutic exercises or swimming in the pool.
It is important to avoid stress and minimize psycho-emotional stress. In addition, it is necessary to carefully monitor the pressure - it should not exceed 130/85 mm Hg. Art.
Classification of cardiosclerosis
According to the morphological principle, focal (most often occurs as a complication after myocardial infarction and myocarditis) and diffuse cardiosclerosis, in which the connective tissue spreads to the entire myocardium, are distinguished.
For etiological reasons, the following types are distinguished:
- Post-infarction. As a result of myocardial infarction, scars form at the site of necrotic damage, which reduces the contractility of the heart muscle. The more cases of myocardial infarction a patient has suffered, the more scar tissue is formed. The threat of chronic aneurysm increases due to protrusion of the walls of the heart muscle, which is stretched and weakened by connective tissue. Aneurysm rupture is associated with high mortality.
- Myocardial. Myocardial inflammation develops mainly in young patients with chronic allergic and infectious diseases. With this form, the right ventricle of the heart increases in volume and is insufficiently supplied with blood.
- Atherosclerotic. As a rule, it is the result of atherosclerosis of the coronary vessels and coronary heart disease. This form of the disease develops over a long period of time, because due to damage to blood vessels, heart cells do not receive enough oxygen, hypoxia develops, the course of coronary heart disease is complicated, and cholesterol levels increase. This leads to diffuse cardiosclerosis, which is accompanied by arrhythmia.
Consequences
A patient with the diagnosis in question needs lifelong medical supervision. Knowing what post-infarction cardiosclerosis is, one cannot ignore the situation, as this leads to inevitable complications in the form of the following consequences:
- Diffuse cardiosclerosis: symptoms, treatment tactics, preventive measures
- pericardial tamponade;
- atrial fibrillation;
- thromboembolism;
- blockades;
- pulmonary edema;
- tachycardia;
- decreased automaticity of the sinoatrial node.
These processes negatively affect a person’s quality of life. The patient loses tolerance to physical activity, loses the opportunity to work and lead a normal life. Advanced cardiosclerosis provokes the appearance of an aneurysm, the rupture of which leads to death in 90% of non-operated patients.
Symptoms of cardiosclerosis
Very often the initial stages of the disease are asymptomatic. In the clinic of the onset of sclerosis, the first symptom may be arrhythmia. Typical manifestations of the diffuse form should be considered heart failure and disturbances in the rhythm of the heartbeat.
Symptoms regardless of the form (post-infarction or atherosclerotic):
- heart rhythm disturbances;
- dyspnea;
- the appearance of fluid in the abdominal and pleural cavities;
- pain in the heart area;
- increased heart rate;
- pulmonary edema;
- increase in liver size.
As the area of affected heart tissue increases, the severity of symptoms increases.
Very often the course of cardiosclerosis is accompanied by arterial hypertension. In this case, high blood pressure alternates with long periods of normal blood pressure.
How to make a diagnosis?
ECG signs
Post-infarction cardiosclerosis is established on the basis of anamnesis (previous infarction), laboratory and instrumental diagnostic methods:
- ECG - signs of a heart attack: a Q or QR wave may be observed, the T wave may be negative, or smoothed, weakly positive. The ECG may also show various rhythm disturbances, conduction disturbances, and signs of an aneurysm;
- X-ray - expansion of the heart shadow mainly on the left (enlargement of the left chambers);
- Echocardiography - zones of akinesia are observed - areas of non-contractile tissue, other contractility disorders, a chronic aneurysm, valve defects, an increase in the size of the heart chambers can be visualized;
- Cardiac positron emission tomography. Areas of reduced blood supply are diagnosed—myocardial hypoperfusion;
- Coronary angiography - conflicting information: the arteries may not be changed at all, or their blockage may be observed;
- Ventriculography - provides information about the functioning of the left ventricle: it allows you to determine the ejection fraction and the percentage of scar changes. Ejection fraction is an important indicator of heart function; if this figure decreases below 25%, the prognosis for life is extremely unfavorable: the quality of life of patients significantly deteriorates; without a heart transplant, survival is no more than five years.
At-risk groups
The risk of cardiosclerosis is highest in patients with pathologies in the development of the heart and cardiovascular diseases, as well as in people with various types of allergies.
Pregnant women can be identified as a separate group. Pregnancy causes hormonal, autonomic, metabolic and hemodynamic changes in the body of women and can act as a proarrhythmogenic factor. Complex heart rhythm disturbances are diagnosed both in pregnant women with cardiovascular pathology and in patients without changes in metabolism and the condition of internal organs.
Cardiosclerosis in children is possible against the background of myocardial pathologies, for example, inflammatory and dystrophic processes, in particular diseases of the heart muscle caused by metabolic disorders in heart cells. These biochemical disorders significantly weaken the contractile, conductive, excitatory and automatic functions of the myocardium.
Deadly complications
Typical disorders of the body have already been described above, but there are a number of pathologies that pose a direct threat to life and cause death, including sudden death. These include:
- Aneurysm . The wall of the organ becomes thinner and stretched, and rupture with cardiac tamponade can occur at any time.
- Blockade . The impulse is not transmitted to individual parts of the heart, which stop contracting.
- Atrial fibrillation or extrasystole is the uncoordinated work of different parts of the organ. If fibrillation is severe and emergency assistance is not provided, the complication can be fatal.
- Acute heart failure is the final stage of chronic heart failure, when the organ is no longer able to provide adequate blood flow. The cause of death is ischemia.
Cardiosclerosis medications
The European Society of Cardiology recommends the following medications for the treatment of cardiosclerosis, eliminating the symptoms of the disease, as well as its root cause:
- Antihypertensive drugs. To maintain vascular tone and normalize blood pressure, ACE inhibitors (Captopril, Enalapril, Ramipril) are prescribed; calcium antagonists (Amlodipine, Semlopin, Phenigidine), beta blockers (Atenolol, Bisoprolol, Metoprolol), antiplatelet drugs (Aspirin), lipid-lowering drugs (Simvastatin, Atorvastatin, Allesta).
- Cardioprotectors (antianginal agents). Their task is to maintain the functional activity of the heart and counteract the influence of negative exo- and endogenous factors on it. These include organic nitrates (Nitroglycerin, Isosorbide Mono- and Dinitrate); sydnonimines (Mosikor, Sidocard); metabolic agents (Trimetazidine).
- To normalize heart rate and conduction: amiodarone (Amiodarone), dronedarone (Multak).
- To normalize metabolic processes - potassium and magnesium preparations: Panangin, Asparkam, Magnerot.
- Antibiotics and corticosteroids: for myocarditis and other inflammatory processes.
Development mechanism
Atherosclerosis develops as a result of disruption of two mechanisms that ensure the functionality of tissue blood supply.
1st mechanism
The first mechanism is a metabolic disorder that directly affects lipid (fat) metabolism. This leads to an increase in the concentration of cholesterol, non-esterified (free) fatty acids and triglycerides. At the same time, the content of phospholipids in the blood decreases, and cholesterol is converted into a finely dispersed state:
- alpha lipoproteins - strong compounds with proteins and triglycerides;
- beta lipoproteins are fragile molecules – prebeta lipoproteins.
Once in the walls of blood vessels, lipoproteins quickly break down, releasing triglycerides and cholesterol, and have an atherogenic effect on the arteries, that is, they damage them. In atherosclerosis, due to a decrease in the level of alpha proteins, the concentration of fragile lipoproteins increases. Depending on the nature and characteristics of lipid metabolism, the predominance of certain groups of lipoproteins, there are 5 types of hyperlipidemia (increased fat content in the blood).
The most pronounced pathogenic effect is observed when hyperlipidemia of types 2 and 3 occurs, which develop due to the predominance of beta and prebeta lipoproteins, respectively. In addition, an important factor is the increase in free fatty acids necessary for the production of triglycerides and cholesterol.
Their effect also helps to reduce the sensitivity of body cells to insulin, which reduces the speed and quality of transformation of glucose into glycogen, leading to hyperglycemia (increased blood sugar) and other local disorders of carbohydrate metabolism. In parallel, pathologies of protein metabolism are also observed, which is due to the direct interaction of proteins and lipids.
Cholesterol plaque in the lumen of the artery
2nd mechanism
The second mechanism, interruptions in which occur during atherosclerosis, is a morphological change in the vascular walls, that is, a violation of their permeability. As a rule, the ability to pass certain substances through the walls of blood vessels increases, which is caused by a decrease in the quality of microcirculation and an increase in the level of acidic mucopolysaccharides.
At the same time, the number of pores increases, resulting in increased permeability of the vascular walls. Often the cause of such disorders is a high level of concentration of local hormones, for example, bradykinin, which, in turn, causes an increased formation of catecholamines.
In the pathogenesis of atherosclerosis, a significant role belongs to the growth of enzyme activity directly in the vascular wall itself, and specifically elastase, which causes changes in the vascular framework. An additional aspect of the development of this pathology can also be an increase in blood pressure (blood pressure), which is a mechanical factor in the appearance of damage.
List of used literature
- Stryuk R.I., Shoikiemova D.U., Borisov I.V.; State Budgetary Educational Institution of Higher Professional Education "Moscow State Medical and Dental University named after. A.I. Evdokimov" Ministry of Health of the Russian Federation, Moscow, Russia / Pregnancy as a risk factor for heart rhythm disturbances
- POKROVSKAYA E.M., 2, Ph.D., N.A. VOLOV 2, Ph.D., I.S. VASILYEVA 2, GORDEEV I.G. 1, Doctor of Medical Sciences, Professor, PAVLIKOVA E.P., 2, Doctor of Medical Sciences, Professor 1 State Budgetary Educational Institution of Higher Professional Education “Russian National Research Medical University named after. N.I. Pirogov" of the Ministry of Health of Russia, Department of Hospital Therapy No. 1, Faculty of Medicine 2, State Budgetary Institution "City Clinical Hospital No. 15 named after. O.M. Filatova "DZ Moscow / NEW OPPORTUNITIES FOR TREATING PATIENTS WITH HEART FAILURE DUE TO POST-INFARCTION CARDIOSCLEROSIS
- Berezin A. E., Doctor of Medical Sciences, Professor of the Department of Internal Medicine No. 2 of the 1st Medical Faculty of Zaporozhye State Medical University / Combined potassium and magnesium preparations in the treatment of patients with high cardiovascular risk.
Clinical example
An important stage in compensating for the general condition is the psychological component of the patient and his adherence to treatment.
I would like to give an interesting example from the experience of my colleague. Patient N., 47 years old. Suffered a large-focal myocardial infarction. The diagnosis was made based on an ECG and troponin test. The lower and lateral walls and the apex of the left ventricle were affected. The typical picture of the disease (acute pain syndrome, circulatory disorders) was absent, and therefore, he sought help only 12 hours after the acute thrombosis.
Thrombolytics were ineffective in the long term (more than 4-6 hours), symptomatic therapy was carried out. The patient felt excellent, refused treatment and the prescription of preventive medications, and left the hospital on his own.
After 3 months, he was readmitted to the hospital with severe signs of left ventricular failure. “The diagnosis was made: IHD. Post-infarction cardiosclerosis. CHF III. FC III. Left ventricular aneurysm.” Full life activity was no longer possible. The patient died from cardiac tamponade on the 10th day. If doctors' instructions were followed, this condition could develop only after several years.
Thus, post-infarction cardiosclerosis is a problem faced by almost every person who has suffered a myocardial infarction. It is necessary to understand that the appearance of any signs of cardiac dysfunction that have not previously manifested is an indication for urgent medical help. Only properly selected therapy will ensure a comfortable life.
Frequently asked questions about cardiosclerosis
Which doctor treats cardiosclerosis?
If you suspect cardiosclerosis, you should contact a cardiologist.
What signs should you see a doctor for?
High blood pressure; arrhythmia; increased fatigue and swelling of the limbs.
Can cardiosclerosis develop in children?
Cardiosclerosis in children can develop against the background of inflammatory and dystrophic processes in the myocardium - in particular, diseases of the heart muscle caused by metabolic disorders in heart cells.
Diagnostics
Source: US Army photo by Jason W. Edwards / DVIDS
If a person experiences symptoms such as sharp pain in the chest, dizziness, difficulty swallowing and numbness of the limbs, he has every reason to suspect the development of atherosclerosis. When contacting a doctor, you should talk in detail about all manifestations of the disease. Based on the patient’s complaints and data obtained during the examination, the specialist can make a preliminary diagnosis, to confirm which a number of diagnostic studies are prescribed.
The emphasis is on hardware diagnostic methods:
- radiography;
- Ultrasound;
- angiography;
- aortography;
- CT or MRI.
Additionally, a blood test is prescribed to determine the level of total cholesterol, lipoproteins and triglycerides. In combination with medical history data, the research results make it possible to make a final diagnosis and begin therapeutic measures.