Optic neuritis is an inflammatory process that damages, often suddenly, nerve fibers.
Two forms of the disease
- Intrabulbar, when the localization of inflammation occurs in the initial part of the nerve and does not extend beyond the tissues of the eyeball.
- Retrobulbar, in which the visual canals located outside the eye are acutely affected.
General information
Optic neuritis is an inflammatory process in the optic nerve. The disease in most cases involves the trunk and sheaths of the optic nerve (n. Opticus). Among the causes of ocular disability (low vision/blindness), inflammatory diseases of the optic nerve of various origins, according to various authors, occupy from 20 to 28%.
Optic nerve
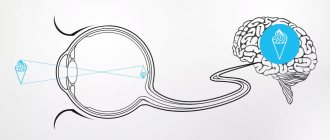
The optic nerve is the 2nd pair of cranial nerves (cranial nerves), formed by the axons of retinal ganglion cells. The optic nerve is a part of the brain in its development, which distinguishes it from other cranial nerves. It begins with the optic disc located on the retina, exits the eyeball through the cribriform plate of the sclera, heading back in the orbit, then passes into the cranial cavity through the bony optic canal. Further, after leaving the optic canal, the optic nerves at the base of the brain form an incomplete optic chiasm and pass into the optic tracts (Fig. below).
The length of the optic nerve in adults varies between 35-55 mm. Along its length there are several sections:
- Intrabulbar (intraocular) - 0.5-1.5 mm long, the beginning of the nerve from the disc to the point of exit from the sclera.
- Retrobulbar (orbital) - 25-35 m long, from the point where the nerve exits the sclera to the orbital opening of the optic canal.
- Intracanal - 5-8 mm long, from the orbital canal of the optic nerve to its intracranial foramen.
- Intracranial (intracranial) - 4-17 mm long, from the point where the nerve exits the optic canal to the chiasm.
It should be noted that as inflammatory exudate appears and nerve fibers are compressed by edema, as well as the toxic effects of exudate on them, the axial cylinders/myelin sheaths of the optic fibers undergo dystrophic processes, degeneration and atrophy (death of the retinal ganglion mother cell). At the same time, the structural elements of the optic nerve do not possess any regenerative ability.
In accordance with the predominant localization of the inflammatory process, the following are distinguished:
- Actually, optic neuritis (optic neuritis), in which the optic disc is also involved in inflammation. In this case, intrabulbar neuritis can occur with isolated damage to the optic disc (optic disc neuritis/papillitis).
- Retrobulbar neuritis - with a predominant localization of the inflammatory process behind the eyeball.
Since the visual analyzer is connected to the entire body through various physiological/anatomical mechanisms, functional and morphological changes occur in it during general diseases. In fact, most pathological changes in the organ of vision (with the exception of local infections/traumatic injuries) are a manifestation of systemic or general diseases (for example, with progressive chronic demyelinating disease of the central nervous system, multiple sclerosis).
High level of disability due to the development of partial atrophy of n. Opticus, leading to irreversible changes in the visual apparatus, as well as the prevalence of the disease among relatively young people, give optic neuritis a high social significance.
Helpful information
To understand the essence of the problem of people diagnosed with optic neuritis, it is worth taking a closer look at the optic nerve. It is known that anatomically it has a process structure. It represents the neurons of the retina. The latter can absorb visualization and transmit information about it in the form of nervous vibrations. Their transportation is transmitted along axons to the visual part of the cerebral zone. All parts of a nerve are made up of millions of branches. The origin comes from the disk, which is located on the retina. It can be seen during a routine examination by a doctor. That part located in the inner region of the orbit is called intrabulbar. When the optic nerve leaves the orbit and makes its way to the cavity of the cranium, this part of it is called retrobulbar. The ending takes place in the visual centers of the midbrain and diencephalon. Along its entire length there are dense membranes, closely connected with nearby parts of the orbit, brain and cerebral surfaces. Therefore, quite often neuritis manifests itself in the formation of inflammatory anomalies.
Pathogenesis
Inflammation of the optic nerve can involve both the trunk and the optic nerve sheath. The small cell infiltration/inflammatory edema that develops, including in the optic nerve head, causes compression of the optic fibers with gradually developing degeneration, which causes a sharp decrease in visual acuity. Some fibers, after the acute inflammatory process subsides, can restore their function, which is manifested clinically by an improvement in vision. In severe cases of optic neuritis, disintegration of nerve fibers and their replacement by glial tissue may occur with the development of optic nerve atrophy, accompanied by irreversible impairment of the function of the visual analyzer (decrease in visual acuity).
In addition to the inflammatory process in the optic nerve, its damage may be based on the process of destruction of its myelin sheath (demyelination of nerve fibers), which occurs in multiple sclerosis . Demyelinating lesions of the optic nerve are in practice referred to as retrobulbar neuritis .
The above pathological processes cause dysfunction of the visual analyzer (transmission of information from the retinal receptors that perceive the image), which is clinically manifested by a decrease in visual acuity/disorder of color perception or loss in the optical fields. As the disease progresses, irreversible damage occurs to an increasing number of optical fibers with the gradual filling of the areas of destruction with growths of connective tissue.
Classification
The classification of the disease is based on the localization of the pathological process and the etiological factors causing it. Based on localization, intrabulbar and retrobulbar optic neuritis are distinguished. In turn, retrobulbar neuritis can occur in 3 forms:
- Axial . Characteristically, the lesion is predominantly in the axial bundle. Manifests with the appearance of central scotomas/sharp decline in central vision.
- Peripheral . The localization of the inflammatory process in the peripheral fibers occurs with severe pain, which is caused by the formation of intrathecal exudate, which provokes pain. Characteristic is a narrowing of the visual fields with preserved central vision.
- Transversal . The inflammatory process covers the entire diameter of the nerve trunk. Characterized by severe impairment of visual function up to complete blindness.
Based on the etiological factor, infectious, ischemic, parainfectious, demyelinating, autoimmune and toxic neuritis are distinguished.
Based on topographic location, the following lesions are distinguished: n. opticus:
- orbital;
- intracanalicular;
- intracranial.
Treatment of optic neuritis
Treatment must be carried out in a hospital setting; it should begin as early as possible, in order to avoid the disease becoming chronic and developing complications. Source: Modern view on the problem of optic neuritis (systematic review). Krivosheeva M.S., Ioileva E.E. Saratov Scientific and Medical Journal, 2021. p. 602-605. For patients with optic neuritis, diet No. 15 is indicated - a general table, in the absence of indications for other types of therapeutic diets.
The basis of treatment is etiotropic therapy aimed at eliminating the primary disease that caused optic neuritis. Until the etiology of the disease is clarified, remedies are used to reduce the symptoms of inflammation, remove swelling, allergic manifestations, and improve metabolism. For this purpose:
- glucocorticosteroid drugs, if they are intolerant - non-steroidal anti-inflammatory drugs (prescribed in rare cases);
- antibacterial or antiviral therapy;
- antifungal agents to prevent fungal infection due to a long course of antibiotics;
- detoxification therapy – intravenous drip administration of saline solutions;
- antihistamines;
- diuretics;
- products that improve microcirculation;
- neuroprotectors;
- vitamins.
In addition to medications, physical therapy may be used to treat optic neuritis.
With papillitis, as well as the infectious-toxic etiology of the disease, the prognosis is more favorable than with other types of optic neuritis - in 75-90% of cases, with proper treatment, vision is completely restored. When the optic nerve is damaged due to autoimmune, demyelinating diseases, collagenosis, sarcoidosis, and specific infections, relapses often occur, incomplete restoration of vision, and nerve atrophy is possible. Source: Results of treatment of optic neuritis. Latypova E.A. Saratov Scientific and Medical Journal, 2021. p. 875-879.
Causes
The etiology of inflammation of the optic nerve is varied. The main etiological factors are:
- Viral infections that occur in a chronic form ( herpes infection , mononucleosis ), causing disturbances in immune reactivity, which leads to the production of antibodies to the tissues of the optic nerve and the development of autoimmune inflammation outside the orbital part of the nerve.
- Acute/chronic diseases ( sore throat , influenza , erysipelas , smallpox , tuberculosis , typhus , malaria , brucellosis , syphilis ), persistent infectious foci located nearby ( sinusitis ), less often - relatively distant foci ( cystitis / pyelonephritis ) in which the introduction of an infectious agent in the tissue of the optic nerve occurs hematogenously.
- Inflammatory processes in the eye orbit: chorioretinitis , uveitis , iridocyclitis .
- Focal infection of the teeth, sinuses, ears ( otitis ), nasopharynx ( tonsillitis ).
- Inflammatory diseases of the meninges ( meningitis / encephalitis ), lesions of cerebral tissue ( multiple sclerosis ).
- Neuroinfections ( Lyme disease , neuroAIDS , neurosyphilis , tuberculous meningitis ).
- Brain tumors (neoplasms of the optic chiasm ( chiasma / glioma ), or other localization, directly compressing the chiasm area with impaired metabolism/blood supply to the optic nerve tissue.
- Some endocrine ( thyrotoxicosis / diabetes mellitus ) and metabolic processes are based on degeneration of nerve fibers (pregnancy pathology, toxic damage to the optic nerve with methyl alcohol, tobacco, lead, iodine preparations, pesticides, some medications), fasting, vitamin deficiencies .
Symptoms
Introtrobulbar optic neuritis
An acute disorder of visual function is characteristic, and their nature/severity of inflammation of the optic nerve is determined by the degree of damage to the trunk and membranes. Neuritis of the optic nerve is manifested primarily by a decrease in visual acuity, the indicators of which depend on changes in the papillomacular bundle. With partial damage, visual acuity may not be impaired, but spots appear in the field of vision - central/paracentral, round or arch-shaped scotomas, but can also be significantly reduced (at the initial stage, myopia up to 2 diopters).
Symptoms of optic neuritis are manifested by a narrowing of the boundaries of the visual field, a decrease in dark adaptation and color perception, a high frequency of flicker fusion is noted, as well as a decrease in electrical sensitivity and a low level of n lability. Opticus. With total damage to the diameter of the nerve, visual acuity can drop sharply up to complete blindness. Symptoms of the pathology appear predominantly in one eye.
At the initial stage of neuritis, the pathognomonic picture is represented by changes in the optic nerve head: blurred boundaries, moderate vasodilation, hyperemia, exudative swelling, the presence of streak-shaped hemorrhages in the tissue of the disc/peridiscal region. When the vascular funnel is filled with exudate and the adjacent layers of the vitreous are immobilized, unclear visualization of the fundus is noted.
In the acute period, symptoms of inflammation of the optic nerve last 3-5 weeks, and then gradually the swelling/hyperemia of the disc disappears, hemorrhages resolve and the boundaries of the disc acquire clear outlines again. In severe cases, ophthalmoscopy reveals a pale disc with pronounced vasoconstriction and clear boundaries and atrophy of n. opticus.
Retrobulbar optic neuritis
Symptoms of damage to the optic nerve with retrobulbar neuritis n. opticus. determined by the type of inflammatory changes.
With axial inflammation, the pathological process primarily involves a bundle of axons passing through the optic nerve. Characterized by a pronounced disorder of central vision with the formation of central scotomas throughout the entire visual field and a significant decrease in functional tests.
With the peripheral type of retrobulbar neuritis, the inflammatory process in the nerve sheaths spreads deep into the nerve trunk. A significant amount of exudate accumulates under the optic nerve sheath, causing the appearance of “shell-like” pain in the eye, which increases during movement of the eyeball. Central vision is not affected, but there is a concentric narrowing of the visual fields.
In the most severe form - transversal type of retrobulbar neuritis , the inflammatory process completely covers all tissues of the optic nerve. Functional tests with extremely low scores. In the acute course, visual acuity decreases sharply, in some cases to the point of blindness, while in chronic retrobulbar neuritis the decline in vision occurs gradually.
However, regardless of the type of retrobulbar neuritis, there are no changes in the optic nerve head and only 1-2 months after the manifestation of the disease can decolorization of the disc, as well as signs of partial/total atrophy of the n. opticus.
Advantages of treatment in Israel
- High level of qualifications and experience of doctors.
- Equipping clinics with modern equipment.
- Development of an individual comprehensive therapeutic program.
- Comfortable conditions for staying in the clinic.
- Reasonable prices.
Completing a full course of therapy in the initial stages of the disease will make it possible, after a short time, to restore visual functions and return to normal life. Don’t waste time, contact the clinic of your choice and start treatment.
- 5
- 4
- 3
- 2
- 1
(0 votes, average: 5 out of 5)
Tests and diagnostics
The diagnosis of optic neuritis is made based on a thorough history (pre-existing diseases, symptoms, rate of progression) and ophthalmological/neurological examination of the patient.
Ophthalmological examinations include:
- Visometry. Characteristic is a decrease in visual acuity to 0.1-0.2 diopters, less often to light perception, which cannot be corrected by lenses.
- Determination of color perception using color tables. Characterized by a decrease in color saturation/brightness.
- Perimetry. Characteristic is the presence of scotomas (central, peripheral, paracentral) in the visual fields.
- Ophthalmoscopy. Allows you to determine hyperemia/swelling of the optic disc, the presence of petechial hemorrhages, disc pallor (with the development of atrophy).
- Tonometry. In order to identify increased IOP, characteristic of a number of diseases that can contribute to the development of neuritis.
Neurological studies to assess the neurological status of the patient, allowing to identify cerebral/focal cerebral:
- MRI of the brain/orbit of the eye. To visualize brain pathology (areas of demyelination, inflammatory foci, tumor) and identify compression/edema/damage to the orbital part of the n. Opticus. X-ray of the paranasal sinuses/chest organs.
- Ultrasound of the optic nerve.
- Study of cerebrospinal fluid (chemical/cellular composition of the cerebrospinal fluid).
To identify the etiology of optic neuritis, blood cultures for sterility, ELISA/PCR studies, consultations with an immunologist, neurologist, infectious disease specialist, endocrinologist and other specialists may be prescribed.
Differential diagnosis of optic neuritis is carried out with intrabulbar lesions, ischemic optic neuropathy, and neuromyelitis optica. With the gradual development of atrophy n. Opticus it is necessary to exclude the hereditary mitochondrial disease Leber's disease (syn. Leber's syndrome).
Diagnosis of optic neuritis
It is easy to recognize a typical case of optic neuritis. It is much more difficult to diagnose mild neuritis or inflammation with edema, which are similar to pseudoneuritis and congestive disc. The main difference is the preservation of visual functions.
If there are symptoms of increased intracranial pressure, a spinal tap is performed to confirm a congestive disc. It is most difficult to distinguish neuritis from edema or complications of a stagnant disc, since in both cases there are visual disturbances.
The diagnosis of neuritis can be confirmed by the presence of small hemorrhages or foci of exudate in the disc tissue or retina. The most informative method for diagnosing optic neuritis is fluorescein angiography of the fundus.
Signs of neuritis according to the severity of the process:
- mild: moderate hyperemia of the optic disc, unclear boundaries of the optic disc, dilatation of arteries and veins;
- pronounced: sharp hyperemia of the disc, the boundaries of the disc merge with the retina, white spots and many hemorrhages appear in the peripapillary zone;
- transition to atrophy: disc blanching, narrowing of arteries, resorption of exudate and hemorrhages.
Forecast
In mild cases, optic nerve neuritis is benign and in 75% of cases, visual acuity is restored after 4-6 weeks. However, at the same time, other parameters of the visual analyzer function (contrast sensitivity/color vision) are often not fully restored. Progressive chronic disease leads to persistent disabling disorders - optic nerve atrophy and irreversible vision loss, the development rates of which vary between 22-25%.
List of sources
- Borisevich E. S. Clinical manifestations, diagnosis and outcomes of optic neuritis / Borisevich E. S., Shamal D. Yu., Klyuiko Yu. D., Kachan T. V. // Young scientist. - 2021. - No. 13 (147). — pp. 146-149.
- Zhaboedov G.D. Lesions of the optic nerve / G.D. Zhaboyedov, R.L. Skripnik // GEOTAR-Media. - 2006. - 286 p.
- Gustov A.V. Practical neuro-ophthalmology / Gustoe A.V., Sigriansky K.I., Stolyarova Zh.P. // Nizhny Novgorod State Medical Academy, 2014. - pp. 260-263.
- Kruzhkova G.V. Pathology of the fundus and optic nerve/G.V. Kruzhkova, M.S. Agronovich //MEDpress-inform, 2014. - pp. 32-35.
- Kanski, D. Clinical ophthalmology: a systematic approach. - M.: Logosphere., 2006. - 744 p.