Diseases that begin with the letter "P": Felon, Panic attack, Pancreatitis, Papillomas, Paralysis, Bell's palsy, Paranoia, Paraproctitis, Facial nerve paresis, Periodontitis, Periodontal disease, Paroxysm, Paroxysmal tachycardia, Scab (favus), Pediculosis, Testicular torsion cord, bone fracture, rib fracture, femoral neck fracture, post-term pregnancy
Paroxysmal tachycardia is a type of arrhythmia. The patient experiences periodic attacks of heart rate ranging from 140 beats per minute. The pulse can rise to more than 200 beats per minute, which poses a danger to human life. The normal sinus rhythm of the heart muscle increases due to the appearance of ectopic impulses in the ventricles and atria.
The duration of the attack may vary, and the onset and end may be sudden and unpredictable. The disease can manifest itself in both adults and children.
Paroxysmal tachycardia has several varieties. Types of disease are divided into the following categories:
- form of the disease (chronic, acute, recurrent);
- according to the location of the attack (atrial, atrioventricular, ventricular, supraventricular);
- according to the degree of development (ectopic or focal, multifocal, reciprocal).
What is paroxysmal tachycardia?
As a rule, attacks of paroxysmal tachycardia begin and end suddenly and have different durations.
They make the heart work uneconomically, reduce the efficiency of blood circulation, and lead to its failure. According to the mechanism of development and etiology, paroxysmal tachycardia resembles extrasystole. Therefore, cardiologists regard successive extrasystoles as a short attack of tachycardia.
Classification of paroxysmal tachycardia
1. Based on the location of ectopic impulses, doctors distinguish:
- atrial paroxysmal tachycardia;
- atrioventricular (atrioventricular) paroxysmal tachycardia;
- ventricular paroxysmal tachycardia.
In turn, atrioventricular and atrial tachycardia are combined into a supraventricular or supraventricular form.
2. Taking into account the nature of the course, the following types of paroxysmal tachycardia are distinguished:
- chronic (constantly recurrent);
- spicy;
- continuously relapsing (lasts for years, can cause circulatory failure and dilated, arrhythmogenic cardiomyopathy).
3. According to the characteristics of the development mechanism, paroxysmal supraventricular tachycardia is classified into:
- focal (ectopic);
- reciprocal (associated with the re-entry mechanism in the sinus node);
- multifocal (multifocal).
In children, paroxysmal tachycardia manifests itself in the same way as in adults.
Supraventricular tachycardia
The forms of cardiac arrhythmia differ in the location of the pathology and the characteristics of its course. Supraventricular tachycardia is a fairly common type of increased heart rate.
What is supraventricular tachycardia?
Supraventricular tachycardia is a form of increased heart rate in which the source of pathological influence is located in the upper part of the myocardium. This is also a form of paroxysmal tachycardia. As a rule, with this disease, a disorder occurs in the sinus or atrioventricular node.
Normally, the heart rate is regulated by the sinus node and ranges from 60 to 100 beats per minute. It is the sinus node that sets the basic parameters of the heart rhythm, including the sequence and speed of contractions. An electrical impulse that autonomously arises in the atypical muscle cells of the sinus node passively spreads along the muscular lining of the heart through conductive structures. If a conduction site is damaged, the patient may develop tachycardia.
Classification of pathology:
- Atrioventricular tachycardia. The area where the electrical impulse closes is located in the atrioventricular node.
- Ectopic atrial tachycardia. The site of pathology is located in the sinus node.
- Multifocal atrial tachycardia – several sources of pathological rhythm.
- Atrial fibrillation is chaotic and intermittent contraction of the atria.
- Atrial flutter is a weak, intermittent contraction of the atria.
8
24/7
Attacks of supraventricular tachycardia usually appear only occasionally and do not significantly affect the patient’s quality of life. Many people with this anomaly do not even notice the manifestations of tachycardia. However, in some cases, supraventricular tachycardia can cause dangerous complications.
Reasons for development
Unlike sinus tachycardia, the supraventricular form of rhythm disturbance is never associated with the physiological needs of the body. In most cases, the disease is caused by an organic or functional disorder of the supraventricular part of the myocardial pathways. This may be an area of electrical impulse cycling, causing the depolarization wave to continually return. In some cases, the condition also occurs due to lack of sleep, low physical activity and anxiety.
Main reasons:
- Various types of myocardial damage: heart attack, viral or bacterial infection, dystrophy, sclerosis, trauma.
- Heart failure.
- Impaired blood supply to the heart.
- A disease of the thyroid gland that leads to a significant release of hormones (hyperthyroidism).
- Chronic lung diseases.
- Smoking and alcoholism.
- Drinking large amounts of caffeine.
- Taking drugs, including cocaine and methamphetamine.
- Side effects of asthma, cold and allergy medications.
- Consequences of cardiac surgery.
- Wolff-Parkinson-White syndrome.
Also, some risk factors can increase the likelihood of developing the disease. These include:
- Age. Some types of supraventricular tachycardia are more common in young people.
- Diseases of the coronary arteries.
- Congenital heart defect.
- Diabetes.
- Anxiety and panic attacks.
- Increased physical activity.
- Obstructive sleep apnea (temporary breathing disorder).
Combining risk factors with heart disease significantly increases the risk of developing the disease.
Symptoms and signs
Doctors often point out that supraventricular tachycardia, the symptoms and treatment of which depend on the severity and type of pathology, may have a different clinical picture. Due to the episodic nature of the disease, many patients do not notice signs of tachycardia and have no complaints. Typical symptoms develop in the chronic form of the disorder.
Frequent symptoms and signs of supraventricular tachycardia:
- Feeling of fluttering in the chest.
- Feeling of rapid heartbeat.
- Hesitant breathing.
- Dizziness and loss of consciousness (rare).
- Increased sweating.
- Chest pain.
In infants and preschool children, signs and symptoms can be difficult to identify. Parents are advised to pay attention to sweating, refusal to eat, pale skin and measure the pulse rate. If the heart rate exceeds 200 beats per minute, then most likely the child has supraventricular tachycardia.
Not all forms of supraventricular tachycardia resolve quickly. The patient may experience increased heart rate from several minutes to several hours. Possible complications depend on the duration of the course, since with frequent contractions the ventricles do not have time to fill with blood, and a lack of blood supply occurs. Sometimes hypotension also develops.
Diagnostics
You can detect tachycardia yourself at home. If discomfort occurs, you need to place two fingers on the area of the radial artery just below the wrist and, after detecting the pulse, count the number of beats per minute. If the heart rate exceeds 100 beats in the absence of stress and physical activity, but most likely we are talking about pathological tachycardia. However, this method does not indicate the type of disease and the source of the pathological influence, so you must consult a doctor.
During the consultation, the doctor will question the patient about complaints, study the medical history and conduct a physical examination. Cardiac auscultation and tonometry will help identify signs of the disease only during an attack, so in most cases additional research methods will be required.
Instrumental diagnostic methods:
- Electrocardiography is the study of the electrical activity of the myocardium. The doctor examines the resulting cardiography and detects any signs of disturbances in the rhythm, speed and sequence of heart contractions. Supraventricular tachycardia on the ECG may have typical signs.
- Holter test – recording of a cardiogram during the day using a portable device attached to the patient’s body. The patient is required to keep a diary and indicate the time of occurrence of unpleasant sensations in the heart, so that the doctor can study the desired section of the cardiogram.
- Echocardiography is a method of scanning the heart, with which you can obtain an image of the organ and evaluate its functional state.
- Stress test is a method of recording a cardiogram during physical activity. Helps identify episodic supraventricular tachycardia. The results also depend on the patient’s fitness level.
- X-ray, magnetic resonance and computed tomography are methods of visualizing organs that make it possible to detect the source of organic damage. Supraventricular tachycardia may be associated with damage to certain areas of the myocardium.
A variety of diagnostic methods makes it possible to detect even an asymptomatic and rarely manifested form of tachycardia. Some experts believe that supraventricular tachycardia, the symptoms of which do not affect the patient’s health, can be considered a variant of the physiological norm.
Treatment and prognosis
Most patients with supraventricular tachycardia do not require special treatment. However, if prolonged and frequent episodes of increased heart rate develop, doctors may prescribe the following treatment methods:
- Therapeutic massage to stimulate the vagus nerve. This nerve is responsible for the functional activity of the parasympathetic system and slows the heartbeat, which can be useful during an attack of tachycardia. The massage technique involves applying gentle pressure to the neck in the area of the carotid sinus. It is recommended to entrust the massage to a specialist.
- Physical exercises to reduce the frequency of contractions during an attack.
- Cardioversion is a method of applying current to the myocardium, aimed at normalizing the rhythm of cardiac activity. This is an emergency procedure required for severe tachycardia.
- Antiarrhythmic drugs for symptomatic treatment.
- Radiofrequency removal of the source of pathological rhythm using catheterization.
In rare cases, this disease requires the introduction of a pacemaker to permanently correct the heart rhythm. This device will sit under the skin near the collarbone and provide electrical signals in the event of a seizure.
It is important for patients to know that supraventricular tachycardia, for which help may be limited to massage, is not a dangerous disease. In the absence of additional heart diseases, the prognosis is favorable.
Prevention
Cardiologists believe that supraventricular tachycardia, which does not always require treatment, can be prevented by fairly simple preventive measures. The most useful methods include:
- Correct selection of therapeutic diet.
- Increase physical activity.
- Quitting smoking, alcohol and caffeine.
- Maintaining a healthy body mass index.
- Reducing stress.
- Regular diagnostics of the cardiovascular system.
- Treatment of precursor diseases of tachycardia.
- Use of sedatives in the presence of severe anxiety and panic attacks.
If supraventricular tachycardia has already been diagnosed, it is recommended to follow the doctor's instructions and take medications on time. Regular massage is also an excellent means of preventing attacks of supraventricular tachycardia.
8
24/7
Causes of paroxysmal tachycardia
Supraventricular paroxysmal tachycardia occurs as a result of increased activation of the sympathetic nervous system. Ventricular is a consequence of necrotic, inflammatory, sclerotic or dystrophic damage to the heart muscle.
In the ventricular form, the focus of ectopic excitation is located in the His bundle, its legs and Purkinje fibers, that is, in the ventricular sections of the conductive nervous system. Most often, the pathology is diagnosed in elderly men who have suffered a myocardial infarction, coronary heart disease, or suffer from hypertension, myocarditis, or heart defects.
The main causes of the development of paroxysmal tachycardia also include:
1. The presence of additional innate impulse pathways in the myocardium. That is:
- Kent's bundle between the atria and ventricles, bypassing the atrioventricular node;
- Macheim fibers between the atrioventricular node and the ventricles.
2. The presence in the myocardium of additional impulse pathways resulting from myocardial damage (infarction, myocarditis, cardiomyopathy).
3. Additional pathways cause pathological movement of excitation throughout the myocardium.
Cardiology knows cases when longitudinal dissociation appears in the atrioventricular node, causing uncoordinated functioning of the fibers of the atrioventricular connection. Then some of the fibers function normally, while the other, on the contrary, conducts excitation in the retrograde (opposite) direction and acts as the basis for the circular circulation of impulses from the atria to the ventricles and along the opposite fibers back to the atria.
In young children, essential (idiopathic) paroxysmal tachycardia of unknown etiology is sometimes diagnosed.
2. Causes of the disease
The following factors are considered to be the causes of paroxysmal tachycardia:
- endocrine disorders;
- transient oxygen starvation of the heart muscle;
- changes in the concentration of electrolytes in the blood;
- heart defects;
- inflammatory diseases of the heart muscle;
- hypertension;
- hereditary factor;
- psycho-emotional factor.
However, in some patients no obvious causes are identified either before the onset of an attack or during life.
Visit our Cardiology page
Symptoms of paroxysmal tachycardia
An attack of paroxysmal tachycardia always begins and ends suddenly. Its duration can range from several minutes to several days. The patient feels an incomprehensible “push” in the area of the heart. Then the heartbeat increases sharply and reaches 120-220 beats/min. The correct heart rhythm is maintained.
Paroxysm may be accompanied by:
- noise in the head;
- dizziness;
- a feeling of squeezing of the heart.
In some cases, neurological focal symptoms occur - hemiparesis, aphasia.
Paroxysm of supraventricular tachycardia is often manifested by autonomic dysfunction, which is characterized by:
- nausea;
- sweating;
- flatulence;
- low-grade fever.
When the attack ends, polyuria (increased urine production) is observed after a few hours. If paroxysmal tachycardia is prolonged, blood pressure may decrease, severe weakness, and fainting may occur.
If you notice similar symptoms, consult a doctor immediately. It is easier to prevent a disease than to deal with the consequences.
Characteristic manifestations of paroxysmal tachycardia
The attack begins and ends unexpectedly and can last from several minutes to 2 days. The first sign of the disease is felt as a sharp “push” in the heart, and then the pulse quickens to 140-200 beats per minute and remains this way for several minutes or even days.
In addition, the disease is manifested by the following symptoms:
- noise in the ears and head;
- nausea or vomiting;
- dizziness and headaches;
- flatulence;
- feeling as if the heart muscle turns to stone and contracts;
- excessive sweating.
Ventricular tachycardia is manifested by an increase in heart rate up to 180 beats per minute, and supraventricular tachycardia - from 180 to 250 beats per minute.
If the attack lasts for a long time, the patient may experience a drop in blood pressure, fainting, and severe weakness. After its completion, a person may experience excessive urine output.
Diagnosis of paroxysmal tachycardia
Paroxysmal tachycardia is recognized by the typicality of the attack (sudden onset and sudden end) and data obtained from a cardiac examination. The supraventricular and ventricular forms differ in the degree of increase in heart rate:
- with ventricular tachycardia, the heart rate is up to 180 beats/min, tests with excitation of the vagus nerve are negative;
- with supraventricular tachycardia, the heart rate is about 220-250 beats/min, the attack is easily stopped by excitation of the vagus nerve.
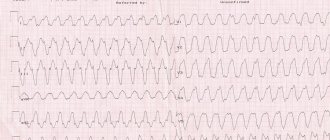
An ECG with paroxysmal tachycardia shows a change in the polarity and shape of the P wave, as well as a violation of its location in relation to the ventricular QRS complex. These signs allow us to judge what form of the disease we are talking about.
Thus, an ECG with atrial paroxysmal tachycardia shows the location of the positive/negative P wave in front of the QRS complex. If the paroxysm comes from the atrioventricular junction, a negative P wave is recorded, located behind/merging with the QRS complex. An ECG with ventricular paroxysmal tachycardia registers expansion and deformation of the QRS complex, and an unchanged P wave can also be recorded.
Paroxysmal tachycardia cannot always be detected using an ECG. Then cardiologists resort to daily ECG monitoring, which allows them to observe short episodes of attacks that are not subjectively felt by the patient.
In order to exclude organic cardiac pathology, the following are additionally carried out:
- MRI;
- Ultrasound of the heart;
- MSCT of the heart (layer-by-layer scanning of cardiac structures).
In some cases, an endocardial electrocardiogram is recorded by inserting electrodes into the heart.
Diagnostics
If paroxysmal tachycardia is suspected, the patient should consult a general practitioner or cardiologist to confirm or refute the diagnosis. The main research method is electrocardiography (ECG). Not all attacks are felt by the patient, so the doctor may prescribe daily
Additionally, the patient may be prescribed the following diagnostic methods:
- magnetic resonance imaging of the heart;
- layer-by-layer scanning of the heart muscle (MSCT);
- Ultrasound diagnostics of the heart.
Treatment of paroxysmal tachycardia
The treatment regimen for paroxysmal tachycardia depends on:
- forms of arrhythmia (ventricular, atrial, atrioventricular);
- reasons that caused the disease;
- duration and frequency of paroxysms;
- presence/absence of complications.
Attacks of paroxysmal tachycardia require emergency hospitalization (with the exception of idiopathic variants with a benign course, which are easily stopped by administering an antiarrhythmic drug to someone).
For the treatment of the supraventricular form, complicated by cardiovascular or heart failure, patients are hospitalized in the cardiology department. Planned hospitalization is carried out if attacks recur more often than 2-3 times a month. Then the question of the relevance of surgical intervention is decided.
Emergency care for paroxysmal tachycardia includes intravenous administration of antiarrhythmic drugs (Propranolol, Aymalin, Rytmodan, Quinidine, Ethmozin, Cordarone, Isoptin, etc.). If the attack is prolonged and cannot be controlled with medications, electropulse therapy is performed. Then the patient undergoes outpatient cardiological treatment, during which effective antiarrhythmic drugs are selected.
To relieve paroxysmal tachycardia, doctors often use vagal maneuvers - techniques that have a pronounced mechanical effect on the vagus nerve. These include:
- straining;
- Aschner's test (moderate and uniform pressure on the inner upper corner of the eyeball);
- Valsalva maneuver (vigorous exhalation with the mouth and nasal cavity closed);
- irritating the root of the tongue to trigger a gag reflex;
- Chermak-Hering test (uniform pressure on the carotid sinuses in the area of the carotid artery).
If attacks of paroxysmal tachycardia occur several times a month, the patient is prescribed long-term anti-relapse therapy:
- quinidine preparations (Disopyramide, Kinylentine, Amiodarone, Verapomil, etc.);
- cardiac glycosides (Celanide, Digoxin).
The selection of an effective dosage is carried out taking into account the patient’s well-being and ECG results.
Surgical treatment of paroxysmal tachycardia is used only if the disease is severe and cannot be controlled with medications. Among the most common surgical methods are:
- mechanical, laser, electrical, cryogenic, chemical destruction of additional impulse pathways or ectopic foci of automatism;
- RFA;
- implantation of a pacemaker;
- implantation of an electrical defibrillator.
If a patient wants to treat paroxysmal tachycardia using traditional methods, he should first consult with a cardiologist, since failure to take prescribed antiarrhythmic drugs can lead to serious complications.
Prevention
Prevention lies in early diagnosis. Often, success directly depends on the patient and his attitude towards his health. Basic recommendations that should be followed during prevention:
- moderate regular physical activity;
- proper nutrition;
- rejection of bad habits;
- avoidance of situations that lead to stress and cause anxiety;
- compliance with the instructions of the attending physician.
The main thing is to diagnose tachycardia in a timely manner in order to move on to prevention in time. You can get acquainted with the programs of our center by following the link.
Diet for paroxysmal tachycardia
Patients with paroxysmal tachycardia should monitor blood sugar and cholesterol levels and maintain normal body weight. It is recommended that they take food in small portions 4-5 times a day. This is explained by the fact that overeating leads to irritation of the nerve receptors that are responsible for the functioning of the heart, and this is fraught with attacks of tachycardia.
You can't eat late at night. The last meal should be no later than 2-3 hours before going to bed. Exclude from the diet:
- coffee Tea;
- products containing large amounts of sugar, starch;
- sweets, baked goods;
- fatty foods (lard, mayonnaise, fatty meat, butter).