Another name for intestinal cancer is colorectal cancer.
It is localized in:
- Sigmoid colon;
- Rectum;
- Ascending colon;
- Descending colon;
- Caecum;
- Transverse colon;
- Appendix;
- Small intestine.
If intestinal cancer is detected in the early stages, the patient needs the following comprehensive therapy:
- Innovative type operations (radical or palliative);
- Chemotherapy;
- Radiation therapy.
There are factors influencing the occurrence of neoplasms in the intestinal area:
- Hereditary: family history of cancer, i.e. genetic predisposition, in which you need to monitor your health and see a doctor.
- Intestinal diseases of various types: the presence of polyps, Crohn's disease, adenomas, ulcerative colitis.
- Poor nutrition: fatty foods, low fiber consumption, foods rich in carbohydrates - all this leads to constipation, which causes damage to the intestinal walls and malignancy of its cells.
- Harmful health habits: the use of nicotine, drugs and alcohol can trigger the degeneration of cells into cancer.
- Polluted environment: Cancer can be caused by substances in the pathogenic atmosphere, such as mercury, asbestos, etc.
The development of intestinal cancer is individual in time and directly depends on the above factors and the state of human health.
Bowel cancer is of the following types:
- Intestinal adenocarcinoma (new glandular formation);
- Intestinal lymphoma (damages of the intestinal walls in the location of fibrous tissue, can release metastases to the liver and bone marrow);
- Intestinal carcinoma (damage to intestinal epithelial cells);
- Intestinal sarcoma (occurs on the anterior intestinal wall, pathology grows from connective tissue);
- Intestinal melanoma (cancer formed from melanocytes found in the skin).
Cancer can arise from a benign tumor - an adenoma, which, in turn, arises due to chronic colitis, gastritis and ulcers.
There are four stages of bowel cancer. In the first two stages, symptoms are almost invisible. In the later stages, symptoms are already noticeable, but curing this cancer is much more difficult.
Quarter stage
With her
- Intestinal perforation occurs;
- Possible intestinal bleeding;
- Intestinal obstruction;
- The appearance of a large number of metastases;
- Severe intoxication.
There are many manifestations of bowel cancer. The most common ones are:
- Blood in stool;
- I have a stomachache;
- Digestion is upset.
At an early stage, symptoms are as follows:
- Chronic fatigue;
- Mucus in the stool, blood in the stool (blood in the form of streaks, then in clots);
- Frequent urge to go to the toilet to have a bowel movement;
- Tachycardia;
- Decreased hemoglobin and red blood cells.
At a later stage, the symptoms are much brighter:
Chondrosarcoma
- Intestinal obstruction: gases and feces stop coming out on their own, the intestines become swollen;
- Acute stomach.
Also, symptoms directly depend on the type of intestinal cancer. With adenocarcinoma, symptoms include pain in the large intestine, constipation, fever, and general fatigue.
With carcinoma, the symptoms manifest themselves in the form of a feeling of pain and distension in the abdomen, constipation is replaced by diarrhea, there is mucus and blood in the stool, and the patient’s appetite is poor.
With lymphoma, symptoms include nausea, lack of appetite, fatigue, periodic bloating, gas formation, anemia, and fever.
With sarcoma, the symptoms are manifested by upset stool, heartburn, blood in the stool, painful bowel movements, pain in the lower abdomen, pain when moving, and eating.
Let's consider what signs of cancer are observed in women and men.
Prevention and diagnostic methods for colon cancer
Colon cancer is preventable. The most important step in preventing colon cancer is screening. Any abnormal screening test result should be followed by a colonoscopy. Some doctors prefer to begin their investigations by performing a colonoscopy as a screening test.
Colonoscopy is a detailed examination of the intestinal lumen and walls of the colon. During a colonoscopy, it is possible to detect and remove polyps of the colon and rectum. There is anecdotal evidence that diet has a significant effect in preventing the development of colorectal cancer. It is generally accepted that high fiber and low fat are dietary measures that can prevent the development of colorectal cancer.
Finally, pay attention to your gut health and function. Any changes in bowel habits, such as constipation, diarrhea, or traces of blood in the stool should be discussed with a coloproctologist.
Among women
Most often, colon cancer occurs in women. Cancer usually appears after the age of forty, as the body prepares for menopause. Very often, cancer arises from the degeneration of polyps. Hereditary predisposition and poor nutrition play a very important role here.
The main symptoms appear after two years. Usually these are abdominal pain, problems with stool, and bloating. When metastasis occurs, the lymph nodes, vagina, and other pelvic organs are affected. In the later stages, the pain intensifies, intestinal incontinence occurs, the patient vomits, the composition of his urine changes, the kidneys are affected, urogenital fistulas occur, and the menstrual cycle may change.
Colon tumors
Types of tumors
Tumors of the large intestine are divided into benign and malignant, as well as tumors of epithelial and non-epithelial origin. According to the international morphological classification, the following neoplasms are distinguished:
- Epithelial tumors of the intestine
: tubular adenoma, villous adenoma, tubular-villous adenoma, adenomatosis. Epithelial tumors are the most common, they make up about 92% of all neoplasms, and have a high tendency to malignant degeneration. - Non-epithelial intestinal tumors
: lipoma, leiomyoma, leiomyosarcoma, angiosarcoma and Kaposi's sarcoma.
Also among benign processes, tumor-like lesions of the colon (hamartomas) are distinguished: Peutz-Jeghers polyp, juvenile polyp. Among tumors of the large intestine, there are heterotopias: hyperplastic or metaplastic polyp, benign lymphoid, inflammatory and deep cystic polyp. According to their prevalence, there are single, multiple (grouped and scattered) polyps, and diffuse polyposis.
Malignant tumors of the large intestine are divided into four types based on their growth patterns:
- exophytic polypoid tumors
that grow into the intestinal lumen; - endophytic-ulcerative tumors
, spreading in the intestinal wall, often give ulcerations; - diffuse infiltrative tumors
(malignant cells have a diffuse distribution within the walls of the organ); - Annular tumors
grow around the circumference of the intestine.
In the last two cases, the histological boundaries of the tumor process are difficult to determine; cells can penetrate into areas that at first glance look healthy.
Tumor staging
When classifying malignant tumors of the large intestine, the stage of the process is of great importance. Staging is determined using the internationally accepted TNM classification, where T is the degree of tumor growth in the tissue, N is the presence or absence of metastasis to regional lymph nodes, M is distant metastasis.
- T0
– no signs of tumor growth - Tx
– reliable assessment of the primary tumor is impossible - Tis
– carcinoma in situ, or cancer “in place”, does not invade the mucosa - T1
– tumor spread to the submucosal layer - T2
– tumor invasion of the muscle layer - T3
– tumor spread to the muscle layer and penetration into the tissues around the large intestine that are not covered by the peritoneum. - T4
– tumor has invaded the visceral peritoneum or spread to organs and tissues located nearby.
Nx – it is impossible to assess the condition of regional lymph nodes. N0 – there are no metastases in regional lymph nodes. N1 – metastases in 1-3 lymph nodes located around the large intestine. N2 – metastases in four or more lymph nodes located around the large intestine. N3 – metastases in the lymph nodes that are located along the vessels. Mx – distant metastases cannot be determined. M0 – no metastases. M1 – there are metastases in distant organs.
According to the TNM classification, there are four stages of colon cancer. The zero stage is TisN0M0. The first stage is T1N0M0 or T2N0M0. The second stage is T3N0M or T4N0M0. The third stage is any T and N1M0 indicators, any T and N2M0 indicators, or any T and N3M0 indicators. The fourth stage is any indicators of T and N, M1.
Along with this classification, many European countries and North American countries use the classification of tumors by S. E. Dukes, proposed back in 1932. Colon tumors are also divided into four stages, designated by Latin letters. Stage A - the tumor process spreads within the mucous and submucosal layer (T1N0M0 and T2N0M0). Stage B – the tumor grows into all layers of the intestinal wall (T3N0M and T4N0M0). Stage C - the tumor can be of any size, but there are metastases to regional lymph nodes. Stage D – there are distant metastases.
In men
Men usually get colorectal cancer. Its symptoms are as follows:
- Anus hurts;
- Diarrhea and constipation;
- Blood or mucus appears in the stool.
If the process of metastasis has begun, the prostate may be affected.
The neoplasm can be palpated by a proctologist.
Cancer in men can develop due to the use of harmful substances, poor diet, the presence of intestinal polyps, ulcers, colitis, hemorrhoids, and excess weight.
The first organ in which metastases develop in this type of cancer is the liver. The process occurs at the last stage of the disease. With proper treatment, a patient with this diagnosis can live up to two years.
Metastasis can also occur in the pelvic organs, peritoneum, pancreas, lungs, retroperitoneal space, and bladder.
The processes of metastasis are as follows:
- Initially, the tumor grows into the fatty tissue;
- Perforation of the colon;
- Cancer cells are found in neighboring organs.
First, the rectum is examined by palpation.
Next, colonoscopy and sigmoidoscopy are performed. During the latter, the doctor examines the rectal mucosa. Sections of the sigmoid colon can be examined.
During endoscopy, the surgeon performs a biopsy, followed by a histological examination.
To diagnose colon cancer in the early stages, protein levels are determined. Thanks to these tumor markers, bowel cancer can be detected in the absence of symptoms.
Treatment
Comprehensive treatment is recommended: surgery, chemotherapy, radiation therapy, radiotherapy.
Who is at risk?
Although colorectal cancer can occur at any age, more than 90% of patients develop cancer over the age of 40, with the risk of developing the disease doubling every 10 years. In addition to age, risk factors include a family history of colorectal cancer, polyps and ulcerative colitis, as well as colon polyps and cancers of other sites, especially the breast and uterus.
What is colon cancer?
Colon cancer is formed from the mucous membrane and is malignant in nature. Adenocarcinoma is more common, squamous cell carcinoma is less common.
In most cases, a malignant neoplasm is formed as a result of the transformation of polyps that have arisen in the colon. Thus, timely removal of polyps reduces the likelihood of developing cancer and is a surgical prevention of cancer.
A colon tumor forms in one of its sections:
- Cecum
- Ascending colon
- Transverse colon
- Descending colon
- Sigmoid colon
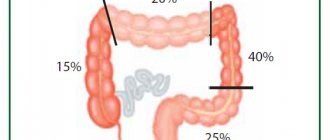
Despite the possibility of cancer forming in any part of the colon, the incidence of lesions in each area varies significantly. Thus, in 50% of cases, the tumor affects the sigmoid colon, more than 20% occurs in the cecum, 10% in the transverse colon, and about 15% in areas of the physiological bends of the intestine. And only in 2% of cases, cancer initially affects several parts of the colon.
Risk factors
- The likelihood of detecting a tumor in yourself increases if the medical history of relatives already includes colon polyposis;
- Unbalanced diet: satiety with fatty foods, lack of vegetable and fruit components, legumes, whole grain bread, buckwheat and corn in daily dishes;
- Frequent constipation, especially those that were eliminated after the use of laxatives that irritate the mucous surface of the intestinal layer;
- Crohn's disease - inflammation of the colon mucosa with the appearance of numerous ulcers, diarrhea is much more pronounced than with ulcerative colitis, the presence of perianal lesions in the form of polyps and fistulas (inflammation in the recess of the anal mucosa, perirectal tissue or intersphincteric space);
- Hypodynamia - weakened motor tone;
- Age limit: over 50 years;
- Angiodysplasias are congenital malformations of blood vessels;
- Smoking;
- Nonspecific ulcerative colitis (UC) is a chronic diffuse inflammatory process of the mucous layer of the rectum and colon, which serves as an impetus for the formation of various ulcers of the mucous membrane.
Fact. The total length of the colon is approximately one and a half to two meters.
Question answer
How much does the food we eat affect the formation of tumors?
Yes, the risk of developing tumors increases if you have food in your daily diet that is low in fiber, but rich in animal proteins and fats. In this situation, a person may experience frequent constipation, and an imbalance of intestinal flora is likely. The content of bile acids and carcinogenic phenols increases in the intestines. And this harms the mucous membrane. Smoked foods and preservatives also cause harm. They also contain predominant carcinogens. Fact. A person is able to eat food even when placed upside down, since special peristalsis muscles “turn on” in time. This explains why astronauts eat in a weightless state.
Can anal sphincter insufficiency predict the appearance of a colon tumor?
Mostly no. Colon incontinence is associated primarily with obstetric trauma and muscle dysfunction as a result of nervous disorders. This is also a reaction to various inflammatory diseases, to prolapse of hemorrhoids or the rectum itself.
Is it possible to perform sphincter-sparing surgery for familial adenomatosis (a hereditary disease that is accompanied by the formation of many polyps on the mucous membrane) of the colon?
If the polyps have not progressed to the stage of cancer, then the probability remains approximately 85%. If the polyps have become malignant, then this kind of sparing surgery is permissible only in 30% of cases of the total number of cases. But removal of polyps in the affected parts of the intestine is mandatory, since cancer appears from them one way or another.
Diagnosis based on cell structure - the near future
— You have a super-technological specialty, have new techniques appeared lately that have amazed you?
— We work beyond human perception, the equipment allows us to see more than our eyes. Endoscopic classification - what type of polyp is and whether it can be removed - is based on the structure of the tissue glands and microvascular capillary bed, which are not visible to the human eye. Now there are endoscopes that work on the principle of microscopes. Endoscopic devices that magnify the image a thousandfold should soon appear in Russia. With their help, we will be able to make diagnoses based on the structure of the cell. Essentially, this is intravital microscopy.
— It is believed that endoscopists are second only to resuscitators at the risk of contracting Covid. How are you working during the COVID-19 epidemic?
— Those doctors who perform bronchoscopy are at greatest risk. Colonoscopy and gastroscopy also have risks for personnel, but they are many times lower compared to bronchoscopy. But in our department, everyone has already recovered from Covid, and everyone has already been vaccinated, while we continue to comply with the recommended sanitary and epidemiological regime.
Department of Endoscopy, National Medical Research Center of Oncology named after. N.N. Petrova specializes in the diagnosis and treatment of malignant neoplasms and precancerous diseases of the gastrointestinal tract, as well as tumor pathologies of the trachea and bronchi. Every year the department carries out 4,000 diagnostic endoscopic examinations and about 1,000 treatment procedures. This is a highly specialized scientific and clinical unit of the center. The department is the base of the Department of Endoscopy of the Northwestern Medical University. I.I. Mechnikov and the Department of Oncology of St. Petersburg State Medical University named after. acad. I.P. Pavlova.