Frontal hyperostosis is a rare pathology, but sometimes it is dangerous for the patient. Due to its low prevalence, it has not been studied enough, so there are not many serious studies in this area. In ICD-10, the disease is defined as No. M85 along with other disorders of bone density.
The very concept of “hyperostosis” means bone growth of a pathological nature. It is often accompanied by tumor processes and serious hormonal disorders. Hyperostosis also occurs as a consequence of malignant neoplasms.
General information
Hyperostosis is a pathologically increased content of unchanged bone substance (from the Greek hyper - over, osteo - bone), which can be a response to certain intoxications , poisoning , physical overload, exposure to radiation, cancer formation , hypervitaminosis of vitamin A and endocrinopathies, obesity , arterial hypertension , chronic infections, and is also a manifestation of osteomyelitis . It is quite rare and formally resembles spondylosis .
The disease is assigned the ICD-10 code: M48.1 Ankylosing Forestier hyperostosis or diffuse idiopathic skeletal hyperostosis. Hyperostosis can affect the entire musculoskeletal system (generalized), several bones, or just one (local). Forestier's disease is a striking example of local hyperostosis and is a degenerative-dystrophic lesion of the spine in the form of ossification and thickening of the longitudinal ligament along the cervical and thoracic spine. The disease is more common in people 55–60 years of age and older.
Local hyperostosis also includes:
- damage and increase in size of the skull bones, most often the facial bones ( craniosclerosis );
- proliferation of bone tissue that has not undergone pathological changes within the diaphyses in tubular bones;
- Morgagni-Morel-Steward syndrome is characteristic of older women and affects the internal plate of the frontal bone.
What is hyperostosis of the frontal bone?
It is very important to promptly recognize and understand what hyperostosis of the frontal bone is. It usually develops in the setting of virilism , obesity , amenorrhea , or other neuroendocrine and reproductive disorders. However, recent studies have shown that Morgagni syndrome was also identified in men, and it was a hyperostosis of the inner plate of the frontal bone.
In women, the underlying mechanism for the development of pathology is an increase in the concentration of male sex hormones above normal. This manifests itself in the form of a tendency for fat deposition in the abdominal area, a deepening of the voice, increased muscle growth, and the appearance of a beard and mustache. Changes occur gradually, cause pain and discomfort, provoke weight gain, irritability and sleep disturbances, and can even cause depression .
What is craniostenosis in children?
First of all, it depends on whether the child has other developmental defects. Sometimes pathology accompanies various syndromes - then it is called syndromic. For example, it can occur simultaneously with fusion of fingers or toes, cleft palate or lip, or cerebral hernia.
If fusion of the sutures in the bones of the skull occurs without other developmental defects, it is considered non-syndromic, that is, independent.
Doctors classify the disease into types based on which cranial sutures are fused:
- metopic,
- lambdoid,
- coronary,
- sagittal.
Synostosis - or suture fusion - can involve one to several sutures. There is a concept of pansynostosis - complete overgrowth of all seams. This type of pathology can be considered the most severe; it is less common than others.
Pathogenesis
The main manifestation of Forestier hyperostosis is ossification (extraskeletal formation of bone tissue in atypical places) of the anterior longitudinal ligament along the cervical and thoracic spine.
The pathology develops as a result of an autoimmune nonspecific inflammatory process, which leads to diffuse idiopathic changes in the skeleton in the form of replacement of the end structures of the nodes with cartilage and then with bone tissue.
Ligaments of the spinal column
Typically, the ossification process affects the ligamentous apparatus, while bone growths can form in the anterolateral sections - the so-called hyperostotic strata, non-connecting “bridges” and “spurs” of the spine, bypassing the intervertebral discs. As a result, the mobility of the vertebrae suffers, which leads to ankylosis (in some cases to complete immobilization) and, as a consequence, to muscle atrophy.
The disease is characterized by a long course, with no disturbances in the structure of internal organs, joints or the height of the vertebrae.
Cephalohematoma
Cephalohematoma is not quite an anomaly of the skull, but a pathological local deformation of the skull that occurs in the postnatal period due to trauma and the use of forceps during childbirth, in which hemorrhage occurs between the inner and outer plates of the diploe. If this hematoma is not evacuated in childhood, it will persist throughout life, and cloud-like calcifications can be found in its stoma.
Fig. 14 Cephalohematoma
Causes
The initiating factors for the development of hyperostosis are considered to be:
- neuroendocrine disorders;
- frequent intoxication;
- age-related changes in connective tissue;
- chronic infectious diseases.
Causes of Forestier's disease
Pain syndrome and ankylosis can be observed in people after 45-50 years of age, and most often such changes were observed in their parents. It is believed that genetic factors are of greatest importance in the development of pathology. Studies have shown that a third of patients had the following antigen: human leucocyte antigen - HLA B27 , the gene of which is responsible for bone formation.
Why is craniostenosis dangerous?
The absence of movable sutures in the skull severely limits the brain. Therefore, the sooner help comes for craniostenosis, the higher the likelihood of a complete cure for the child in the future. Compensation mechanisms in infants under 2 years of age are very high, but rehabilitation after this age turns out to be more complex and lengthy. If not treated promptly, the disease can cause the following conditions:
If you do not receive treatment in a timely manner, the disease can cause the following conditions:
- delayed physical, mental, intellectual development;
- disruption of normal brain functions;
- skeletal underdevelopment;
- compression and atrophy of the optic nerve up to complete loss of vision;
- headache;
- ophthalmological diseases;
- death.
Symptoms
The clinical manifestation of Forestier's disease is only a limitation of the range of motion in the affected part of the spine. In extremely rare cases, patients may experience symptoms such as:
- slight or moderate pain in the thoracic spine;
- smoothing the physiological curves of the spinal column;
- changes in posture in the form of stooping or the development of a pronounced “supplicant pose”;
- dysphagia (more typical for more severe stages of significant ossification of the structures of the cervical spine);
- amyotrophy;
- with ossification of other ligaments, pain may occur in the places of their attachment, including the area of the calcaneus, the process of the ulna, the hip joint, the ischial tubercle, and the patellas.
The disease is much more severe with ossification of the posterior longitudinal ligament (“posterior” Forestier). Its thickening leads to progressive spinal stenosis, compression of the spinal cord, myelopathy and severe neurological disorders.
Deformities of the cranio-vertebral region
Fig. 1 General diagram of anomalies in the forms of the craniovertebral junction (Koval G.Yu. General issues of X-ray diagnosis of diseases of the skull)
Fig. 2 Basilar impression (Fig. 2a). Sagging of the squama of the occipital bone (Fig. 2c). Convexobasia (Fig. 2b).
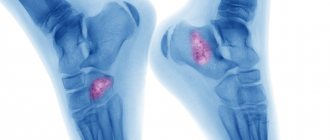
Tests and diagnostics
Despite the level of development of modern medicine, it is quite difficult to recognize hyperostosis after studying the clinical picture. X-ray examination becomes the most revealing, and tomography is used to accurately determine the localization of the pathological process within the bone structure. In some cases, additional radionuclide testing may be required.
Cervical spine with Forestier hyperostosis
Forestier's disease on an x-ray is characterized by the presence of thickening of the anterior longitudinal ligament and its fusion with the ventral surfaces of the vertebral bodies, but the height of the intervertebral spaces is not reduced. Laboratory values sometimes reveal hyperglycemia .
When making a differential diagnosis with other pathologies that deform the spine, take into account the absence of laboratory signs, manifestations of inflammatory activity, sacroiliitis , ankylosis of intervertebral joints , and narrowing of intervertebral discs.
Normal formation of cranial sutures
After 3 years, throughout the entire length, the width of the lumen of the seam does not exceed 0.5-1.0 mm. In adults, the lumen of the suture looks like a thin hairline and cannot be measured. Starting from the 2nd year of life, the lumen clearly competed, and from 4-8 years an intense stripe appears along its edge - the so-called zone of physiological sclerosis (Fig. 10a and Fig. 10b).
Fig. 10 Cranial sutures of a 2-year-old child (Fig. 10a), cranial sutures of a 9-year-old child (Fig. 10b), craniostenosis in a 4-year-old child (Fig. 10c).
Diet for Forestier hyperostosis
Hypocaloric diet
- Efficiency: 3-6 kg in 30 days
- Terms: 14-30 days
- Cost of products: 1500-1600 rubles. in Week
The fundamental factor in improving the condition of patients with hyperostosis is weight normalization, which can be achieved through a lifelong diet. Most often, a hypocaloric diet is prescribed, which can reduce the number of calories consumed, but at the same time provide the body with all the necessary substances and vitamins. It is recommended to add more to your diet:
- fresh vegetable and fruit salads;
- light soups;
- flour products made from whole grain or wholemeal flour;
- porridge;
- seafood;
- teas and compotes.
It is advisable to completely eliminate alcohol, flour, sweets, fried and fatty foods, as well as harmful foods such as smoked meats, canned food, semi-finished products, fast food, etc.
Variants of normal skull shapes
Fig. 3 General diagram of normal variants of skull shapes (Koroluk I.P. “X-ray anatomical atlas of the skeleton”).
Mesocephalic skull (Mesocrane) is the normal anatomical shape of the skull, the average statistically encountered shape is the standard shape of the skull.
Dolichocephalic skull (Dolichocephalic) - a significant predominance of the anteroposterior size (A) of the skull over the frontal size (B).
Fig. 4 Dolichocephalic skull (Dolichocephalus)
Brachycephalic skull - an increased value of the frontal dimension (B) of the skull over the anteroposterior dimension (A).
Fig.5 Brachycephalic skull
Acrocephaly (Acrocephalus) is the predominance of the vertical size of the skull over the anteroposterior and frontal.
Fig.6 Acrocephaly
Bibliography
- Koval G. Yu., Danilenko G. S. “X-ray diagnosis of diseases and injuries of the skull.
- Esinskaya G.N. “A short guide to neuroradiology”, Medicine Publishing House, 1965.
- I.P. Korolyuk, “X-ray anatomical atlas of the skeleton (norm, options, interpretation errors)”, Moscow publishing house “VIDAR” 1996.
Author: radiologist, Ph.D. Vlasov Evgeniy Alexandrovich
Full or partial reprint of this article is permitted by installing an active hyperlink to the source
If you still have doubts about the conclusions of your MRI, you can order a review of your study with a detailed transcript here: