fibular
and the tibia are the long bones of the lower leg. The fibula is small and located on the outside of the lower leg. The tibia is a bone located on the inside of the lower leg.
The fibula and tibia meet at the knee and ankle joints. Two bones help stabilize and support the ankle and foot.
A fracture of the fibula occurs when a fall from a height or any blow to the outer surface of the lower leg. Even a sprained ankle can lead to a fracture of the fibula. A fracture of the fibula can occur at any point.
Photo: Medscape Reference
Types of Fibula Fracture
Types of fibula fracture include:
- Lateral malleolar fibular fracture - occurs when the fibula breaks at the ankle joint;
- Fracture of the proximal head of the fibula - localized at the upper end of the fibula in the area of the knee joint;
- Avulsion fracture - a fracture in which the tendon tears off part of the bone from the side of its attachment;
- Stress fractures occur as a result of repetitive trauma while running or walking;
- Fibula fractures are common in athletes, especially those who participate in running, jumping, soccer, and basketball.
Causes of injury
Let us first consider the mechanism of injury to the medial collateral ligament. As already mentioned, she gets injured quite often. The situation in which this occurs is a blow just below the knee from the outside of the shin. In this case, the leg is usually in an extended position and is more susceptible to injury (happens more often in football players). Otherwise, this can happen during falls, when the lower leg is fixed, and the body moves relative to it to the side with torsion on the leg (injuries of skiers and snowboarders). When the external collateral ligamentous fibers are torn, on the contrary, the blow should fall on the inner surface of the lower leg, and also excessive extension of the knee or internal rotation of the body on the supporting leg should occur.
Diagnosis of fibula fracture
People with a leg injury should see a doctor for a diagnosis. During the diagnostic process the following is carried out:
- Physical examination
- the doctor will look for any noticeable deformities; - X-ray
- used to detect a fracture or displacement of a bone; - Magnetic resonance imaging
(
MRI
) - provides a more detailed scan and can produce detailed pictures of internal bones and soft tissues; - Computed tomography
(
CT
) and other tests may be performed to make an accurate diagnosis and assess the severity of a fibular fracture.
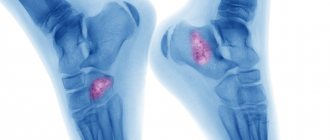
Osteochondroma of the lower (distal) tibia
In a healthy ankle joint, the distal anterior portion of the tibia is round in shape. The neck of the talus, in contact with it, has a groove. When the joint is excessively extended, the anterior edge of the tibia receives microtrauma due to friction against the groove, which can cause the formation of osteochondral exostosis in this area. Moreover, the growth can form both on the anterior lower border of the tibia and in the groove of the talus itself.
Much less often, osteochondromas are observed in the distal part of the fibula, i.e., in the ankle or ankle area. They are usually the result of a direct blow or sprain to the ankle.
When the ankle joint is affected and the exostosis reaches a large size, it can become visible to the naked eye and look like a dense lump. You may also experience:
Pain with strong ankle extension;
· swelling of soft tissues;
· pain on palpation, increasing with hyperextension of the foot;
· limited mobility, which is especially acute for athletes, as their ability to run decreases.
Exostosis of the tibia can provoke the development of inflammatory processes in the ankle joint. In this case, the first symptoms may be manifestations of tenosynovitis and synovitis, i.e. inflammation of the tendons, ligaments and synovial membrane. This is manifested by pain in the ankle, aggravated by movement, a local increase in temperature, and swelling of the soft tissues.
Open fracture of the fibula (compound fracture)
In an open fracture, part of the bone passes through the skin and comes out. Open fractures are often the result of severe trauma or a direct blow, such as a fall or auto accident. This type of fracture is often accompanied by additional injuries. Some injuries can be potentially life-threatening.
Open fibula fractures should be treated immediately. Patients are given antibiotics to prevent infection. The wound is thoroughly cleaned and internal fixation with a plate and screws is used to stabilize the fracture. A bone graft is used to speed up healing.
Treatment of collateral ligament ruptures
Treatment of isolated deformities of the external and internal ligaments is usually carried out using conservative methods. Here it is important to provide fixation to the joint in the first time after injury by using an orthosis. It is better to avoid stress. A course of nonsteroidal anti-inflammatory drugs will relieve inflammation and relieve pain. For rapid regeneration, injections of platelet-rich plasma are used. The rehabilitation period is aimed at gradually increasing the load with strengthening the muscles and without additional injury to the lateral ligaments. Kinesiotherapy, mechanotherapy, taping and physiotherapeutic procedures are used.
Arthroscopy for ligament rupture
It happens, especially with extensive damage, that after the injury instability occurs, which worries during exercise (for athletes and other patients with an active lifestyle). In such cases, reconstruction is performed surgically. Arthroscopy is the most gentle type of surgery. In addition, recovery after it is quick and easy. Sometimes the ligament can be sutured (with fresh partial ruptures); in other cases, fixators are used to the bone if the rupture occurred at the site of attachment of the ligament to it. Another method of reconstruction is ligament plastic surgery using autografts (own tissue). The tendons of the muscles of the popliteal region are used. In the vast majority of cases, the prognosis after such operations is favorable. Patients quickly undergo rehabilitation and return to sports and normal life. When damage to the collateral ligament is combined with injuries to other structures of the knee, their arthroscopic restoration and all necessary surgical procedures are usually carried out in one operation.
Closed fracture (simple fracture)
With a closed fracture, the skin remains intact. The goal of treating closed fractures is to realign the bone fragments, control pain, allow time for the fracture to heal, prevent complications, and restore normal function of the leg. Ice is used to relieve pain and reduce swelling. The leg should be in an elevated position.
If surgery is not required, a brace or cast is used, and crutches are recommended when walking. After fusion, it is necessary to strengthen the weakened joints with the help of physical therapy.
Delayed fracture consolidation - what is it?
What is delayed consolidation of fractures (bone non-union). Most bone fractures heal (consolidate) within 3-6 months. If the fracture has not healed by this time, then doctors talk about delayed consolidation of the fracture or delayed healing of the fracture. Pseudoarthrosis (false joint, non-union fracture) is a complication of a bone fracture when the healing process of the fracture is interrupted. Fibrous or cartilaginous tissue forms between the main fragments of the fracture and therefore, even after 6-8 months, the formation of bone callus and healing of the fracture does not occur.
Prevention of recurrent fibula fracture
To prevent future fibula fractures, athletes should wear appropriate safety equipment.
To reduce the risk of fracture, you must:
- Wear suitable shoes;
- Follow a diet rich in calcium products, such as milk, yogurt, cheese;
- Do exercises to strengthen your bones;
- A fibula fracture usually resolves without further problems, but complications may occur:
- Degenerative or traumatic arthritis;
- Abnormal deformities or dysfunction of the ankle joint;
- Constant pain;
- Damage to the nerve and blood vessels around the ankle joint;
- Chronic swelling of the limb.
Most fibular fractures do not have any serious complications. Within a few weeks to several months, most patients recover completely and can continue their normal activities.
Degrees of ligament damage
Different degrees of damage produce both differences in the clinical picture and require different treatment tactics. Highlight:
- First degree- This is a partial rupture of the surface fibers. Pain occurs at the site of deformation, and swelling is possible.
- The second is damage to most ligamentous fibers. The pain is more widespread, swelling of the joint increases quickly, may be associated with hemarthrosis, and a hematoma occurs on the lateral surface of the joint.
- The third is a complete break. In addition to the above symptoms, joint dysfunction and instability appear.
Anatomy and position relative to other bones
The musculoskeletal system (MSA) in adults is represented by active and passive parts. The active component includes muscles and ligaments. The passive fragment is indicated by a skeleton consisting of bones and their joints. In the adult human body, this part is represented by 208 bones. In order for the human body weight to be correctly redistributed during life, the inside of the bones is hollow. Thanks to this, the weight of the skeleton is less in comparison with the total mass, however, despite this, the structure of the bones is strong, which allows the body to function adequately to the loads applied.
To appreciate the physiological significance of the tibia, it is necessary to understand their topography. The tibia is located in the lower part of the skeleton (leg area), between the thigh and foot, in contact with the tibia. Above, the tibia is limited by the knee joint, below by the ankle. The small bone is connected to the foot through the lateral malleolus through the ankle joint. Large ligaments are located between the shin bones.
According to the length, the fibula is divided into 3 parts: the diaphysis (body) and 2 epiphyses (upper, lower fragment). The body of the bone is bent towards the back and twisted along the axial direction. The diaphysis is represented by a prism and consists of three faces: medial, lateral and posterior. Each face is separated by a ridge. The medial and lateral edges are separated by the anterior protrusion, the inner (medial protrusion) subdivides the medial and posterior sides of the bone, the posterior ridge is located between the posterior and lateral sides.
Read also…. Why does my lower back hurt?
At the back of the MBC there is an opening for the exit of blood vessels and nerves. From this hole, a special canal runs distally into the bone, communicating through holes with canals in other areas of the skeleton. On the inner side between the bones there is a delimiting edge. The upper epiphysis, represented by the head, is in contact with the tibia on its articular side. The apex is pointed. The head is connected to the diaphysis of the fibula through the neck.
One of the most important formations of the fibula is the peculiarity of its topography and interaction with the bones of the foot and leg through the lower epiphysis. The distal part of the bone is often called the lateral malleolus. This ankle can be easily palpated through the skin when the foot is flexed forward.
On the inner side of the lower epiphysis there is an articular side that provides the connection between the talus and the lateral malleolus. Slightly higher in the fibula there is a small roughness that connects to the fibular notch in the tibia. Posteriorly on the fibula there is an ankle groove. The peroneus tendon passes through this depression.
Surgical treatment of patients with pseudarthrosis
Surgical treatment of patients with pseudarthrosis has been used for a long time, and its methods are being improved as science develops. For pseudarthrosis that formed after a closed fracture, at one time the method of choice was metal osteosynthesis with bone grafting.
After exposing the area, the pseudarthrosis is freed from scars and the bone fragments are refreshed, which, after reposition, are firmly fixed with a metal rod killed by the intramedullary. Then the area of pseudarthrosis is covered with a bone autograft, which is taken from the proximal metaepiphysis of the tibia or iliac wing; allografts (preserved cadaveric bones) or xenografts (bovine bone) are used. The graft is closely fitted with a spongy surface to the exposed layer of the pseudarthrosis area and firmly fixed with wire or bolts. The operation is completed by applying a plaster cast, which immobilizes the limb until the bone heals.
With tight pseudarthrosis without displacement of fragments, good results are achieved using a less traumatic operation - bone grafting with Khakhutov. After exposing the area of pseudarthrosis from the side of the subperiosteal wound, grafts of the same width are cut out from both fragments. Their length in one of the fragments should be 2/s, and in the second - 1/s of the total length of the graft. The grafts are moved so that the longer part covers the pseudarthrosis gap, and the shorter part fills the resulting defect after movement. After surgery, the limb is fixed with a plaster cast until the bone heals.
decortication surgery , has proven its worth . After opening all the soft tissues in the area of pseudarthrosis, thin plates of the cortex are knocked down with a subperiosteal chisel so that they are contained on the periosteum with the adjacent soft tissues. After performing circular decortication, the wound is sutured and a plaster cast is applied.
To stimulate reparative osteogenesis and improve blood supply to the pseudarthrosis area, some surgeons use a chisel to make incisions into the callus and bone to a depth of 2-3 mm in the form of a fir cone. The treatment of patients with infected pseudarthrosis complicated by osteomyelitis and after open fractures was very problematic. Treatment was delayed for many months and even years, since open surgical treatment can be carried out no earlier than 6 months after the healing of the festering wound or closure of the fistula.
To accelerate the healing of infected pseudarthrosis, the Steward-Bogdanov operation, or extrafocal bypass polysynostosis, was used, and for defects of the tibia, the Hahn operation was used - moving the fibula under the tibia.
Ilizarov apparatus into traumatological practice opened a new era, which radically changed the treatment tactics for pseudarthrosis, including those complicated by osteomyelitis and bone defects.
The use of hardware osteosynthesis eliminates deformation, creates stable fixation of the damaged segment, provides movement in adjacent joints, and allows loading the limb. However, with hypovascular pseudarthrosis, the process of bone fusion even in the apparatus remains slow, and therefore it is necessary to additionally apply bone grafting.
Patients with suppurative processes in the area of pseudarthrosis are treated according to the general rules of purulent surgery under conditions of hardware osteosynthesis.
For pseudarthrosis complicated by osteomyelitis , even when there is a fistula, the use of the device and the creation of stable fixation leads to increased regeneration, attenuation of the inflammatory process, closure of the fistula and bone fusion. If there is a formed sequestration, sequestrectomy is performed in the device or before its application. With the help of hardware osteosynthesis, it is possible to shorten the treatment period for patients and achieve bone fusion.
For bone defects, a 4-ring (or more) compression-distraction device is applied, a unipolar, and for large defects, a bipolar osteotomy (compactotomy) is performed in the metaphyseal (cancellous) area of the bone. After the formation of the primary cellular regenerate (7-10 days), the middle bone fragment begins to be lowered towards the defect. Lowering is carried out very slowly, 1 mm per day (in one or two steps of 0.5 mm), bringing the middle rings of the device closer together. As the space in the osteotomy area expands, it is filled with new regenerate and gradually grows.
When the ends of bone fragments approach each other at the site of the former defect, some compression is created to cause necrobiosis and stimulate the local reparative process and fusion of the fragments. For complete bone fusion, the device should be kept in a neutral position for 2.5-4 months. This treatment method allows you to eliminate bone defects over a significant area (15 cm or more).
How is shock wave therapy performed to treat delayed fracture consolidation?
In case of delayed consolidation of the fracture (non-union of the bone), the procedure is performed once every 7-10 days. At the Avatage Medical Center, doctors use special attachments that stimulate the formation of callus (stimulate osteogenesis). The impact is applied to the fracture area. Doctors at the Avatage Medical Center use their own patented methods for treating and preventing delayed fracture consolidation, based on the use of Storz Medical equipment. As the famous scientist Professor G. Ilizarov said: “Tensile tension is a powerful factor that activates tissue growth. According to this pattern, it is possible to stimulate the formation of new structural units of fibrous tissue, blood vessels, skin, and bones.” Taking this into account, we force muscles to contract and stretch using biomechanical stimulation (directed local vibration therapy), which trains the muscles and makes them work without making movements. This effect complements shock wave therapy and accelerates the process of bone healing.
What is the way out? What's new in the treatment and rehabilitation of fractures?
As it turns out, he is! Recently, an effective solution to this problem has emerged - shock wave therapy, a truly unique method of treating non-united fractures and pseudarthrosis. Over 10 years of treating PCP, specialists at Avatage MC have developed their own method for treating delayed consolidation of fractures and pseudarthrosis using Storz Medical equipment, which was patented. According to our data, the effectiveness of such treatment is 100%. All patients who came to our center were discharged with recovery - the formation of bone callus.
What is unique about shock wave therapy for bone nonunion?
The shock wave acting on tissue leads to stimulation of angiogenesis (the only method in medicine!). The flow of nutrients and oxygen increases to the area of injury. Tissue healing is accelerated. When exposed to bone, osteoblasts are activated, which begin the synthesis of bone tissue. As a result of the impact of shock wave therapy on the fracture area, callus formation and bone fusion occur. We also use the shock wave therapy method as a method of preventing delayed consolidation of fractures. Metal structures are not a contraindication for shock wave therapy procedures. More than 200 people were treated at the Avatage MC with a diagnosis of delayed consolidation of fractures or pseudarthrosis. All of them received bone fusion. 12 years of our own experience in the treatment of fractures and cooperation with leading departments of traumatology and orthopedics in Ukraine allowed us to create our own methods for the treatment and prevention of delayed consolidation of fractures and pseudarthrosis.