Hepatic encephalopathy
Therapy of hepatic encephalopathy is a complex task, and it must begin with eliminating the causes of this condition, treating acute or chronic liver failure. The treatment regimen for hepatic encephalopathy includes diet therapy, bowel cleansing, lowering nitrogen levels, and symptomatic measures.
The amount of protein consumed from food should be reduced to 1 g/kg/day. (provided that such a diet is tolerated by the patient) for a sufficiently long time, since in some patients a return to normal protein content causes the reappearance of the clinical picture of hepatic encephalopathy. During the diet, amino acid preparations are prescribed and salt content is limited.
To ensure effective excretion of ammonia in feces, it is necessary to achieve bowel movements at least twice a day. For this purpose, regular cleansing enemas are performed and lactulose preparations are prescribed (their intake must be continued at the stage of outpatient treatment). Ornithine and zinc sulfate also improve the utilization of ammonia.
Antibacterial therapy includes the prescription of broad-spectrum drugs that are active primarily in the intestinal lumen (neomycin, vancomycin, metronidazole, etc.). For sedative purposes in hepatic encephalopathy, it is undesirable to prescribe benzodiazepine drugs; preference is given to haloperidol.
The course of hepatic encephalopathy can be complicated by cerebral edema, bleeding, aspiration pneumonia, pancreatitis; therefore, treatment of patients at stages 3-4 of the disease should be carried out in the intensive care unit.
Prognosis and prevention of hepatic encephalopathy
The prognosis for hepatic encephalopathy depends on several factors, but is generally unfavorable. Survival is better in cases where encephalopathy develops against the background of chronic liver failure. In liver cirrhosis with hepatic encephalopathy, the prognosis worsens in the presence of jaundice, ascites, and low protein levels in the blood. In acute liver failure, the prognosis is worse in children under 10 years of age and adults after 40 years of age, against the background of viral hepatitis, jaundice and hypoproteinemia. Mortality at stages 1-2 of hepatic encephalopathy is 35%, at stages 3-4 – 80%. Prevention of this pathology consists of abstaining from alcohol and uncontrolled use of medications, treatment of diseases that lead to the development of hepatic encephalopathy.
Causes of hepatoencephalopathy in alcohol dependence
The basis of brain disorders in this disease is liver failure against the background of hepatitis caused by alcohol. Ethanol has a direct damaging effect on liver cells. Hepatocytes are destroyed and cease to perform a number of their basic functions. The acute process is especially dangerous when drinking large quantities of alcoholic beverages.
Malfunction of the liver leads to:
- accumulation of toxins selectively acting on neurons;
- changes in the acid-base properties of blood, hemostasis;
- deviations in the values of oncotic (created by plasma proteins) and hydrostatic pressure;
- disturbance of the electrolyte and water balance of the body.
These pathological processes cause inhibition of the function of astrocytes - cells that act as a natural defense between the tissues of the nervous system and blood.
As a result of the destruction of hepatocytes and astrocytes in the central and peripheral nervous system:
- Unneutralized poisons accumulate;
- electrolyte imbalance occurs;
- a malfunction of neurotransmitters—impulse transmitters—is formed;
- the production of cerebrospinal fluid (CSF) increases sharply, leading to a pronounced increase in intracranial pressure;
- There are increasing signs of cerebral edema.
The following has a particularly destructive effect on nervous tissue:
- ammonia;
- the appearance of false neurotransmitters - substances that replace the main mediators of the nervous system, which leads to insufficient functions of the latter;
- some types of fatty acids and amino acids.
Sources
- I. L. Klyaritskaya Hepatic encephalopathy. 2005. Crimean therapeutic journal;
- Polukhina A.V., Khaimenova T.Yu., Vinnitskaya E.V. Hepatic encephalopathy: the problem of pharmacotherapy. 2021. Medical Council;
- Ivanikov I. O., Syutkin V. E. Hepatic (porto-systemic) encephalopathy. 2003. Practical medicine;
- Podymova Svetlana Dmitrievna New approaches to the pathogenesis, clinical picture, treatment of hepatic encephalopathy. 2021. Therapeutic Archive;
- Tsapyak T. A., Klopotiy E. V., Viltsanyuk I. A. Hepatic encephalopathy and the possibilities of its drug correction. 2007. Crimean therapeutic journal;
- Polunina T. E., Maev I. V. Hepatic (porto-systemic) encephalopathy. 2011. Medical advice.
Video from YouTube on the topic of the article:
Clinical picture
Currently, there are three clinical variants of PE [2, 3]:
1. Subclinical encephalopathy
Subclinical PE is characterized by the absence of clinical symptoms, but additional studies reveal a number of neuropsychic disorders (deterioration of cognitive abilities, loss of fine motor skills, which can only be determined using psychometric tests). According to the literature, in patients with cirrhosis, subclinical PE is detected in 50–70% of cases. In patients with cirrhosis with portosystemic shunting, PE can be episodic with spontaneous resolution or intermittent, lasting many months or even years.
2. Chronic encephalopathy
This form of PE is divided into three stages (Table 2). In stage I, subtle personality changes, absent-mindedness, decreased attention, inability to concentrate, mild ataxia, and sleep disturbances are clinically observed.
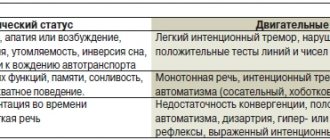
Stage II is manifested by fatigue, drowsiness, apathy, monotonous speech, inappropriate behavior with noticeable changes in the “structure” of the personality, disturbances in time orientation, the presence of intention tremor, reflexes of oral automatism, and ataxia.
Stage III PE is characterized by severe disorientation in time and space, incoherent speech, aggression, hypo- or hyperreflexia, pathological reflexes (Gordon, Zhukovsky), pronounced intention tremor, and muscle rigidity. With inadequate treatment of PE, hepatic coma may occur, which is characterized by a lack of consciousness and disappearance of reactions to painful stimuli. Rigidity of the muscles of the limbs and the back of the head, a mask-like face, and pathological reflexes (Babinsky, Gordon, Zhukovsky) are noted. Sometimes grasping and proboscis reflexes are detected [5].
In addition to psychoneurological symptoms, coma is characterized by clinical manifestations of hepatic cellular failure - jaundice, liver odor, ascites, hemorrhagic symptoms. The causes of death are cerebral edema, pulmonary edema, hepatorenal syndrome, infectious-toxic or hypovolemic shock.
3. Acute PE
It can develop in patients with severe jaundice against the background of ascites with severe necrotic processes in the liver, as well as in patients with fulminant liver failure. Acute HE may be accompanied by the development of hepatic coma.
Forms of the disease
Depending on the etiological factor, several types of hepatic encephalopathy are distinguished:
- type A – caused by acute liver failure;
- type B - caused by the release of neurotoxins from the intestines into the bloodstream;
- type C – associated with cirrhosis of the liver.
Based on the rate of increase in symptoms, hepatic encephalopathy is divided into two forms:
- acute – develops rapidly, accompanied by severe mental disorders;
- chronic – symptoms increase slowly over months, and sometimes even years.
What symptoms are typical?
Symptoms of hepatic encephalopathy:
- irritability;
- apathy;
- decreased performance;
- lethargy, even to the point of impaired consciousness;
- memory loss;
- nausea;
- sleep disturbance: drowsiness during the day and insomnia at night;
- dyspnea;
- fixed gaze;
- loss of interest in previously loved things;
- alternating irritability with an overly cheerful mood;
- writing disorder;
- impossible to complete simple tasks, for example, sequentially linking numbers (Reitan test);
- speech is slow and monotonous.
In the early stages of hepatic encephalopathy, patients may experience only minor changes in behavior, which others may attribute to the consequences of alcohol consumption:
- attention disorder
- lethargy and slowdown in performing daily routine activities,
- slowing down of psychomotor processes,
- increased irritability,
- emotional instability,
- aggression,
- difficulty performing small movements with your hands.
Diagnosis of hepatoencephalopathy
If the damage to the liver and brain is alcoholic, the doctor is interested in:
- symptomatic picture;
- establishing the severity of the disease;
- stage of the process.
Based on the data obtained, during a survey and examination, the doctor prescribes additional types of diagnosis of hepatic ecephalopathy.
These include:
- A detailed clinical blood test with determination of the content of erythrocytes, leukocytes, hemoglobin, platelets.
- Biochemistry data with liver tests, bilirubin, alkaline phosphatase, gamma globulin transferase.
- Ultrasound of the parenchymal organs of the abdominal cavity. The specialist is especially interested in the condition of the liver, pancreas, and kidneys.
- Computed tomography is the most informative method of x-ray diagnostics.
- MRI in doubtful cases, as an additional diagnostic method.
- Needle biopsy as the most accurate option for differential diagnosis.
Course, complaints and symptoms of hepatic encephalopathy in alcoholism
PE can occur in acute and chronic forms. The first develops over several hours or days. The second option is characterized by a slow course, sometimes lasting more than one year.
Stages of hepatic encephalopathy:
- Initial changes (compensation). Patients report sleep disorders, increased unmotivated irritability, attacks of apathy, and general loss of strength. Upon examination, the doctor determines the yellowness of the mucous membranes, and less often - the skin.
- Clinical manifestations (subcompensation). Mental problems are getting worse. They are accompanied by pronounced aggressiveness. Muscle (flapping) twitching during tension is detected - asterixis. The amplitude of these painful movements is wide and is observed both in the limbs and in the muscles of the neck and torso. Damage to the thermoregulation center results in periodic and unreasonable increases and decreases in temperature. There are violations of intellectual abilities. The patient becomes forgetful, cannot read and write, looks around him absent-mindedly and uncertainly. During certain periods, gaze fixation is observed. A specific sweetish (liver) odor emanating from the patient indicates a metabolic disorder.
- Terminal (decompensation). In this phase of the disease, disturbances of consciousness develop. Among the main symptoms is disorientation, the aggressiveness of which gradually reaches a soporous status. It is characterized by suppression of conscious functions, but preservation of reflexes. As a result of stupor, coma is formed - a completely unconscious state with complete inhibition of the reflex activity of the body, which is preceded by a convulsive syndrome. It is at this moment that most patients die.
Total information
Liver pathology is extremely rarely complicated by hepatic encephalopathy. However, if the disease is nevertheless detected, its outcome is almost always tragic: for 2/3 of those affected, encephalopathy ends in death. Chronic liver diseases are more often complicated by hepatic encephalopathy than acute ones. They are potentially reversible, but significantly affect the patient’s ability to work and lifestyle.
Modern medical science does not yet have a clear idea of the causes of the development of the disease, but recent research allows us to hope for a solution to this problem in the near future. Discovering the mechanisms of the disease will contribute to the development of an effective treatment plan that will not only reduce the number of deaths, but will significantly improve the quality of life of those affected.
Etiology
The main causes of the disease are:
- liver cirrhosis: this is the most unfavorable option, since according to statistics, within a year after the manifestation of encephalopathy, up to 50% of patients with cirrhotic damage to the hepatobiliary system die, and within 5 years - up to 80%;
- viral hepatitis B and C.
Risk factors include:
- old age and, accordingly, more severe liver disease;
- concomitant gastric ulcer and gastritis with an increase in the concentration of H. pylori (it is assumed that these gastrointestinal pathologies provoke increased production of ammonia);
- decreased motility of the large intestine;
- excessive consumption of protein;
- alcohol consumption, long-term use of hepatotoxic drugs (in particular, antitumor drugs, immunosuppressants, etc.), diuretics;
- chronic metabolic and electrolyte disorders associated with any severe fever, inflammatory process (including an autoimmune nature).
Hepatic encephalopathy caused by pathology of the hepatobiliary system is called “true” or “endogenous”. It develops as a result of necrosis of most of the liver parenchyma and, as a consequence, a decrease in its detoxification function. However, in some cases, due to irreversible changes, shunts (a kind of “alternative” vessels) are formed between the portal and general circulatory systems. As a result, toxic metabolic products enter directly into the systemic bloodstream and, accordingly, into the brain, bypassing the liver. This form of the disease is called portosystemic.
Neurological symptoms of the disease develop due to the influence of the following factors:
- Accumulation of endogenous neurotoxins (ammonia, mercaptans, phenols, etc.).
- Violation of the synthesis and balance of amino acids.
- Imbalance of neurotransmitters (in particular, decreased levels of dopamine and norepinephrine, increased concentrations of serotonin and γ-aminobutyric acid).
- Increased activity of benzodiazepine receptors.
- Increasing the permeability of the blood-brain barrier to toxic substances.
- Pathologies of energy metabolism.
But the leading role in pathogenesis is played by the influence of ammonia , one of the strongest neurotoxic metabolites. Normally, the synthesis of this compound occurs in the liver as a result of the biochemical transformation of amino acids; in much smaller quantities it is formed in the muscles, kidneys and digestive tract.
But the liver is not only the main “source” of ammonia, but also the organ where its neutralization occurs due to the synthesis of urea, glutamine and other compounds. Accordingly, the more serious the damage to the hepatobiliary system, the higher the ammonia level.