Perforation of the eardrum (in the ear), treatment at the City Med Clinic Orenburg
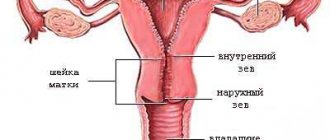
The eardrum is a thin multi-layered membrane that separates the ear canal from the middle ear cavity. The role of this membrane is to transmit sound waves (air vibration) to the hammer, which then travel to the auditory ossicles of the inner ear. Thus, the eardrum is an important element of the acoustic system that the ear represents. In cases where a hole or rupture appears in the eardrum, the conduction of sounds is disrupted, which, accordingly, impairs hearing. In addition, when the membrane is perforated, a kind of barrier disappears, which does not allow pathogens - bacteria, viruses and fungi - to penetrate into the middle ear.
Causes of perforation
Among the causes of eardrum ruptures are the following:
- inflammatory diseases of the middle ear (otitis media), in which purulent melting of the membrane can occur, as well as its thinning under the influence of pressure from the inflammatory exudate;
- barotraumas that occur when the pressure in the external auditory canal or in the tympanic cavity increases (when sneezing with a closed nose, falling on the ear, during a sharp decrease or gain in altitude by an airplane, with a sharp blow to the ears, tests in pressure chambers, in divers, while in zone of action of a shock wave during explosions, during jumps into bodies of water from a great height, etc.);
- noise injury that occurs when exposed to sudden intense noise (for example, during an explosion);
- mechanical damage to the eardrum by foreign bodies, in case of ear injuries (bullet and shrapnel wounds, cleaning the ears with sharp objects not intended for this purpose, traumatic brain injuries with fractures of the temporal bone, etc.);
- chemical damage (caustic chemical compounds, alkalis, acids, etc.);
- significant thermal damage (burn in an industrial environment with the death of a section of the eardrum and its perforation).
Symptoms of perforation of the eardrum When the eardrum ruptures, there is usually sudden intense pain in the damaged ear, which is often accompanied by dizziness, tinnitus, bleeding from the ear and deafness. Then the pain syndrome may subside, but mucous, purulent or bloody discharge from the affected ear is noted, as well as the release of air from the ear when sneezing and blowing the nose.
Tympanitis, or otitis media of the middle ear
Fungus
Cold
2767 08 October
IMPORTANT!
The information in this section cannot be used for self-diagnosis and self-treatment.
In case of pain or other exacerbation of the disease, diagnostic tests should be prescribed only by the attending physician. To make a diagnosis and properly prescribe treatment, you should contact your doctor. Tympanitis - causes, symptoms, diagnosis and treatment methods.
Definition
Tympanitis is a purulent-inflammatory disease of the ear, affecting the mucous membrane of the tympanic cavity, characterized by a chronic course, perforation of the eardrum. Tympanitis is considered to be a type of acute or chronic otitis media of the middle ear.
Causes of tympanitis
The cause of tympanitis is the penetration of infection from the nasal part of the pharynx through the auditory tube (tubar tract), with the flow of blood (hematogenous tract) or lymph (through lymphatic vessels), as well as through an injured eardrum. The causative agents of the inflammatory process are considered to be pneumococci, streptococci, and less commonly, E. coli, etc. Combined infection with several types of bacteria and fungi is possible.
The occurrence of acute inflammation of the middle ear is facilitated by diseases of the upper respiratory tract, the presence of adenoids, chronic inflammatory diseases of the nasal cavity and paranasal sinuses, intensive attempts to blow out mucus during infectious or allergic pharyngitis, and a general weakening of the body's defenses.
At risk are patients with metabolic disorders (for example, diabetes), with a history of traumatic brain injury, pregnant women, as well as with immunodeficiency conditions and blood diseases. Among the reasons for the development of tympanitis, the resistance of pathogenic microorganisms to antibiotics that were previously used is noted.
With systematic purulent discharge from the ear cavity, in the presence of perforation of the eardrum, and progressive hearing loss, they speak of chronic tympanitis.
The disease often appears in childhood, which is associated with the anatomical characteristics of the child’s body. In children, the Eustachian tube (auditory tube), which connects the nasal passages to the ear, is shorter and wider than in adults and is more horizontal. Therefore, an infection that gets into the nose or nasopharynx easily penetrates the ear.
Classification of tympanitis
Tympanitis has two forms of the disease:
- Mesotympanitis, when inflammation covers the lower and middle parts of the tympanic cavity; Usually the disease is characterized by perforation of the central part of the tympanic septum, the presence of odorless purulent discharge, and hearing loss.
- Epitympanitis (total otitis), when inflammation affects not only the middle ear, but also surrounding tissues. With epitympanitis, marginal perforation of the eardrum occurs, purulent discharge becomes thick and has a pungent odor. Epitympanitis has purulent-carious and cholesteatoma forms.
According to the course of the disease, acute and chronic tympanitis are distinguished.
Symptoms of tympanitis
Symptoms of tympanitis and the clinical picture depend on the form of the disease and the stage of its development.
In most patients, mesotympanitis begins with a gradual unilateral deterioration of hearing. Then intoxication occurs, which is characterized by an increase in body temperature to 39.0°C, chills, weakness, aching headache, and drowsiness. Following this, purulent mucous discharge from the ear (otorrhea) appears. Otorrhea is often accompanied by a feeling of fullness in the ear, distortion of the perception of one's own voice, and pain. With significant damage to the eardrum, there is a constant noise (hum) in the ears. Perforation of the tympanic membrane can be central or marginal, when the prerequisites for the development of cholesteatoma are created.
During otoscopy, an accumulation of purulent discharge and perforation of the eardrum are observed in the ear canal. The membrane itself is thickened and hyperemic due to an increase in its blood supply.
The purulent-carious form of epitympanitis is characterized by destructive changes in the bone of the lateral (side) wall of the attic, which, if left untreated, spread to the mastoid process. In this case, purulent discharge from the ear with a putrid odor is observed. At this stage, there may not yet be a pronounced hearing loss; hearing loss occurs later, as a result of caries (destruction) of the auditory ossicles.
In the case of proliferation of epidermal tissue and inclusion of the bone walls of the ear canal in the process, a neoplasm is formed - cholesteatoma. It resembles a tumor and, if left untreated, can reach impressive sizes.
For a long time, cholesteatoma can manifest itself only as a headache.
It is not easy to determine tympanitis in a small child, since he cannot yet tell where and how it hurts. The following symptoms may be observed: the child is restless, periodically cries loudly for no apparent reason, refuses to eat, as the pain intensifies when swallowing and sucking. The temperature rises to 39-40°C, and there may be vomiting and diarrhea (diarrhea). In an infant, pay attention to the position of the head; it will be tilted in the direction where it hurts.
Diagnosis of tympanitis
To diagnose tympanitis, a doctor can use the following research methods:
— instrumental research methods:
- otoscopy (examination of the eardrum, and if it is destroyed, the tympanic cavity using an otoscope);
- audiometry (a hearing test using a tuning fork allows you to measure hearing acuity, determine auditory sensitivity to sound waves of different frequencies, and determine sound conduction on the side of the affected ear);
- tympanometry (study of the function of the middle ear, the degree of mobility of the eardrum and the conductivity of the auditory ossicles using air pressure in the ear canal);
- X-ray to determine the condition of the bone tissue of the mastoid process;
Diagnosis of eardrum perforation at City Med
Endoscopic examination of the ear is the main method for diagnosing this pathology and is often quite sufficient. It includes otoscopy and microotoscopy, which are performed by an otolaryngologist. The study is carried out using an ENT machine, which allows you to visualize defects in the eardrum, hemorrhages, the presence of pus, and also take pathological discharge for bacteriological analysis in order to determine the causative agents of infection and their sensitivity to antibacterial drugs. If necessary, our clinic uses additional research methods: audiometry, tympanometry, stabilography, tuning fork examination, electrocochleography, acoustic impedance measurement, caloric test, vestibulometry.
Treatment of eardrum perforation
Therapeutic tactics depend on the nature of the damage to the eardrum. Thus, in case of mechanical damage by a foreign body, it is necessary to remove it (if necessary) and disinfect the wound to prevent secondary infection. If perforation occurs against the background of an already existing inflammatory (purulent) process, antibiotic therapy is prescribed. Surgical closure of the tympanic membrane defect is performed in case of extensive damage or when conservative treatment methods are insufficiently effective. There are mainly two types of surgical interventions used: myringoplasty and tympanoplasty. The material used to close the defect can be fascia of the temporal muscle, chick amnion, meatotympanic flap, or skin graft. Complications are usually caused by perforations exceeding 25% of the area of the eardrum, infected perforations and accompanied by damage to the auditory ossicles. Complications may include the development of mixed or conductive hearing loss, chronic and recurrent inflammatory processes, adhesive otitis media, and disability due to complete hearing loss. To prevent perforation of the eardrum, it is recommended to promptly consult a doctor if symptoms of inflammatory processes in the ear, hearing loss, etc. appear, and also to avoid exposure to sudden changes in pressure, loud noises, and mechanical injuries.
Parotid fistula: what is the danger of an additional canal in the ear
Parotid fistula is a rather unpredictable disease. In some cases, the anomaly may not bother a person throughout his life, but sometimes it makes itself felt immediately after birth and threatens with serious complications. When surgical treatment is necessary, and when surgery can be avoided, said otorhinolaryngologist at the Morozov Children’s Hospital with 25 years of experience in treating the disease, candidate of medical sciences, holder of the “Moscow Doctor” status, Alexander Mikhailovich Ivanenko.
How does the anomaly manifest itself?
Externally, a parotid fistula looks like a barely noticeable point at the helix of the auricle. With an atypical location, the mouth can be located anywhere in the auricle, including the lobe. But this is very rare. The fistula itself is an additional passage covered with skin measuring 1.5 - 2 cm in length, which has a tortuous structure. Sometimes the fistula bifurcates or ends in a thick cyst-like extension. It can form in one ear or in two at the same time.
What are the causes of the disease?
Congenital parotid fistulas are the most common developmental anomaly of the external ear. Occurs in 15 - 43 children per 100,000, depending on the region. In 30% the disease is hereditary, in 70% it is sporadic, that is, it occurs from time to time. The appearance of a fistula is associated with abnormalities in fetal development. The defect forms at 9-11 weeks of intrauterine development. At this time, six ear tubercles are formed from the I and II gill arches, from which the structures of the auricle subsequently develop. Pathological processes during pregnancy (stress, respiratory diseases) lead to the occurrence of a defect.
Why is parotid fistula dangerous?
The fistula canal is lined with skin containing sweat and sebaceous glands, so contents of a yellow-curdled consistency accumulate and are periodically released. When a bacterial infection occurs, an inflammatory process develops that spreads to soft tissues. Huge pyogenic ulcers form on the skin, reaching 5 cm in diameter. A cosmetic defect significantly reduces the child’s quality of life. If the inflammatory process involves the cartilage of the auricle, perichondritis occurs, which leads to deformation of the auricles.
It happens that a congenital anomaly is misdiagnosed, mistaking it for other diseases: atopic dermatitis, eczema, osteomyelitis, skin tuberculosis and even systemic lupus erythematosus. Often children come to us after long but ineffective treatment.
Can parents independently detect a parotid fistula in a child?
In most cases this is possible. It is necessary to carefully examine the child and understand whether he has a small hole at the base of the ear curl or not. If there is a hole, but it looks like a small needle puncture and does not bother the child, there is no need to worry. The fistula is not dangerous and does not need to be removed. If the mouth is red, secretions are released from the hole, discomfort or pain appears - it is necessary to treat the mouth with a chlorhexidine solution and consult an otolaryngologist.
How is a congenital anomaly treated?
As a rule, patients come to us for the first time with an exacerbation of the disease. We treat the abscess and schedule a planned operation to remove the fistula. Surgical removal is performed only in the cold period, that is, not in the active phase of inflammation. Otherwise complications may arise. It takes about one and a half months to restore the skin after the inflammatory process is removed.
There are no age restrictions for the intervention. Our youngest patient was only three months old. Since birth, his fistula has become inflamed twice.
How is the operation performed?
The point of surgical treatment is to completely remove the entire fistulous tract. At the same time, the surrounding tissues cannot be damaged. A method based on the property of diaphanoscopy helps to recognize and highlight the pathological zone. My colleagues and I developed and patented the method several years ago, and we successfully apply it in practice.
During the operation, a sterile light guide catheter with a diameter of 0.75 mm is inserted through the mouth into the fistula canal. The catheter lights up and we accurately assess the length, shape and direction of the fistula, and the presence of possible branches. Then we gradually isolate the fistula from the surrounding tissues. The operation lasts from 40 minutes to an hour. This is a low-impact intervention. Previously, children spent 7-10 days in the hospital after surgery, but now they are discharged after 3-4 days. There is no need to remove sutures - we use absorbable suture material. If a child has a bilateral fistula, we remove the pathology from both sides at the same time.
We perform 20 to 30 such operations annually. Over the past years, vast experience has been accumulated in effective surgical treatment of congenital anomalies.